Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2014) Volume 3, Issue 5
Study background: Obesity is constantly increasing health problem worldwide and so are its detrimental consequences, including obstructive sleep apnea (OSA). Mandibular advancement devices (MADs) are proven to be efficient in treating mild to moderate OSA and snoring. We followed for two years 103 patients treated with a titrable MAD in a Community Dental Care setting. Methods: A follow-up questionnaire was mailed in 2012 to 124 patients who had participated in a survey 2010 and given their consent for further study. Results: Of all the 103 respondents 85% (n=88) still used MAD. Subjective tiredness (p<0.05) and the presence of any snoring (p<0.01) were reported more often in the long-term study than in the short-term study. In contrast, difficulty in initiating sleep with the device in situ was seen less often (p<0.05). According to the logistic regression, reduced loud snoring was significantly associated with the compliance of frequent wear of MAD (p<0.05). The majority (82%) of the patients also reported a positive impact of MAD in social (family) life due to reduced loud snoring. Conclusion: Titrable MAD is a noteworthy treatment modality for mild to moderate OSA and especially snoring. Compliance in using MADs and reported subjective health seem to remain at good level. General dentists could probably perform a great part of the care. However, possible worsening of OSA and side effects of MADs should be borne in mind.
Keywords: Obstructive sleep apnea; Snoring; Oral appliance; Compliance; Community dental care; Long-term study
The use of mandible advancement devices (MAD) in the treatment of obstructive sleep apnea (OSA) and snoring has increasingly become an alternative treatment modality for continuous positive airway pressure (CPAP) in patients with mild to moderate OSA. In these patients, clinical studies have shown equal efficacy between both modalities on ambulatory blood pressure, daytime sleepiness, and quality of life, among other things [1]. These results may also be explained by good clinical use of MAD, since particularly in mild OSA, the compliance with CPAP is frequently far from optimal [2-5].
Bearing in mind the increasing incidence of OSA worldwide [6,7] there is a need to improve clinical guidelines to be able to provide the best possible treatment option for each patient. In addition, the treatment modalities need to manage this condition cost-effectively. OSA is a chronic, progressive disease and particularly, the more severe stages of OSA have been linked to an increased risk of cardiovascular morbidity and mortality [8,9].
Obesity is the most important risk factor for OSA and based on current knowledge about the evolution of OSA, it is particularly the weight gain that represents a high risk for further progression towards more severe disease [10]. Recent studies have well-demonstrated that lifestyle intervention, including an early weight reduction program, represents a feasible and effective treatment for OSA and the achieved beneficial changes are sustained even four years after the active intervention, thus preventing the progression of the disease or even curing it in obese patients with OSA [11,12].
On the other hand, it has been shown that deviations in craniofacial morphology are much more common in normal weight than in overweight adult patients with OSA [13]. Together, these findings imply that there may be three different phenotypes of sleep-disordered breathing; one related to excess fat tissue, the other to craniofacial abnormalities and the third a combination of these two phenotypes. Hence, especially in normal-weight patients with mild or moderate OSA and in the case of disturbing snoring, MAD could represent a first-line treatment strategy.
Not only the efficacy but also the possible side effects of a treatment play important roles when choosing one treatment over the other. MAD reportedly causes symptoms of temporomandibular disorders (TMD), tooth pain, and development of posterior open bite [14-16]. This may seriously affect the compliance, thus resulting in discontinuing of treatment. However, the adverse symptoms are often transient. Also, loss or frequent breakage of the device, along with the cost of repairing or replacing it, may lead to cessation of treatment [17].
Our recent pilot study, based on self-report on short-term MAD treatment among patients in Community Dental Care, showed good compliance and a fair treatment effect on sleep quality [18]. As many as four out of every five patients had worn their device at least three nights per week, while sleep was reported being significantly less disrupted and more restorative, leading to markedly less frequent daytime sleepiness.
To our knowledge, thus far no other study exists on the effects of MAD on OSA and snoring that has been performed among patients treated in Community Dental Care. The aim of this study was to evaluate self-reported longer-term effects and compliance of MAD treatment in this specific setting, perhaps presenting better the real-life setting of the treatment.
A pilot questionnaire study was performed in 2010 [18], comprising 142 patients who had received MAD treatment for OSA or snoring in the Unit for Specialized Oral Care in the Metropolitan Area in Finland. The unit is a part of the public dental care system with subsidy. All patients had been treated with a titrable Herbst-type MAD. To the participants of that study, a follow-up questionnaire was mailed in 2012. Altogether, 124 respondents who had completed the pilot questionnaire and gave written consent to the additional study were mailed the follow-up questionnaire.
