Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2014) Volume 4, Issue 3
Objective: This pilot trial explored the influence of static magnetic fields imbedded in a wrist-hand fitment on nerve conduction and symptom reports in persons with carpal tunnel syndrome (CTS) to determine if the active magnetic wristhand fitment would improve objective and subjective symptom measures versus the sham control.
Methods: Randomized, sham-controlled, pilot trial involving participants with CTS (N=26) who wore either an active magnetic wrist-hand fitment or a sham fitment for 8 to10 hours a day for 8 weeks. Outcome measures included changes in nerve conduction and weekly symptom ratings.
Results: The active magnetic fitment group showed significant improvement in motor nerve conduction latency (p=0.046) and a trend toward improvement in sensory latency (p=0.090) compared to the sham group. Objective measures of motor and sensory nerve conduction improved in the active group compared to the sham group, while there were no differences between groups for subjective reports of symptom and functional measures, with both groups showing improvement over time.
Conclusion: Findings of improvement in motor distal latency, with only a trend toward improvement in sensory latency, still leave healthcare professionals without sufficient information to inform patients that static magnetic fields are either effective or ineffective in the management of symptoms related to CTS.
Keywords: Permanent magnets; Magnetic fields; Carpal tunnel syndrome; CTS; Cumulative trauma to wrist; Wrist-hand fitment; Pain; Nerve conduction latency
Cumulative trauma disorders such as carpal tunnel syndrome (CTS) involve injury to soft tissue (i.e., nerves and/or tendons, ligaments, vascular structures). Repetitive and excessive motion in the involved area over a long period of time is thought to cause microtears, inflammation, and eventual degeneration of tendons and ligaments, leading to alterations in the synovial fluid. Inflammation produces swelling that may cause compression of the median nerve as it traverses the confined space known as the carpal tunnel [1]. Symptoms are expressed as numbness, tingling, pain, and frequent nocturnal discomforts that prompt affected individuals to seek medical treatment. Hand weakness and clumsiness, in combination with the other symptoms, often interfere with job performance and activities of daily living [2,3].
The incidence of carpal tunnel syndrome is 1-3 cases per 1000 subjects per year, with the prevalence approximately 50 cases per 1000 subjects in the general population. Incidence may rise as high as 150 cases per 1000 subjects per year, with prevalence rates greater than 500 cases per 1000 subjects in certain high-risk groups [4]. Carpal tunnel release is performed about 400,000 to 500,000 times a year and generally results in relief of symptoms and improvement; however, this surgical procedure may fail for several reasons, leading to recurrence of CTS and need for further surgery [5]. Conservative treatment for repetitive motion trauma includes splinting the affected joint, use of anti-inflammatory agents, vitamin B-6 (pyridoxine) supplementation, steroidal injections, changing duties in the workplace, and ergonomic adjustments of equipment [6]. However, given that these treatment options sometimes do not provide symptom relief or return of functionality, more effective and cost-efficient treatment strategies are needed [7].
One noninvasive treatment that some believe worthy of exploration despite mixed reviews is the use of permanent magnets and other sources of static magnetic fields. An early review of magnetic therapy research conducted in Europe [8] reported clinical improvements in patient populations, including individuals with rheumatoid arthritis, cervical osteoarthritis, and CTS. Although the number of published studies since that time testing the efficacy of static magnetic fields is small, preliminary findings from some of these studies suggest the potential for promising applications of this modality in selected populations. Randomized, controlled trials using static magnetic fields (SMFs) have demonstrated effectiveness in reducing neuropathic pain in certain populations [9-13]. These studies were followed by a systematic review and meta-analysis of randomized trials using static magnets for reducing pain that led the British reviewers to conclude that although evidence was insufficient to exclude clinically important benefits, evidence was not sufficient to support the use of static magnets for pain relief [14]. A Cochrane review led by Kroeling and colleagues [15] evaluated the effectiveness of magnetic therapies, including the effectiveness of permanent magnets (in necklaces) for neck pain, with the authors reporting that the evidence quality was low and that further study was needed. A recent critical literature review on use of static magnet therapy for the relief of pain and discomfort [16] concluded there is a benefit to using static magnets for pain given that beneficial health outcomes can be influenced by positive expectation, leading health professionals to conclude that, although there is much more to understand about magnets, even more understanding is needed about expectations of outcomes in many therapies.
