Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Protocol Article - (2014) Volume 4, Issue 1
Objective: This study will investigate the efficacy of implementing either an early or delayed exercise intervention on cardiovascular and cerebrovascular health for newly diagnosed stroke and high-risk Transient Ischaemic Attack (TIA) patients.
Methods: The study is a randomized, parallel group clinical trial. Patients will be recruited from a local hospital based on inclusion/exclusion criteria. Participants will attend a baseline assessment within 2 to 7 days of stroke or TIA diagnosis. The assessment will consist of a series of cardiovascular and cerebrovascular primary and secondary outcome measures which will be assessed during some or all of the following; at rest, during a postural challenge, during a cerebral autoregulation and CO2 reactivity test and/or during an incremental exercise test. Primary outcome measures include vascular risk factors (resting blood pressure, blood lipid profile etc), arterial stiffness of the carotid artery and blood velocity of the carotid artery and middle cerebral artery. Secondary outcome measures include cerebral autoregulation, physical fitness, and central and peripheral blood pressure. Following the baseline assessment, participants will be randomized to either a 12-week exercise programme which will commence within 7 days (early) or 28 days (delayed) of stroke/TIA diagnosis, or to a usual care control group. The exercise programme will consist of twice weekly, 60 minute, prescribed aerobic exercise sessions, and one 30 minute home-based aerobic exercise session. An identical assessment will be implemented post-intervention. Given the practical implications of the study, the clinical significance of early or delayed exercise engagement will be assessed for each outcome variable.
Conclusion: This study will advance our knowledge concerning the timing, importance and viability of exercise as a secondary prevention strategy for improving health outcomes for stroke and TIA patients. The study will provide much needed objective data for stroke and high-risk TIA patients concerning the physiological effect of regular exercise participation.
Keywords: Exercise; TIA; Randomized controlled trial; Secondary prevention; Peripheral vascular diseases; Arterial stiffness; Blood velocity
Stroke is a leading cause of death in the Western World, and is a prominent cause of chronic disability, causing significant physical and cognitive impairments [1]. Stroke is broadly classified into two main types: ischaemic and haemorrhagic, with the former accounting for more than 85% of cases [1]. Approximately 15% of all strokes are heralded by a Transient Ischaemic Attack (TIA) [2]. TIAs are ischaemic brain attacks with focal cerebral or retinal symptoms that last <24 h, usually <1 h [3]. Meta-analyses have demonstrated the short-term risk of stroke after TIA to be between 3-10% at 2 days, and 9-17% at 90 days [1].
Many people who present with a TIA have predisposing modifiable vascular risk factors such as hypertension, tobacco use, diabetes mellitus, hyperlipidaemia, obesity and physical inactivity [4]. The primary preventative strategy used to reduce the risk of a recurrent stroke or TIA includes the prescription of anti-platelet- or anti-coagulation agents, as well as blood pressure- and lipid lowering treatments [5]. However, it has been suggested that 80% of recurrent vascular events could be prevented through a comprehensive multifactorial lifestyle strategy which may include the implementation of physical activity, dietary advice and lifestyle modification [6]. Exercisebased Cardiac Rehabilitation (CR), which utilises a multi-factorial strategy, has been shown to improve each of the aforementioned risk factors (i.e., improved blood pressure and blood lipid profile), and reduce morbidity and mortality among Coronary Artery Disease (CAD) patients [7].
To date, a limited number of a non-pharmacological interventions for secondary prevention of stroke following TIA have been investigated [8], with only two Randomized Controlled Trials (RCT) examining the efficacy of regular physical activity participation [7,9]. The beneficial effect of regular exercise participation, implemented within the acute or sub-acute phase, has been shown with improvements in vascular risk factors (i.e., blood pressure, total cholesterol) and aerobic fitness in TIA [6,9] and ischaemic stroke patients [7]. However, the RCTs implemented by Lennon and Blake [7] and Faulkner et al. [9] did not explore a number of physiological markers that may serve to enhance our understanding of the effects of exercise on cardio- and cerebrovascular health within this population group (i.e., arterial stiffness, cerebral blood flow regulation). As a consequence of the limited number of investigations, particularly in the acute phase [5], no recommendations can be drawn with respect to guiding best practice for this population group [8].