From the questionnaire, data were categorized for the present study as follows:
Descriptive data: gender, age, weight, length, tobacco use, alcohol consumption (equivalent doses of beer, wine, or spirits), aspects of general health, and orofacial pain experience during the past month [18-20]. The body mass index (BMI) was calculated from the weight and length data. Data on treatment decision-making, prior dental treatment, adaptation to the treatment, device maintenance need, and various subjective side effects were also included.
Compliance in using the oral appliance: self-assessed frequency of wearing the MAD (never or less than once a month, less than weekly, 1-2 nights per week, 3-5 nights per week, every night or almost every night).
Insomnia symptoms [7,21]: difficulties initiating sleep (DIS), disrupted sleep (DS), and early morning awakenings (EMA) (symptoms present at least 3 nights per week).
Perceived consequences of sleep: non-restorative sleep (NRS) (sustained>1 month), and tiredness (at least 3 days per week).
Snoring: as perceived or reported by a bed partner (every night or almost every night).
Type of snoring: as reported and confirmed by bed partner (smooth and quiet, smooth and rather loud, smooth and loud, intermittent and very loud)
Statistical analysis
For the demographic data, the Chi square test was used to study the associations between the categorical variables. Student’s t-test was used to compare the group means when the data were normally distributed, and when not, the Mann-Whitney U-test was applied. McNemar change test was used to compare the insomnia symptoms and perceived consequences of sleep between short-term and long-term studies. Logistic regression was used to study the probability of the compliance of frequent wearing of the MAD (‘every night’ or ‘almost every night’=1, else=0). Independent variables entered into the model, adjusted by BMI, age, and gender, were; NRS (yes=1, no=0), DS (yes=1, no=0), intermittent very loud snoring (yes=1, no=0). The method enter was used, i.e., all independent variables were entered in the model as a single step.
The response rate of eligible subjects of the second questionnaire was 83% (n=103). The flow chart of the study is shown in Figure 1. Of all the respondents, 85% still used the MAD (n=88), 67% of them were male (n=59). Mean lifetime of devices i.e. the mean time period between oral appliance put to use and the return date of long-term survey was 35 months (2.9 years) (SD=11.0), the longest period being 67 months (5.6 years) and the shortest 23 months (1.9 years). As compared with the short-term study [18], there were no significant differences in the demographic data, viz., age, gender, BMI, alcohol consumption, and smoking status.
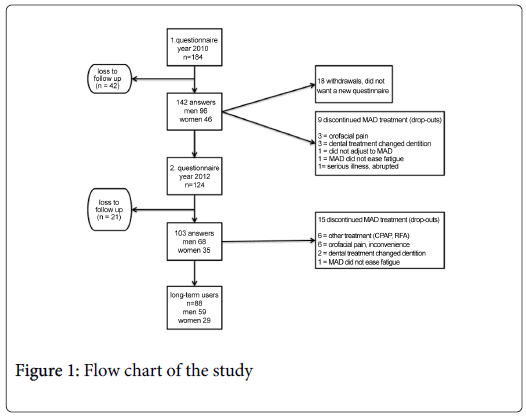
Figure 1: Flow chart of the study
OSA was diagnosed in 77.3%, the rest 22.7% was diagnosed as snorers. In both genders, health was more often reported as ‘very good’ or ‘good’ than in the pilot study (p<0.05) (45% of women and 54% of men). None of the respondents in the present study reported their health as ‘very poor’. Compared to the pilot study (figures in parentheses), diagnosed illnesses were: hypertension blood pressure 36 % (35%), allergic rhinitis 28% (25%) and cardiac arrhythmia 17% (18%) (NS). Cardiac arrhythmia was more common in women, viz. 28%, than in men (12%.) Other diagnosed illnesses were not related to gender.
The subjects had significantly less difficulty in initiating sleep with MAD in situ than what they reported earlier (p<0.05). Altogether 82% of patients claimed that MAD has a positive impact on personal life due to reduced loud snoring. Whereas subjective tiredness (p<0.05) and snoring (p<0.01) were reported more often than in the short-term study. Table 1 shows perceived insomnia symptoms and snoring and related daytime consequences between baseline and the present study.
| n=88 | % | Baseline | Long-term | p value |
|---|---|---|---|---|
| DIS | 10.2 | 2.3 | 0.039 | |
| DS | 39.8 | 52.3 | 0.072 | |
| EMA | 11.4 | 13.6 | 0.774 | |
| NRS | 4.5 | 6.8 | 0.727 | |
| Tiredness | 15.9 | 27.3 | 0.021 | |
| Snoring | 14.8 | 36.4 | 0.002 |
Table 1: Overall occurrence of perceived insomnia symptoms and their awake consequences at baseline and two-year long-term. McNemar change test (DIS: difficulties initiating sleep, DS: disrupted sleep, EMA:early morning awakening, NRS: non-restorative sleep).
