Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Short Communication - (2015) Volume 3, Issue 5
Background: Primary mediastinal B-cell lymphoma (PMBCL) is a distinct clinicopathologic entity from diffuse large B-cell lymphoma. The optimal first-line therapy for PMBCL is subject of ongoing debate with no accepted standard of care.
Patients and Methods: We searched retrospectively for adult patients with newly diagnosed PMBCL treated at our department between 2002 and 2014. Clinical, management and follow-up data were collected. Staging and response assessment of patients included PET and/or CT scan.
Results: Twenty-nine patients with PMBCL (17 female and 12 male) were included. The median age at diagnosis was 36 years (18-79 years). Eighteen (62.1%) and 20 (69%) patients had limited-stage and bulky disease, respectively. All patients were treated with rituximab-based combination chemotherapy; 21 patients underwent consolidation radiotherapy. Seven patients (24.1%) were transplanted (six in first remission and the remaining in second remission). At the end of frontline therapy, 28 patients had responded (27 complete response and 1 partial response) and one patient showed progressive disease. Febrile neutropenia was the most frequent acute adverse event and three patients developed late toxicity. The median follow-up was 51,5 months. The 5-year overall progression-free survival was 83.8%. Four patients died, half of which died within the first year after diagnosis.
Conclusion: Our study shows favorable prognosis of patients with PMBCL treated with rituximab-based chemotherapy and consolidation radiotherapy or autologous stem-cell transplant. While consolidation therapy continues to be commonly used, its role has become increasingly controversial.
Keywords: Aggressive lymphoma; Radiotherapy; Autologous stemcell transplant; Prognosis; Mediastinal tumors
Primary mediastinal B-cell lymphoma (PMBCL) was first recognized in 1980, but only recently has caught attention after being classified as a distinct subtype of diffuse large B-cell lymphoma (DLBCL) [1,2]. It is an aggressive lymphoma accounting for less than 3% of all non-Hodgkin lymphoma and 10% of all DLBCL. It occurs more often during the third and fourth decades of life and shows a female propensity (male-to-female ratio of 1:2) [3,4].
It arises in the thymus from a so-called thymic B-cell either from a germinal center or a non-germinal center [5]. Important differential diagnoses include Hodgkin lymphoma (HL), precursor T-cell lymphoblastic lymphoma, mediastinal germ-cell tumor and primary lung malignancies. It is being increasingly recognized that PMBCL is closely related and shares many imunohistochemical and molecular features with nodular sclerosis HL. Additionally, a small number of cases presenting with clinicopathologic features intermediate between PMBCL and HL have been reported - marginal gray zone lymphoma [1]. These lymphoma also present in the mediastinum but, compared to PMBCL, have a male predominance and an inferior outcome [6].
The optimal therapeutic approach to PMBCL is controversial and there is no accepted standard of care. Different types of protocols have been reported and different institutions using similar regimens have reported different complete response and survival rates [7-10].
The main purpose of this study was to investigate clinical features, treatment plan and overall survival of patients with PMBCL treated at our institution with rituximab-based combination regimen. Additionally, we have reviewed the literature and discussed alternative therapeutic strategies.
Clinical evaluation
For this retrospective study, all adult (≥18 years old) patients with PMBCL treated at our department were considered eligible. All patients had a biopsy proven histological diagnosis of PMBCL based on the current WHO/REAL classification. Patients with minimal mediastinal involvement as part of more extensive lymphoma elsewhere and those treated before January 2002 (rituximab was gradually introduced in our clinical practice during 2002) were excluded. A final cohort of 29 patients was identified. The Institutional Ethical Committee at the Portuguese Institute of Oncology – Porto reviewed and approved this study. The following information was collected from the cohorts’ medical records: demographic data, imunohistochemistry, details of clinical and radiological presentation, response to treatment and the outcome of lymphoma. Endpoints analyzed included response to frontline therapy, progression-free survival (PFS), overall survival (OS) and treatment related toxicity. Staging evaluation included: physical exam, clinical and hematological survey, chest X-ray, computerized tomography of the thorax, abdomen and pelvis or positron emission tomography and unilateral bone marrow biopsy. Central nervous system evaluation (e.g., lumbar puncture, magnetic resonance imaging of the head) was done only in patients with involvement of multiple extranodal sites, involvement of one nodal site associated with high lactate dehydrogenase (LDH) or neurologic symptoms. Bulky disease was defined as a mass of 10 cm or more in greatest dimension.