In earlier research conducted in our center using magnetic sleep pads with persons suffering from fibromyalgia, approximately 45% of participants reported a reduction in pain and an improvement in functional status [17,18]. No adverse effects were reported in these studies. It is important to note that many studies of the effects of SMFs have failed to describe fully the strength and configuration (the “dose”) of the magnets used (e.g., placement site, distance from and flux density within the target tissue); thus, results often cannot be compared or reproduced [9,19]. Important questions remain unanswered concerning the mechanism whereby magnetic devices may produce beneficial effects [20]. Although the evidence of a biological effect is greater for electrical stimulation and pulsed electromagnetic stimulation than for SMFs [6], there are data supporting the biological effects of SMFs. Exposure to a quadra-polar SMF caused reversible blockage of action potential firing and reduction of responses to the pain-producing substance capsaicin in adult dorsal root ganglion cells in vitro [21-23]. Low level static fields (10-100 mT) can produce local, significant arteriolar vasodilation and increased peripheral blood flow in skeletal muscle within 15 min, possibly as a result of the modulation of intracellular Ca2+ concentrations [24-27]. These results imply that SMF exposure influences arteriolar diameters, and therefore microvascular tone, in a restorative fashion, acting to normalize the tone somewhat, which influences tissue perfusion. Thus, SMF application could be efficacious for the treatment of both ischemic and edematous tissue disorders involving compromised microvascular function [25], such as CTS.
Low intensity magnetic fields have shown beneficial biological effects without evidence of adverse effects. For example, very weak (μT range) physiologically-patterned magnetic fields have been shown to synergistically interact with drugs to potentiate effects that have classically involved opiate, cholinergic, dopaminergic, serotonergic, and nitric oxide pathways. The combinations of the appropriately patterned magnetic fields and specific drugs can evoke changes that are several times larger than those evoked by the drugs alone [28]. There also is the potential for new therapies based on the vascular neurological response to magnetic fields [26].
Given the reported effects of magnetic fields on pain, edema reduction, and nerve firing, it is conceivable that magnetic fields may help alleviate pain and symptoms in persons with CTS or other cumulative trauma-related wrist or hand injuries. Thus, the purpose of the current study was to determine the effects of magnetic wristhand fitments on symptoms of CTS using both objective and subjective measures in a randomized, sham-controlled, double-blinded study. We hypothesized that the active magnetic wrist-hand fitment would improve objective and subjective symptom measures versus the sham control fitment.
Study subjects
The University of Virginia Institutional Review Board for Health Sciences Research approved the study protocol, monitored enrollment progress, and provided oversight of data management and adverse event monitoring. The study coordinator explained the study rationale and protocol to potential participants and obtained written informed consent. Sixty adults with symptoms of CTS were recruited through the Physical Medicine and Rehabilitation Clinic at the University of Virginia Health System, Charlottesville, Virginia, and through flyers and advertisements in local newspapers for an 8-week study of the effects of wearing a magnetic wrist-hand fitment. Participants were screened for the inclusion and exclusion criteria of the study. Inclusion criteria were: (1) history of numbness, tingling, pain, and/or weakness in median nerve distribution; (2) clinical symptoms of CTS, including decreased sensation (complete or partial)of the first 3.5 digits (index finger [first digit], middle finger [second digit], ring finger [third digit], little finger [fourth digit]); abnormal values of 2-point discrimination (>6 mm); compression maneuvers (Tinel’s and Phalen’s) positive at the wrist with radiation into the first 3 digits (index finger, middle finger, ring finger); and/or weakness of thumb abduction and opposition; (3) abnormal electrodiagnostic results on at least two of the three following tests (described below): (a) between median and ulnar sensory distal latencies; (b) median and radial sensory distal latencies; and (c) median and ulnar motor distal latencies (maximal acceptable latency differences were 0.4 milliseconds (ms), with the median nerve conduction being the slowest); and (4) a normal mixed median forearm conduction test to rule out the presence of peripheral neuropathy. Exclusion criteria included pregnancy, use of opioids, currently using wrist splints during the day, and receiving Workers’ Compensation for CTS.
Study protocol
Baseline Symptom Severity Scale (SSS), Functional Status Scale (FSS), and nerve conduction tests were completed (see Measures), and participants were randomized to one of two groups: active magnetic wrist-hand fitment or sham fitment. Randomization was accomplished using a computer-generated assignment list and was masked (using envelopes). That is, the next available assignment number was not revealed until it was required. Participants were instructed to wear the fitment on the more symptomatic hand (“study hand”) for 8 to10 hours a day for 8 weeks. Previous studies have shown that neurological pairing of hands (using each hand as an independent sample) leads to high correlations of responses in left or right hands [12], which is problematic when interpreting study results. Although both hands are involved in approximately 50% of patients, symptoms are usually worse in one hand. Participants recorded daily fitment wear time and rated weekly symptoms of pain, numbness, weakness, and tingling using numeric rating scales. Participants were instructed not to alter their medications or treatments for CTS during the study period. At 8 weeks, participants had post-study nerve conduction tests on the study hand and completed follow-up SSS and FSS measures. All outcome assessors, including the physician (third author) performing the electrodiagnostic testing, as well as those individuals responsible for data analysis, were blinded to participant allocation until the completion of data analyses.