Early mobilization and better blood pressure control have been suggested to be the greatest contributors to improved health outcomes with newly diagnosed stroke patients [10]. Early mobilization has been promoted within Published stroke guidelines [10], although the practice remains controversial due to inconclusive evidence [11]. A recent meta-analysis of randomized and non-Randomized Controlled Trials (RCT) demonstrated that stroke survivors may benefit from cardiovascular exercise during the sub-acute stage as it may contribute to improvements in peak oxygen uptake and walking distance [12]. In theory, improvements in these measures of aerobic capacity may be aligned with an improved vascular profile, and reduced risk of recurrent cerebrovascular events. However, the authors defined the commencement of an exercise programme within 6 months of stroke diagnosis to be ‘early’ [12]. There is little clear consensus about what constitutes ‘early’ and thus what the optimal time to start a rehabilitation program is. In the acute and sub-acute phase of stroke care, getting the balance right between diagnosis, medical interventions and exercise rehabilitation can be challenging. Improving our understanding of the impact of the rehabilitation intervention on brain recovery, cardiovascular health and functional restoration should be a priority for stroke and TIA research, particularly as it has major implications for public health.
This study will investigate the efficacy of implementing either an early or delayed exercise intervention on cardiovascular and cerebrovascular health for newly diagnosed stroke or high-risk TIA patients. It is the intention that the present study will provide significant pilot data for a fully-funded randomized controlled trial, and may provide direction for future exercise prescription policy in this population cohort.
Research design
This is a dual-centre, randomized, parallel group clinical trial. This study is designed pragmatically to ensure that it reflects a potential real life application of an exercise intervention for stroke and high risk TIA patients.
Patient population
All stroke referrals are reviewed by specialist neurologists at a hospital and appropriate diagnostic tests are undertaken (stroke classification, side of body affected) including the National Institutes of Health Stroke Scale (NIHSS) and modified Barthel Index. The NIHSS is used to objectively quantify the impairment caused by stroke or TIA. It is composed of 11 items, each of which scores a specific ability (i.e., motor arm and motor leg function) between 0 (normal function) and 4 (significant impairment) [13]. The modified Barthel Index is used to establish the degree of independence during hospital admission [14]. The Neurology department uses scores of 13 out of 20 as an indicator that the patient may be suitable for discharge home [14], pending on the home situation, the available help, previous function and diagnostic criteria.
Inclusion criteria