Treatment protocol
All patients were treated with rituximab-based combination chemotherapy. Patients with localized disease were intended to receive consolidation radiotherapy (RT, 3600 cGy). Prior to 2010, patients with advanced disease, International Prognostic Index (IPI) higher than 1 and less than 66 years of age were intended to receive autologous stemcell transplant (ASCT). Mobilized peripheral blood was the source of stem cells and BEAM (carmustine, etoposide, cytarabine and melphalan) was the preparative regimen for transplant. After 2010, patients with advanced disease were intended to receive consolidation RT. Clinicians assessed treatment response according to international criteria [11]. Adverse events were assessed and graded according to NCI-CTCAE version 4.0. Events grade 3-4 or requiring hospital admission were considered as significant. Salvage therapy was determined on individual basis.
Statistical analysis
Descriptive statistics were used in this study. Overall survival (OS) was calculated from the date of biopsy-proven diagnosis to the time of death or date of last follow-up visit. Progression-free survival (PFS) was calculated from the date of diagnosis to the date of documented disease progression, date of last follow-up visit or time of death. Survival curves were estimated by the Kaplan-Meier method.
Baseline characteristics
Between January 2002 and September 2014, 29 patients (17 female and 12 male) with newly diagnosed PMBCL were treated at our department. The median age at the time of diagnosis was 36 years (18-79 years). The median follow-up was 51,5 months (02- 123 months). Eighteen (62.1%) and 20 (69%) patients had limited-stage disease and bulky disease, respectively. Most patients presented with high LDH. Patient characteristics are resumed in Table 1.
| Age, years Median, (min, max) | 36 (18-79) |
| Male gender, n (%) | 12 (41.4) |
| LDH>UNL (%) | 24 (82.8) |
| B symptons, n (%) | 12 (41.4) |
| Ann Harbor, n (%) I-II | 18 (62.1) |
| III-IV | 11(37.9) |
| Mediastinal massMedian, mm (min, max) | 9.5 (4-18) |
| Bulky, n (%) | 20 (69%) |
| Consolidative RT, n (%) | 21 (72.4) |
| ASCT, n | 7 (24.1) |
| CR1 | 6 |
| CR2 | 1 |
| Histochemistry, n (%, n=28) | |
| CD20 | 28 (100) |
| BCL-6 | 19 (67.9) |
| MUM1 | 16 (57.1) |
| CD23 | 12(42.9) |
| BCL-2 | 14 (50) |
| CD45 | 06 (21.4) |
| CD30 | 04 (14.3) |
Table 1: Demographic, clinical immunohistological data of 29 patients with PMBCL treated at our department between May 2002 and September 2014. Abbreviations: ASCT: Autologous Stem-Cell Transplant; LDH: Lactate Dehydrogenase; Min: Minimum; Max: Maximum; RT: Radiotherapy; UNL: Upper Normal Limit.
Effectiveness and safety
Rituximab-based combination regimens included: R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone, n=26), R-HCVAD (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone, n=2) and R-CHOEP (rituximab, cyclophosphamide, doxorubicin, vincristine, etoposide and prednisolone, n=1). Twenty-one and six patients underwent consolidation RT and ASCT, respectively. One patient, with advancedstage disease, did not undergo consolidation therapy due to comorbidities. The remaining patient, also with advanced-stage disease, showed progressive disease. He was given second-line therapy consisting of ESHAP (etoposide, methylprednisolone, cytarabine and cisplatin) but eventually died of respiratory failure in intensive care unit after the first cycle.
At the end of treatment plan, 27 patients achieved complete response (CR) and one patient achieved only partial response. This patient had been initially treated with six cycles of R-CHOP followed by RT and developed pericardial effusion early after treatment. He did not respond to salvage therapy and died of progressive disease eleven months after diagnosis. During immunochemotherapy, febrile neutropenia and intestinal perforation were observed in three and one patients, respectively. So far, RT has been well tolerated, leading to pneumonitis (n=2) and hypothyroidism (n=1). Five patients presented complications in the post-transplant period: infectious complications [febrile neutropenia (n=2), cellulitis (n=1) and central venous catheterrelated bacteremia (n=1)], mucositis (n=1) and hemorrhagic cystitis (n=1). None developed secondary malignancies.