Electrodiagnostic testing: Electrodiagnostic testing was performed to confirm the diagnosis of CTS and as an objective outcome measure of the intervention. Electrodiagnostic testing measures latency, the time it takes for an electrical impulse to travel from one point to another, measured in milliseconds. When several areas of a nerve are stimulated, such as when testing the mixed median nerve, the differences between the impulse travel times (latency comparisons, subsequently referred to as latency) can be calculated to determine a pattern of nerve damage or compression [29]. Conduction velocity was determined in the current study by dividing the distance (cm) from the point of stimulation to the recording electrodes by the latency from the point of stimulation to the onset of the response (ms). During the electrodiagnostic testing, hand temperature was kept at a minimum of 30°C measured at the fingertip of digit 3 (ring finger). The assessments performed are described below. The electrodiagnostic studies were performed using a Keypoint (Medtronix USA Imaging Systems, Palmdale, CA) electromyograph.
Median-radial sensory nerve latency comparisons [30]: Ring electrodes were placed around the thumb, and stimulation was carried out over the median nerve at the wrist, followed by stimulation of the radial nerve over the lateral distal forearm (radial nerve), both 14 cm proximal to the recording electrodes. The stimulus current was increased to ensure maximal nerve recordings in both median and radial responses. Measurements were from stimulus to onset of the evoked response, and amplitude measurements were from baseline to peak duration from onset of the waves to return to baseline.
Median-ulnar sensory nerve latency comparisons [31,32]: Ringelectrodes were placed around digit 4 (little finger), and stimulation was carried out 14 cm proximal to the recording site at the median nerve and then at the ulnar nerve of the wrist. Measurements were conducted as for the previous test.
Median-ulnar motor nerve latency comparisons [32-34]: A superficial disc recording electrode was placed in the palm over the distal crease at the web space between digits 2 (middle finger) and 3 (ring finger), with the reference electrode over the proximal interphalangeal joint of digit 1 (index finger). Stimulation again was carried out at the wrist over the median and ulnar nerves, both 10 cm proximal to the recording site.
Mixed median forearm conduction velocity [35]: This test was used to rule out peripheral neuropathy and therefore had to be normal (57.4 ± 4.0 microns/step in our clinic) for the subject to qualify for the study. The diagnostic test was performed by placing a bar electrode over the median nerve in the antecubital fossa, medial to the biceps tendon (point of median nerve stimulation in routine conduction studies). Stimulation was carried out at the wrist over the median nerve, locating the cathode proximal. Conduction velocity was determined as described above.
Outcome measures:
Symptom Severity Scale (SSS) and Functional Status Scale (FSS): The SSS and the FSS are self-administered questionnaires [36] for the assessment of symptom severity (11 items) and functional status (8 items) for individuals with symptoms of CTS (reproducibility = 0.91 for SSS and 0.93 for FSS; internal consistency = 0.89 for SSS and 0.91 for FSS). These measures were assessed at baseline and at study completion.
Weekly symptom reports: Symptoms of pain, numbness, weakness, and tingling were rated once a week for the duration of the study using individual 11-point numeric rating scales (0−10). Numeric rating scales were used because these scales are more user friendly across the spectrum of study participants than visual analog scales.
Magnetic wrist-hand fitment: Mag-Na-Prene (Orion Medical Group, Reno, NV) wrist-hand fitments constructed of neoprene that incorporated rare earth magnets were used. The fitment was a flexible rectangle weighing 35.4 g with a cutout for the thumb, which allowed movement of the wrist. The fitment covered both the front and back of the hand and the wrist, and was secured with Velcro straps (Figure 1). The active fitments had permanent magnetic threads incorporated into the neoprene in parallel rows, resulting in the expression of alternating polarity fields. Maximum measured flux densities were ± 4 mT at a distance of 2 mm and ± 0.5 mT at a distance of 10 mm from the surface of the active fitments. Sham fitments appeared identical to active fitments but did not have magnetic threads incorporated into the neoprene. The measured flux densities were all <100 μT for the sham fitments at all distances from the surface. Figures 2 and Figure 3 display diagrams of how the flux densities varied with the vertical position over the surface of the active fitment. These spatial distribution measurements were made with a three-dimensional calibration system that motorizes the movement of a gaussmeter probe through a specified volume. Each fitment was placed flat on the calibration stage with the skin side facing up, and a 4 cm × 4 cm × 1 cm volume, corresponding to that part of the fitment that would overlay the carpal tunnel area, was assessed. The scanning interval of the flux density measurements was 2 mm. The two-dimensional plots created are shown in Figures 2 and Figure 3 at elevations of 2 mm and 10 mm, respectively, from the surface of the fitment, illustrating the distribution of the magnetic flux density at those particular tissue depths during exposure. This is important as it accurately indicates the mT level experienced by the carpal tunnel area of the participants.