• Those diagnosed with a stroke or high risk TIA (with ABCD2 score ≥ 4), after review by a specialist stroke physician.
• Those living within Wellington City and the Greater Wellington region.
Exclusion criteria
• Oxygen dependence, uncontrolled angina, unstable cardiac conditions (i.e., atrial fibrillation), uncontrolled diabetes mellitus, major medical conditions, claudication, febrile illness, significant cognitive impairment, immobile, age>85 years
Randomization
Participants will be randomized on completion of a baseline assessment (Figure 1). Participants will be assigned, using simple randomization, to either:
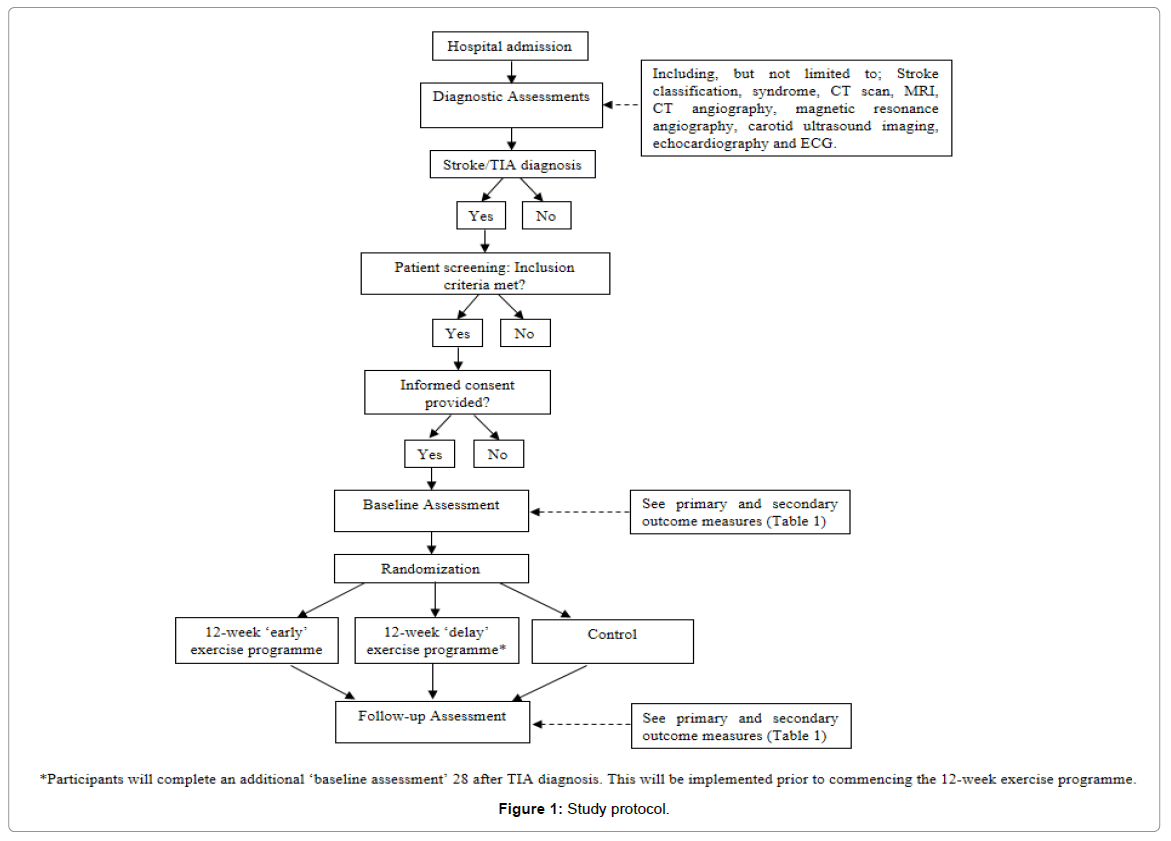
Figure 1: Study protocol.
i) a 12-week exercise programme which will commence within 7 days of stroke/TIA diagnosis (‘early’)
ii) a 12-week exercise programme which will commence 28 days after stroke/TIA diagnosis (‘delay’)
iii) Usual care control group (i.e. no additional supportive strategies will be implemented).
Details of the allocated group will be given on a piece of paper contained within sequentially numbered, opaque sealed envelopes. The randomization procedures will be prepared by an investigator with no clinical involvement in the trial. Although participants and the health and exercise practitioners will be aware of the allocated treatment condition, outcome assessors and data analysts will be kept blinded to the allocation.
For those participants randomized to the ‘delay’ exercise group, an additional assessment session will be conducted prior to the commencement of their exercise programme. This assessment will include all measures conducted in the initial baseline assessment. The purpose of this session is to identify any changes in cardiovascular and cerebrovascular health since the initial stroke/TIA diagnosis.
Baseline laboratory assessment and outcome measures
A baseline laboratory assessment will take place following hospital discharge and within 2 to 4 days of stroke/TIA diagnosis. Participants will be fasted (>10 hours) prior to the laboratory assessment. Primary and secondary outcome measures will be monitored during the assessment (Table 1). These measures include stiffness and blood velocity of the carotid artery, blood velocity of the middle cerebral artery, central and peripheral blood pressures and an Electrocardiogram (ECG). These cardiovascular and cerebrovascular outcome measures will be completed during all or some of the following; 20 minutes supine rest, during a postural challenge, a cerebral autoregulation and CO2 reactivity test and/or an exercise test (Figure 2). The postural challenge will use a modified tilt table [15], in which the researchers will manually lift a hinged table 60o over 1.5s. The exercise test will be completed on a cycle ergometer. This test will be continuous and incremental, commencing at a low-intensity (30 W) and getting progressively harder (30 W every 2 minutes). The exercise test will be terminated when the subject reports volitional exhaustion physiological responses are observed from the ECG (e.g. 2 mm ST depression).