Follow-up
Two patients relapsed. The patient that did not receive consolidation therapy relapsed 26 months after diagnosis, responded poorly to second-line therapy and died nine months later. The other patient relapsed 18 months after diagnosis, achieved CR after second-line therapy consisting of ESHAP followed by ASCT. Overall, seven patients were transplanted; six in CR1 and the remaining in CR2. Except for one patient, all transplanted patients were alive with documented CR at the time of last visit. Overall, 25 patients were able to be maintained in CR and four patients died, half of which died within 12 months of diagnosis: three deaths were due to progression of disease and the remaining was related to transplant (within 60 days after transplant not related to the disease, relapse or progression). Estimated 5-year OS was 84.2% (Figure 1).
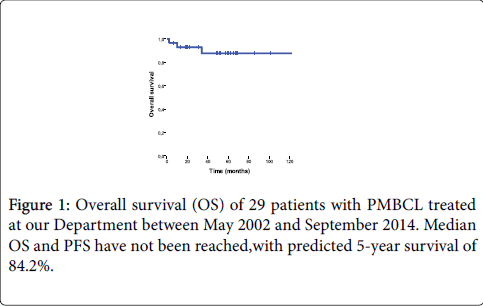
Figure 1: Overall survival (OS) of 29 patients with PMBCL treated at our Department between May 2002 and September 2014. Median OS and PFS have not been reached,with predicted 5-year survival of 84.2%.
At a median follow-up of 51,5 months, median PFS has not been reached (Figure 2). Estimated 5- year PFS was 83.8%.
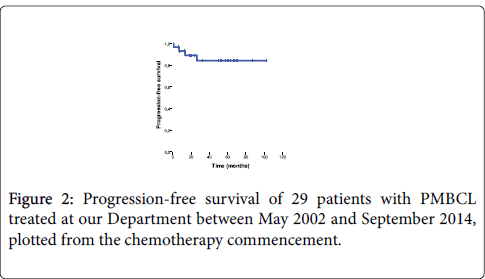
Figure 2: Overall survival (OS) of 29 patients with PMBCL treated at our Department between May 2002 and September 2014. Median OS and PFS have not been reached,with predicted 5-year survival of 84.2%.
In our cohort, PMBCL affected slightly more female than male patients and was characterized by bulky mediastinal disease with frequently elevated LDH and B symptoms. According to recent gene expression profiling studies, PMBCL has more in common with nodular sclerosis HL than with other subtypes of DLBCL [12,13]. Although its clinical and immunohistochemical features are well characterized, there is ongoing debate around several aspects of its treatment plan including optimal induction regimen and the role of consolidation RT and ASCT.
The treatment of PMBCL with standard CHOP or CHOP-like (with or without radiation therapy) showed relatively low rates of CR and OS (50-60%) [14,15]. Rituximab in combination with chemotherapy has revolutionized the treatment paradigm of PMBCL. Our study demonstrated good response rates and survival outcomes with rituximab-based combination chemotherapy similar to those reported by the British Columbia group [8]. These authors reported a 5-year OS of 88% in 96 patients treated with R-CHOP. Similar results were obtained from a multicenter study in Greece [9]. More aggressive treatment approaches (so-called third-generation regimens) such as VACOP-B (methrotrexate, doxorubicin, cyclophosphamide, vincristine and bleomycin) achieved excellent results in early studies [16-18]. However, a phase III comparison of CHOP with three different thirdgeneration regimens for the treatment of intermediate and high-grade non-Hodgkin lymphoma found no significant differences among them [19]. More recently, the National Cancer Institute group presented very encouraging data regarding DA-EPOCH-R in a phase II trial that included 51 patients. At a median follow-up of 5 years, the event-free survival and OS rate was 93% and 97%, respectively [7]. Logistical administration issues of DA-EPOCH-R compared with R-CHOP may represent a drawback of the former regimen. Although these results are promising, the superiority of continuous infusional chemotherapy over R-CHOP has still to be proved in large randomized trials and any potential benefit must be balanced against toxicity. A small randomized phase III trial showed no superiority of infusional EPOCH for aggressive non-Hodgkin lymphoma [20].