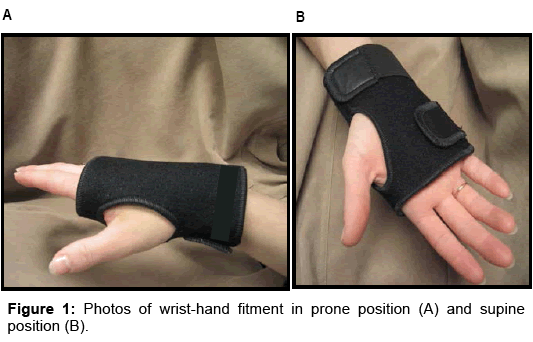
Figure 1: Photos of wrist-hand fitment in prone position (A) and supine position (B).
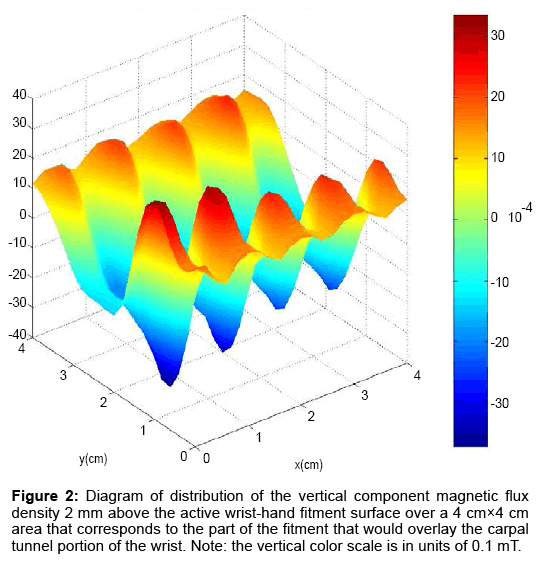
Figure 2: Diagram of distribution of the vertical component magnetic flux density 2 mm above the active wrist-hand fitment surface over a 4 cm×4 cm area that corresponds to the part of the fitment that would overlay the carpal tunnel portion of the wrist. Note: the vertical color scale is in units of 0.1 mT.
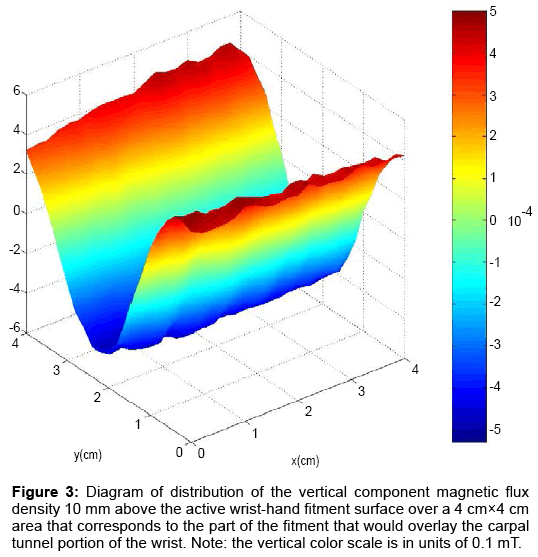
Figure 3: Diagram of distribution of the vertical component magnetic flux density 10 mm above the active wrist-hand fitment surface over a 4 cm×4 cm area that corresponds to the part of the fitment that would overlay the carpal tunnel portion of the wrist. Note: the vertical color scale is in units of 0.1 mT.
The calibration system consisted of four translation stages, three of which were motorized (BiSlide Assemblies, Velmex, Bloomfield, NY, 0.01 cm resolution), a controller for these (VP9000 Series, Velmex), a gaussmeter (Model 6010 Hall-effect gaussmeter, F.W.Bell, Orlando, FL, accuracy 0.25%), and gaussmeter probes (Model STD61-0202-15, UltraThin Transverse Probe and Model HAD61-2508-15, Axial Probe, F.W. Bell), both with linear accuracy of 0.5% and sensor areas of 0.013 and 0.46 mm2, respectively. The system was controlled by a LabVIEW program (National Instruments, Austin, TX) and had an overall measurement sensitivity of 0.1 μT. The host computer orchestrated the movement of the stages and the measurements of flux density. The user input the desired distance to be traversed as well as the desired step increment in each axis. The flux density measurements as well as x, y, and z coordinates were recorded at each increment and archived in a MS Excel spreadsheet.
Data were analyzed using SPSS (version 19; IBM, Armonk, NY). Separate ANCOVA models were used to analyze differences between the groups for the electrodiagnostic results and the subjective outcomes of SSS, FSS, pain, numbness, weakness, and tingling at 8 weeks, with the appropriate baseline outcome measure used as the covariate. Data were normally distributed. Given that this was a pilot study, statistical significance (p < 0.05) and trends (p < 0.10) were examined for all tests.