| Dependent variable | Procedure / measures | Study outcome | Type of measurement |
|---|---|---|---|
| Health History Questionnaire [18] | •Questionnaire to identify family history, personal history and signs and symptoms of cardiovascular disease, and to provide a lifestyle evaluation | Secondary | Rest |
| Vascular risk factors [18] | •Fasted blood lipid profile (total cholesterol, high-intensity lipoproteins etc.) and blood glucose (capillary sample). •Resting supine systolic and diastolic blood pressure. •Body weight, body mass index, waist and hip circumference. |
Primary | Rest |
| Arterial stiffness of carotid artery | •Following 20 minutes post-supine rest, local arterial stiffness of the carotid arteries will be imaged 1-2 cm proximal to the bifurcation using B-mode ultrasound. | Primary | Rest |
| Blood velocity of carotid artery | •Doppler ultrasonography will be used to calculate bilaterally volumetric blood flow in the carotid artery. Blood flow will be recorded using a Doppler spectral trace for 3 minutes during supine rest, during the postural challenge, and for 5-minutes post-modified tilt test. | Primary | Rest, postural tilt |
| Blood velocity of Middle Cerebral Artery (MCA) | •Transcranial Doppler (TCD) ultrasonography will continuously measure cerebral blood flow. | Primary | Rest, postural tilt, exercise |
| Central & peripheral blood pressures | •Pulse wave analysis will investigate central blood pressures, augmentation index and arterial stiffness. | Secondary | Rest |
| Beat-to-beat blood pressure | •Finger photoplethysmography | Secondary | Rest, postural tilt |
| Cerebral autoregulation and CO2 reactivity test | •Cerebrovascular reactivity to changes in the partial pressure of arterial CO2 is a recognised indicator of brain vascular reserve [19]. Sitting in a recumbent (60o) position, participants will breathe a CO2 gas mixture (5% CO2, 21% O2, balanced N2) for 100 s followed by 100 s of voluntary hyperventilation until the partial pressure of end tidal CO2 decreases by 4mmHg or more relative to baseline. Changes in the MCA blood velocity relative to changes in end tidal PCO2 and blood pressure will be assessed. | Secondary | Rest |
| Physical fitness | •A peak and/or symptom limited exercise ECG on a cycle ergometer will be undertaken to determine whether it is clinically safe for participants to engage in the exercise programme. This test will be continuous and incremental. Participants’ ECG, heart rate, blood pressure and blood velocity of the MCA will be continuously recorded. | Secondary | Exercise |
Table 1: Study outcomes which will be measured at the baseline and follow-up assessments.
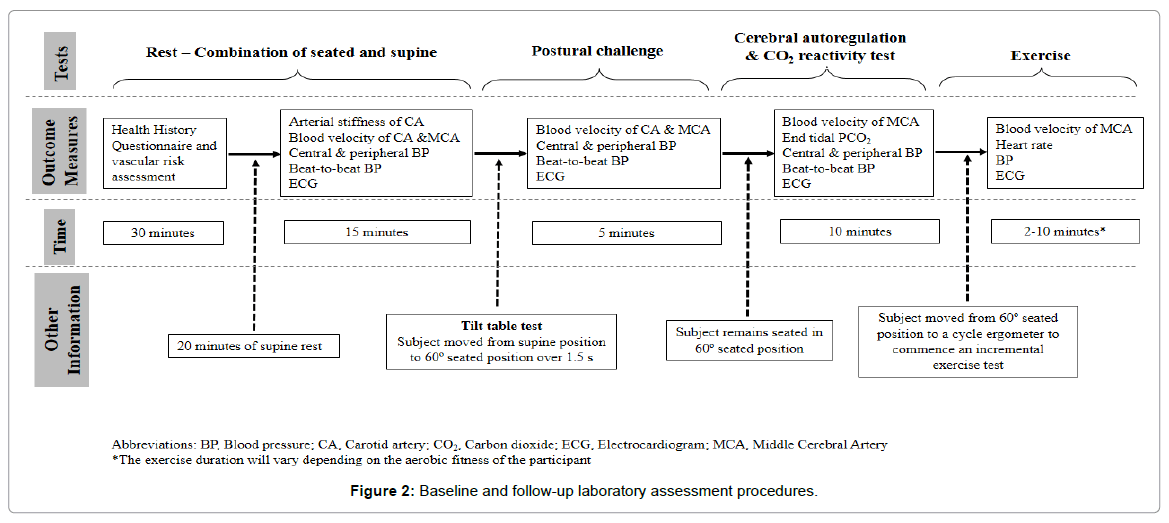
Figure 2: Baseline and follow-up laboratory assessment procedures.
Identical assessments will occur at the follow-up assessment (postintervention).