PMBCL is radiosensitive and frequently limited to the mediastinum. The mediastinum is also the most frequent site of relapse so RT has been routinely applied. Although being insufficient therapy for patients with high risk disease, RT may be an effective local treatment in limited-stage disease. Despite the long follow-up of published studies, very few have reported on toxicity. Zinzani et al evaluated safety and tolerability of a cohort of 74 patients in which 70% received RT and adverse events were predominantly hematological (neutropenia and thrombocytopenia). In our cohort, we observed eight cases of toxicity, but only three (pulmonary disease and hypothyroidism) are most likely secondary to RT. Brusamolino et al. monitored late events and causes of death over 15 years in a cohort of patients with HL treated with a combined modality (chemo and radiation therapy). The risk of cardiovascular events, pulmonary toxicity and secondary neoplasia at 12 years was 14%, 8% and 8%, respectively, with a median latent time of 67 months, 76 weeks and 45 months [21]. Although data on PMBCL is still limited, complications of mediastinal RT cannot be underestimated.
The management of residual mediastinal masses post-chemotherapy is also controversial due to the prominent fibrotic component of PMBCL. The performance of PET scan in detecting viable tumor after rituximab-based combination chemotherapy and its prognostic value in patients planned for consolidation RT was recently assessed. A negative test was associated with a 99% negative predictive value and consequently excellent outcomes. However, the positive predictive value was poor (ranging from 18 to 32% for different cut-off values) [22]. To minimize its false positive rate, PET scans are recommended to be performed at least 3 weeks (preferably 6 to 8 weeks) after the last cycle of chemotherapy [11]. An ongoing phase III study from International Extranodal Lymphoma Study Group (IELSG) is aimed to evaluate whether consolidation RT should be individualized based on PET features (IELSG-37 trial, NCT01599559). This trial is expected to be complete in 2015 and, until IELSG publishes their final results, RT should be considered in all patients regardless of PET scan.
Since PMBCL lacks bone marrow involvement, high-dose chemotherapy supported by ASCT has been used as consolidation therapy in high-risk patients. In the pre-rituximab era, ASCT achieved prolonged survival in 80-90% of patients presenting with high-risk features [23-25]. Currently, it is hard to define ASCT as primary consolidation therapy given the excellent results already obtained with new induction regimen and transplant-related toxicity. Many centers are now reserving ASCT to patients with relapsed/refractory disease in which this procedure may offer a probability of cure. Overall and progression-free survival in patients with relapsed/refractory disease ranges 49-71% and 42-58%, respectively, showing that ASCT can provide durable remissions in these patients [23,26]. Interestingly, not receiving local radiotherapy showed a negative impact on the survival outcomes of transplant [23,26].
Four of our patients had refractory or relapsing disease. Three of them did not respond to salvage therapy and died of progression of their lymphoma. Our results are similar to those reported by other authors. The majority of relapses in PMBCL patients occurs within 12 months and is rare beyond two years from completion of therapy. Prognostic factors have been reported inconsistently in the literature. Retrospective studies have suggested that factors such as LDH level, male sex, performance status and advanced-stage disease may be useful predictors of survival but they lack validation in prospective studies. In a recent study by Aoki et al., IPI and the presence of pleural and pericardial effusion were the only adverse prognostic factors for risk stratification of PMBCL patients [27].
The biology of PMBCL is being increasingly deciphered. Abnormalities on chromosome 9p have been reported in up to 75% of PMBCL patients and seem to have an important role in the pathogenesis of this lymphoma. This region encodes Janus kinase 2 which fosforilates and activates the transcription factor signal transducer and activator of transcription (STAT) 6 [13]. Programmeddeath ligands (PDL) 1 and 2 are also localized in 9p region and are frequently rearranged. These new targets may eventually lead to the development of novel therapies [13]. Agents such as JAK-STAT pathway inhibitors and neutralizing antibodies to PD1 are on the move and have shown promising results both in vitro and in vivo [28,29]. Bcl-6 plays an important role enabling the survival of B-cells and was found to be expressed in two thirds of our cohort, representing another potential target for novel rationally designed therapies. CD30 is more variably expressed in PMBCL and may constitute a critical target for brentuximab vedotin. This antibody drug conjugate against CD30 showed favorable results in patients with relapsed HL, leading to his recent conditional approval by regulation agencies in Europe, and is currently being studied in PMBCL [30].
This study reviewed our experience in the treatment of patients with PMBCL. Most patients underwent consolidation RT or ASCT with favorable response rates and outcomes. Whether infusional chemotherapy is superior to standard R-CHOP and whether RT should be individualized based on PET and or other clinical or prognostic features remain unclear. A small number of patients was refractory or relapsed after treatment and had a dismissal prognosis. Further studies are required to identify risk factors for progression in order to establish individualized therapeutic strategies.
This study was performed at the Department of Onco-Hematology, Portuguese Institute of Oncology - Porto, Portugal.