Sixty persons with CTS were contacted for the study. Seven could not be contacted further following their initial interest in the study. Of the remaining 53 potential participants, 13 did not meet the inclusion criteria. Of the remaining 40 potential participants who consented to have electrodiagnostic testing performed to determine eligibility, 10 did not demonstrate the required nerve conduction abnormalities and 1 had peripheral neuropathy, leaving 29 randomized into the two groups (active group = 15 and the sham group = 14; Figure 4). Four participants dropped out of the study after baseline (Figure 4) and their data were excluded, leaving 25 participants for inclusion in data analyses. The participants had a mean education level of 14.8 ± 2.1 years, and the majority were female (88%) and White (68%). There were no significant group differences in demographic variables (Table 1).
| Variables | Active magnetic fitment | Sham fitment |
|---|---|---|
| Mean (SD) | Mean (SD) | |
| Age (years) | 57.1 (10.7) | 50.4 (11.8) |
| Education (years) | 15.1 (2.3) | 14.4 (1.9) |
| n (%) | n (%) | |
| Gender Male Female |
2 (14.3) 12 (85.7) |
1 (9.1) 10 (90.9) |
| Race Non-minority Minority |
9 (64.3) 5 (35.7) |
8 (72.7) 3 (27.3) |
Table 1: Demographic characteristics by group.
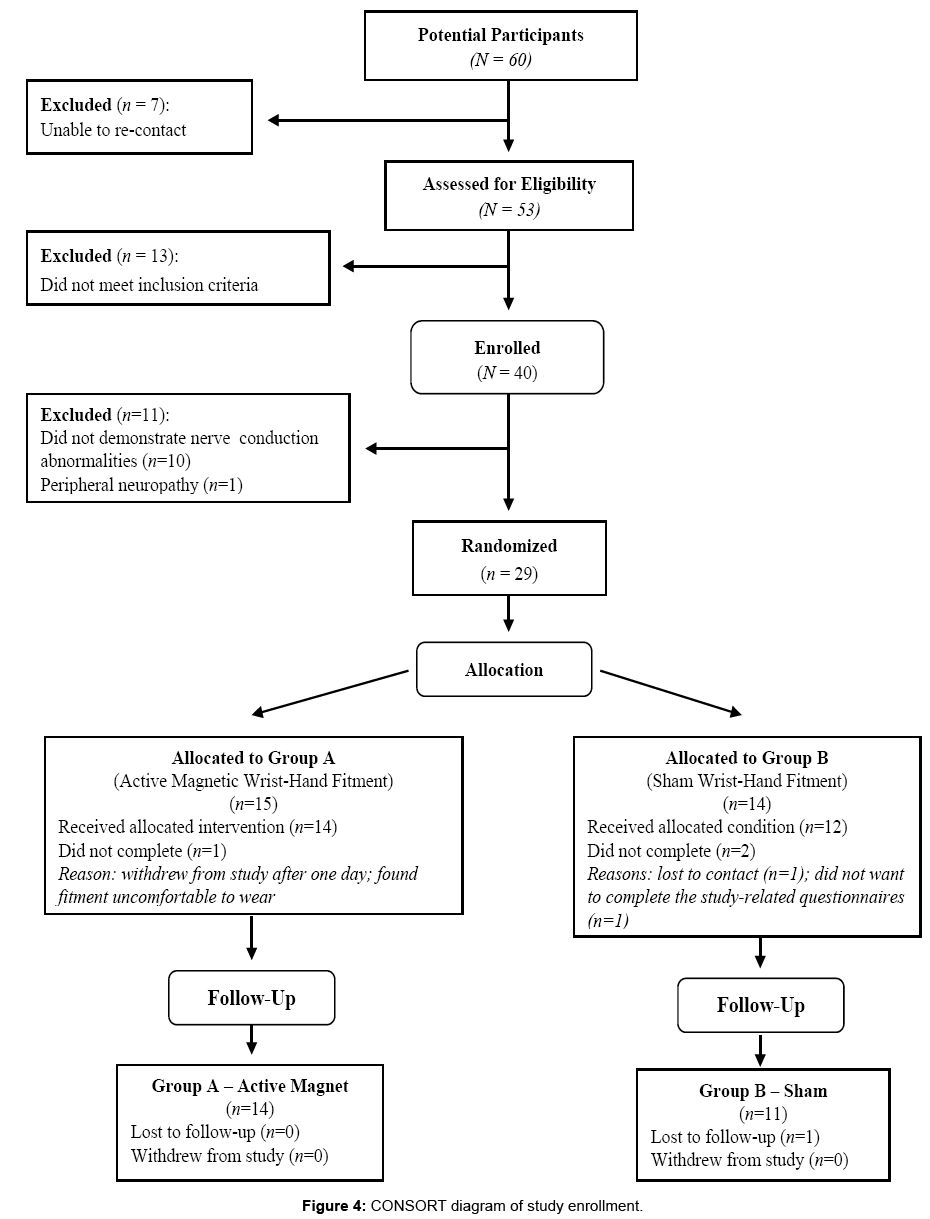
Figure 4: CONSORT diagram of study enrollment.