12 week exercise programme
Participants randomized to the exercise programme (‘early’ and ‘delay’ group) will take part in a twice weekly, group focused (3 to 5 patients) aerobic exercise session, for a period of 12 weeks. Exercise will be prescribed on a one-to-one basis by a health and exercise practitioner. Each session will be for 60 minutes, incorporating 30 to 45 minutes of aerobic exercise (walking, cycling etc). The remaining exercise session will consist of flexibility and balance exercises. Blood pressure, heart rate and RPE will be measured prior to, during and following each bout of aerobic exercise. Participants will exercise between 60 and 95% of age-predicted maximal heart rate during each aerobic exercise tasks. The exercise intensity will increase by ~5% each week, although the rate of progression will be dependent upon how the subject feels during each session. Exercise practitioners will ensure that participants do not exercise above 95% of their age-predicted maximal heart rate, or beyond intensities defined by their cardiac risk as identified from the baseline ECG assessment.
Participants will also be asked to complete an additional homebased exercise session, consisting of 30 minutes walking.
Ethical approval and informed consent
The study protocol has Received date: ethical approval from the New Zealand Health and Disability Ethics Committee. The study has also been registered with the Australian and New Zealand Clinical Trials Registry: ACTRN12613000869774. Written informed consent will be obtained from all study participants.
Data monitoring body
A Research Steering Committee will meet once every 3 months to discuss data and safety monitoring (i.e., adverse events) and to provide advice on implementation of the research outcomes and outputs. The steering committee will include members of the research team and external stakeholders from the University sector, Hospital and community.
Sample size
Sixty participants will be recruited and evenly allocated to each of the three groups to enable an appropriate sample size to be calculated for a larger trial.
Data analysis
The number of subjects which will be screened for inclusion, and the number of individuals who decide not to participate in the study will be tracked. Participant compliance and adherence to the assessment and exercise sessions will be monitored.
Baseline characteristics of the three study groups will be described by means and standard deviations, and percentages as appropriate for the level of measurement and distributions of the data. Baseline characteristics will be compared between groups using a series of one-way analysis of variance (ANOVA). Two-way repeated measures ANOVAs: Condition (early, delay, control) by Time (baseline, postintervention), will be used to compare all primary and secondary outcome measures. Where statistical differences are observed from the preceding analyses, post-hoc analyses for multiple comparisons will be conducted (Bonferroni adjusted t-tests; Tukeys HSD). An intentionto- treat analysis will be used on all consented subjects who are unable to attend the follow-up assessment. Effect sizes will be reported to describe the importance of the relevant findings in practical terms.
The high prevalence of a recurrent TIA or stroke underscores the need for appropriate secondary prevention strategies. Regular physical activity participation may be an important strategy which may yield favourable improvements in physiological outcome measures for these population groups. A recent meta epidemiological study has demonstrated that exercise should be more widely used in the secondary prevention of cardiovascular and cerebrovascular events, and rehabilitation after stroke [16]. In fact, the findings of this review suggest that exercise and many drug interventions are similar in terms of their mortality benefits, and as such, exercise should be considered a viable alternative to, or alongside, drug therapy [16]. However, the scientific rigor behind implementing exercise programmes soon after diagnosis remains controversial [17] due to inconclusive evidence [11]. Although recent research has shown the aerobic and vascular benefit of exercise for ischaemic stroke and TIA patients [7,9], a more comprehensive understanding of the physiological effect of exercise on cardio- and cerebrovascular health outcomes is needed, along with the time domain (early, delayed) for when it should be implemented. An improved understanding of when rehabilitation programmes should be implemented is required to ensure an optimal environment for brain recovery, cardiovascular health and functional restoration. With so few exercise based RCTs being implemented worldwide [16], this is a novel and highly important area of research which requires significant consideration [18,19].
This study may significantly contribute to our knowledge in stroke and TIA rehabilitation, prevent recurrent vascular events and may be a viable secondary prevention strategy which could reduce the mounting health care costs associated with stroke and TIA. The study will provide much needed objective data for stroke and high-risk TIA patients concerning the physiological effect of regular exercise participation. Importantly, this study will identify the effect of patients engaging in exercise immediately following stroke/TIA diagnosis (early) or following a delay. Given the practical implications of the present study, we will examine the clinical significance of early or delayed exercise engagement for each outcome variable.
The study team would like to thank the Massey University Research Fund and University of Otago for their financial support.