The treatment of OSA was initiated by a physician for the majority (81%) and the rest by a dentist. None of the subjects had received treatment by their own request. Prior dental check-up to the treatment was performed in 36%. Most often reported problems with wearing the MAD were sore teeth (39%), soreness in masticatory muscles (37%), and experience that the teeth do not fit (27%) upon awakening. Orofacial pain experience within the past month was reported more often (31% vs. 22%, p<0.01) in the present study than in the short-term study.
Within a short period after initiating the treatment altogether 75% of patients had well adapted to the MAD. Logistic regression, adjusted by BMI, age and gender, revealed a significant association between good compliance (frequent use of MAD) and less loud snoring (p<0.05) (Table 2).
| n=88 | Odds Ratio | 91% confidence interval | p-value |
|---|---|---|---|
| NRS | 0.5 | 0.1-5.1 | 0.51 |
| DS | 0.9 | 0.2-4.0 | 0.26 |
| Loud snoring | 0.6 | 0.3-0.9 | 0.04 |
Table 2: The compliance of frequent wear of the MAD Logistic regression (NRS: non-restorative sleep, DS: disrupted sleep Model adjusted by BMI, age, and gender).
The present study is the first long-term study on the treatment of OSA with MADs in Community Dental Care. Main reason for carrying out this study was to clarify possibilities in treating the increasing amount of patients with sleep-disordered breathing [22] in common dental practice. Long-term studies in such real-life setting are lacking according to our knowledge.
The main finding of the present study was that treatment of OSA with MAD is well tolerated and its compliance remains good. This is also supported in studies carried out in specialist settings [16,17,23-25]. MAD was found to reduce loud snoring. Also, the occurrence of early morning awakenings (EMA) and non-restorative sleep (NRS) remained at low level among respondents in the follow-up period. In addition, morning sleepiness remained minor in follow-up.
Some of the subjective benefits that emerged initially in our short-term study were less prevalent. Daytime tiredness was more often reported. Similarly, disrupted sleep (DS) and the frequency of snoring were reportedly increased. This set back of longer-term subjective benefits has also been shown in a study by Ghazal et al. [26]. Although half of the respondents stated their health as ‘good’ or ‘very good’ (in our short-term study 41%), and none continuously as ‘poor’ or ‘very poor’, our results indicate that long-term follow-up and, when needed, adjustment of the device may be necessary to obtain the best possible result.
In the present study orofacial pain was reported more frequently than in our short-term study. This is contradictory to what has been reported earlier regarding TMD, i.e., TMD having a transient nature in association with MAD [14,16]. However, we only used a single question to evaluate this (derived from the Finnish translation of the RDC/TMD): “Have you had pain in the face, jaw, temple, in front ear or in the ear in the past month?”) [19,20]. Bearing in mind the quasi-static nature of TMD, our findings have to be interpreted cautiously. Also, posterior open bite (POB) as a complication has been reported in clinical studies earlier [15,16], which due to the study design cannot be evaluated here.
Limitation of the present study is that it is based on a questionnaire without objective evidence. Yet, only few longer-term studies exist in this field [27,28]. Also, the sample size (n=103) in our study may be considered fair [23]. Nevertheless, larger-scale studies that include clinical evidence are certainly needed. However, few follow-up studies have concentrated on subjective results of sleep quality. In fact, most existing studies have focused on the influence of MAD on aspects of the masticatory system, namely, TMD-problems [14-16].
When evaluating an impact of treatment long-term evidence is essential. Unfortunately, most published studies have been concentrating only on short-time use of MADs. As seen in the present study, the long-term effects of MAD on sleep quality weakened to some extent, which was a disappointment, as the results in our previous study [18] as well as in other short-term studies [29,30] have been promising. On the other hand, Jauhar et al. reported only modest improvement in sleep quality in their ten-year follow-up study [25]. Nevertheless, McGown et al. and Wiman Eriksson et al. found improved daytime tiredness compared to baseline in a long-term design [27,28]. This all may be summoned that more intensive control of effect of the treatment, i.e. regular checkups of the symptoms and if needed, the devices, may be advisable for better results.
Since the treatment of OSA is demanding, there are no simple solutions and the treatment must always be planned individually. It is important to keep on improving the current treatment modalities and, in addition, trying to find new guidelines for better treatment of OSA patients. There seems to be several phenotypes of OSA patients i.e. related to obesity or cranio-facial anatomy. Furthermore, it may be a combination of different factors and treatment may modulate the underlying mechanisms. Tuomilehto et al showed that weight loss of obese OSA patients could reduce the amount of respiratory events in both supine and non-supine positions [11]. However, the reduction in the number of events was higher in the non-supine position. Especially for positional OSA, where most of the respiratory events occur in supine position, oral appliances are shown to be particularly effective and may offer an important alternative to CPAP [31,32]. However, it seems that regular follow-up and support for MAD users may be essential.
This study was supported by grants from the City of Helsinki Health Centre and the Finnish Association of Women Dentists.