Baseline symptoms described by the participants were numbness (n = 23), tingling (n = 25), pain (n = 20), weakness (n = 19), nocturnal discomforts (n = 22), and significant interference with daily activity (n = 9). Clinical pathologies of CTS noted during the physical exam were weakness of thumb abduction and opposition, decrease of sensation in the first 3.5 digits (or part of these), and/or compression maneuvers (Tinel’s positive only in 4 subjects, and Phalen’s positive in 7 subjects) at the wrist, with radiation into the first 3 digits. All participants were able to discriminate two discrete points 6 mm apart during the 2-point discrimination test.
Regarding the hand that participants identified as their dominant hand and the one on which they wore the fitments, in the active magnetic wrist-hand fitment group (n = 14), 9 (64.3%) identified the dominant hand as worse, 1 (7.1%) the non-dominant hand as worse, and 4 (28.6%) did not identify a dominant hand. In the sham fitment group (n = 11), 5 (45.4%) identified the dominant hand as worse, 3 (27.3%) the non-dominant hand as worse; and 3 (27.3%) did not identify a dominant hand. There were no differences in total fitment wear time between the sham (mean = 440.55 ± 49.00) and active (mean = 437.92 ± 29.51) groups (independent t-test = 1.66, p = 0.87).
Electrodiagnostic results
After controlling for baseline median-ulnar motor latency, the active magnetic fitment group had a significantly lower median-ulnar motor nerve conduction latency at post-treatment than the sham group (p = 0.046), indicating improvement in the active magnetic fitment group (Table 2). The active group also showed a decrease in the sensory median-ulnar nerve conduction latency at post-treatment compared to the sham group (p = 0.090), after controlling for baseline sensory median-ulnar latency. The fact that the active wrist-hand fitment group had 0.62 ms lower sensory median-ulnar conduction latency than the sham fitment group at 8 weeks (after controlling for baseline) indicated a clinically important improvement in the active wrist-hand fitment participants, even though this difference at 8 weeks did not achieve statistical significance in this small group. No significant difference in post-treatment sensory median-radial nerve conduction latency between groups was found (Table 2).
| Nerve conduction distal latency differences (ms) | Post-treatment Mean | F (p-value) | |
|---|---|---|---|
| Magnetic group | Sham group | ||
| Motor median-ulnar *Covariate baseline for both groups (1.958) |
1.594 | 2.058 | 4.435 (0.046) |
| Sensory median-ulnar *Covariate baseline for both groups (1.729) |
1.272 | 1.890 | 3.202 (0.090) |
| Sensory median-radial *Covariate baseline for both groups (1.305) |
1.067 | 1.033 | 0.012 (0.914) |
Table 2: Differences in 8-week nerve conduction distal latency between groups after controlling for baseline.
Symptom severity and functional status
After controlling for baseline values, no statistically significant differences between the groups were found in the severity of symptoms (total severity of symptoms and the separate symptoms of pain, numbness, weakness, or tingling) or functional limitations at 8 weeks (Table 3). Because there were no statistically significant differences by group, dependent t-tests were calculated to determine if the entire sample (pooled data from both active and sham groups) improved from baseline to post-treatment. When considering the entire sample with pooled data, a significant decrease in total symptom severity between baseline and post-treatment was present (p < 0.001; Table 4). These grouped participants rated pain (p = 0.002), numbness (p = 0.002), weakness (p = 0.013), and tingling (p < 0.001) significantly lower at post-treatment compared to baseline. Functional limitation also significantly decreased (p = 0.017). These results indicate selfreported improvement in the subjective measures from baseline to post-treatment regardless of group assignment, indicating that wearing the fitment itself had a positive effect.
| Subjective ratings | Baseline value | Post-treatment Mean | F (p-value) | |
|---|---|---|---|---|
| Magnetic group | Sham group | |||
| Symptom severity (SSS) (5-point scale – 1-5) |
2.575 | 2.076 | 2.134 | 0.069 (0.796) |
| Pain (11-point scale – 0-10) |
4.600 | 3.106 | 2.774 | 0.251 (0.621) |
| Numbness (11-point scale – 0-10) |
5.880 | 2.967 | 2.951 | 0.001 (0.979) |
| Weakness (11-point scale – 0-10) |
4.680 | 2.737 | 2.517 | 0.152 (0.700) |
| Tingling (11-point scale – 0-10) |
6.440 | 3.136 | 3.099 | 0.004 (0.948) |
| Functional limitations (5-point scale – 1-5) |
2.102 | 1.798 | 1.744 | 0.056 (0.815) |
Table 3: Differences in 8-week symptom severity and functional status by group after controlling for baseline.
| Subjective ratings | Baseline | Post-treatment | t-test (p-value) |
|---|---|---|---|
| Symptom severity (SSS) | 2.575 | 2.101 | 4.060 |
| (5-point scale – 1-5) | (<0.001) | ||
| Pain | 4.360 | 2.960 | 3.575 |
| (11-point scale – 0-10) | (0.002) | ||
| Numbness | 4.160 | 2.960 | 3.565 |
| (11-point scale – 0-10) | (0.002) | ||
| Weakness | 3.560 | 2.640 | 2.697 |
| (11-point scale – 0-10) | (0.013) | ||
| Tingling | 4.400 | 3.120 | 4.080 |
| (11-point scale – 0-10) | (<0.001) | ||
| Functional limitations | 2.102 | 1.775 | 2.577 |
| (5-point scale – 1-5) | (0.017) |
Table 4: Differences in 8-week symptom severity and functional status for the entire sample.
Because this was a pilot study, we examined results for statistical significance (p < 0.05) and trends toward significance without adjustment for multiple tests. The active wrist-hand fitment group showed an improvement in median motor nerve conduction (manifested by a decrease in the median-ulnar latency; p = 0.046).
The active fitment group also exhibited a trend toward improvement in median-ulnar sensory nerve latency compared to the sham group (Table 2). Although symptom and functional measures showed no group differences (Table 3), when pooling data from the active and sham groups to consider the entire sample, these measures improved over time (Table 4). Given that the pooled data (from both the active and sham groups) showed significant differences between baseline and post-treatment in symptoms (overall symptom severity as well as specific symptoms of pain, numbness, weakness, and tingling) and function, it may be that wearing the fitment itself was enough to make an improvement in participants’ perceptions of symptom severity and function over the course of the study.
The current findings of improvement in motor distal latency, with only a trend in sensory latency, are interesting considering the results of other studies. A study by Colbert et al. [10] reported no significant differences between groups in SSS, FSS, or median nerve conduction in a placebo-controlled, 6-week study using a three-group design comparing two dosages of SMFs (15 mT and 45 mT) and a sham group in 60 participants with electrophysiologically confirmed CTS. Each group, including the sham fitment group, showed an improvement in symptoms at 6 weeks, similar to the findings of the current study. However, outcome measures were assessed only at three time points (baseline, 6 weeks [following the intervention], and 18 weeks [after a 12-week follow-up period]). Moreover, Colbert and colleagues used magnetic disks applied to the participants’ wrists with adhesive tape in a single location rather than the fitments used in this current study that deliver the magnetic field over a larger area.
In a 4-week, placebo-controlled crossover study of 8 symptomatic hands on 6 persons, a static magnetic neoprene wrist wrap with a magnetic flux density of 35 mT (field penetration of 4 cm) resulted only in improvements in sensory latency in the active wrist wrap group, with no improvement seen in motor latency [12]. However, because no magnetic flux density measurements were presented, the mT level experienced at the carpal tunnel area of these participants is not known. Often, the manufacturer’s specified magnetic strength level for a product is unreliable across the product and does not reflect accurately the level measured by researchers on the product itself using a magnetometer. For this reason, we have included precise measurements of magnetic flux density at two distances from the surface of the fitments used in our study and have included the flux density maps at two distances above the fitment for an active magnetic wrist-hand fitment (Figures 2 and Figure 3).
It is important to note that participants with CTS in the present study who wore sham fitments also reported improvement in CTS symptoms. Various interpretations of these findings could include regression to the mean or a placebo effect. Strong placebo effects have been noted when using injections, surgery, and novel medical devices [37]. It also is possible that the sham fitment may have protected the wrist area from excessive movement and/or may have increased blood flow to the hand and wrist as a result of heat trapped by the neoprene fabric. Despite the effects observed in the sham fitment group, only those participants wearing the active magnetic fitments showed statistically significant improvement in median motor nerve conduction and a trend toward improvement in median sensory nerve conduction (Table 2).
Another consideration for interpreting SMF study results is revealed in the Weintraub and Cole [12] study. These investigators evaluated both hands on 2 participants and treated each hand as independent samples, an approach that we believe is problematic/flawed given that the neurological pairing of hands results in high correlations of responses in left and right hands. Therefore, we used only one hand (the hand the participant identified as more symptomatic) on each of 29 participants, although both hands may have been affected by CTS symptoms. Finally, the static magnetic wrist fitments used in the Weintraub and Cole study [12] and our current study had different magnetic field strengths, as well as differing spatial configurations of the field, which may have led to the discordant results. Yet, improvements in nerve conduction were found in participants in both studies, indicating a potential usefulness of this noninvasive modality, or a possible placebo effect.
One potential explanation of the differences in the findings of the Weintraub and Cole [12] study and the current study is that the lower strength magnetic fields may have preferentially improved motor nerve conduction, while the higher strength multi-polar magnetic fields may have fostered improvement in sensory nerve conduction. A study by Mansouri et al. [38] may lend support to this explanation given that these investigators reported that nerve conduction in the ulnar nerves of 12 healthy volunteers under normal versus high flux density (0.2 T) conditions showed significant changes in sensory latency and amplitude while exposed to the stronger field, although changes in motor nerve conduction were not significantly different.
As with any study, the current trial had several limitations. The severity of median nerve compression and minor recovery could not be captured precisely because of the absence of some of the severely involved median sensory nerve responses. During recovery, a sufficient number of fibers must conduct at the same speed for a deflection in the baseline to be observed. It is therefore possible that changes in the median sensory nerves also could have been more significant than what we found. An interesting observation, as described previously by De Smet [39], is the low correlation of the degree of discomfort and outcome satisfaction with objective findings in individuals with CTS. Involvement of the median motor fibers in all subjects may relate to the fact that the motor fibers are located superficially in the middle of the wrist. This superficial location in the wrist may be an explanation for the statistically significant improvement seen in motor nerve conduction latency in the active magnetic fitment group given that these more superficial structures would have been exposed to a slightly stronger field from the fitments than the deeper structures. The reason motor involvement has not been recognized in CTS in the past is likely a result of the use of less sensitive tests. As noted earlier, median-ulnar or median-radial nerve comparisons using the same recording locations are considerably better to identify a focal median neuropathy than simple median nerve latency studies or comparison of latencies from different locations. The authors found the combination as described in this study to be reliable parameters for the diagnosis and assessment of treatment for CTS.
One must view the present results with caution, as a multicenter follow-up study on the natural history of untreated CTS found that some hands improve spontaneously in the absence of therapy, while CTS symptoms, in general, tend to decrease with time. Padua et al. [40] found that CTS hands with initial low severity on both patient-oriented and neurophysiologic measurements tend to worsen, whereas CTS hands with initial high severity tend to improve over the course of 10 to 15 months. Our study team found that participants often will increase activity level if they experience relief of their CTS symptoms, leading to an exacerbation of symptoms. For this reason, it is important for investigators to capture information about participant activity levels to help in the interpretation of study findings.
Moreover, the diversity and pathophysiology of symptoms of CTS have been difficult to understand fully, given that statistical correlations between symptoms and nerve conduction studies are variable and inconsistent. You et al. [41] prospectively evaluated patients with electrophysiologically diagnosed CTS to correlate and identify relationships between symptoms and nerve conduction studies. Correlations (p < 0.001) for symptoms of numbness, tingling, and nocturnal symptoms were statistically stronger than for symptoms of pain, weakness, and clumsiness (p < 0.01). Findings from the You et al. study [41] suggest that these persistent symptoms (pain, weakness, clumsiness) may not be related necessarily to compression and dysfunction of the nerve. For example, inflammation in the synovium of the flexor tendons has been frequently implicated as a causative factor in CTS and can increase pressure in the carpal tunnel and contribute to median nerve compression [42,43]. Other studies also have shown that the most common synovial histological changes in CTS are related more to fibrosis and edema than to inflammation [44,45].
To validate the effectiveness of complementary therapies for CTS, especially therapeutic application of magnetic wrist-hand fitments, special attention has to be given to the methods of investigative studies. Although modern computerized electromyography greatly decreases measurement error, the use of consistent laboratory standards with meticulous attention to measurement and temperature control remains crucial [46]. Limiting assessments to questionnaires and clinical interviews only could lead to misdiagnosis and, therefore, over-treatment of the classic symptoms [47]. However, it should be noted that nerve conduction studies access only large myelinated fibers and not smaller ones that mediate pain [48]. Clinical signs, such as provocative maneuvers, also fail to improve the accuracy of diagnosing CTS [49].
The results of this pilot study reveal the feasibility and safety of testing SMFs for management of symptoms of CTS. Although the active magnetic wrist-hand fitment group showed moderate improvement in median motor nerve conduction and a trend toward improvement in median sensory nerve conduction compared to the sham group, both symptom and functional measures showed no group differences, although improvement was reported for the entire sample over the course of the study. The current findings of improvement in median ulnar motor distal latency, with only a trend toward improvement in median-ulnar sensory latency, still leave healthcare professionals without sufficient information to inform patients that SMFs are either effective or ineffective in the management of symptoms related to CTS. More studies are needed to determine the optimum SMF dose and to assess issues related to the use of sham controls in trials involving SMF testing.
The authors declare that they have no conflicts of interest.
AGT conceptualized the idea, secured funding, oversaw the research study, and co-wrote the manuscript. PFR was the study coordinator and co-wrote the manuscript. MDiB performed the electrodiagnostic testing, participated in interpretation of the electrodiagnostic testing data, and co-wrote the manuscript. CB conducted the data analyses and participated in interpretation of the data. JGA conducted data analyses, participated in interpretation of the data, and edited the manuscript. GTG validated the magnetic strength of the wrist-hand fitments and edited the manuscript. All authors read and approved the final manuscript.
This publication was made possible by grant number 5-K30-AT-000060 from the National Center for Complementary and Alternative Medicine (NCCAM) at the National Institutes of Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NCCAM.