Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2015) Volume 5, Issue 1
Objectives: to evaluate the effectiveness of a three-year workplace intervention for healthy lifestyle promotion in the prevention of hypertension among employees.
Methods: A quasi-experimental study design was employed to assess the effectiveness of a health promotion intervention program for corporate employees, which mainly consisted of educational videos and interactive teaching sessions with occupational physicians, healthy eating and smoking cessation workshops, free physical activity sessions for employees and free smoking cessation consultation in workplace. There were three workplace sites in the intervention and control groups, respectively.
Results: The prevalence of screened hypertension decreased significantly in the intervention arm from 16.2% to 12.8% (p=0.02), but increased significantly in the control arm from 13.3% to 23.3% (p<0.001). Of note, obesity increased both in intervention and control arms. Assessment of hypertension prevalence according to weight status demonstrated a significant decrease in the intervention group among normal weight participants from 11.5% to 6.6% (p=0.009), but an increase in the control group albeit not statistically significant. Among overweight participants, hypertension decreased in intervention group from 18.9% to 13.5% (p=0.058), but increased significantly in control group from 13.1% to 23.1%
(p=0.001). Among obese participants, the decrease in the prevalence of hypertension was not significant in intervention group (27.8% to 24.4%, p=0.48), however, it increased significantly in the control group from 22.4% to 34.3% (p=0.009). Determinants of hypertension were age > 35 years, male sex, overweight and obesity in the two groups. Overall, the intervention was negatively associated with hypertension in intervention group (OR= 0.61, CI 95% [0.47-0.8]).
Conclusion: The intervention program was effective in decreasing the prevalence of hypertension among normal weight workers. However, additional strategies and/or time are need to combat hypertension among overweight and obese individuals.
Keywords: Workplace; Intervention; Prevention; Hypertension; Obesity; Chronic disease
In 2009, the World Health Organization (WHO) attributed 13% of all deaths globally to high blood pressure, making it an issue of prime public health importance for both developing and developed nations [1].Tunisia exemplifies the reason for the WHO sentiments because hypertension now affects more than 30% of adults as part of an evolving epidemiological transition within the African region [2-4]. High blood pressure is preventable, and is directly related to lifestyle habits such as poor diet, low levels of physical activity, tobacco use, and obesity. These behavioral risk factors are responsible for about 80% of serious heart conditions [5]. Hypertension has long been recognized as a modifiable health risk that can be addressed the worksite [6]. Goetzel et al. [7] recently estimated the cost of health, absenteeism, short-term disability, and productivity losses for 10 health conditions using combined findings from several surveys; and found that the overall economic burden of illness was highest for hypertension [8].
The worksite is a setting that offersgreat potential for health promotionbecause of access to a captive cohort, the opportunity for follow-up, and the ability of employers to modify the work environment so it could be ideal for risk factor prevention [9]. Fortunately, workplace health initiatives around the world are growing in number and scope, as employers come to realize that addressing employee health and wellness is linked to increased productivity and reduced absenteeism [10], and that the return on this strategic investment and overall health cost savings are high [11]. Consequently, during the past few decades, in both the USA and inEuropean countries, worksite health promotion programs have increasingly was implemented [12,13]. Mainfactors addressed in such programs involve physicalactivity or fitness, nutrition, and tobacco use. It was demonstrated that these programs on cardiovascular risk factors can be implemented and can have a positive impact on intermediate cardiovascular disease outcomes in developing countries [14]. The effectiveness of such intervention depends on the programs, their duration and the risk factors profile of participants [9,15-17]. In Tunisia, few worksite interventions have been implemented to prevent hypertension, and they were of limited duration.
In this context, this study was designed to evaluate the effectiveness of a three-year workplace intervention for healthy lifestyle promotion in the prevention of hypertension among employees.
Study design
In Sousse Tunisia we conducted a quasi-experimental study (pre and post-tests with intervention and control groups) from 2009 until 2014 to evaluate the effectiveness of an intervention implemented at a workplace. The purpose of this intervention was to decrease chronic disease risk factors (tobacco use, unhealthy diet and lack of physical activity) and hypertension among workers. However, this report is focused only on hypertension. The intervention group included workplaces located in the delegations of Sousse Jawhara and Sousse Erriadh, while the control group was from workplaces located in the neighboring delegation of Msaken (Figure 1).
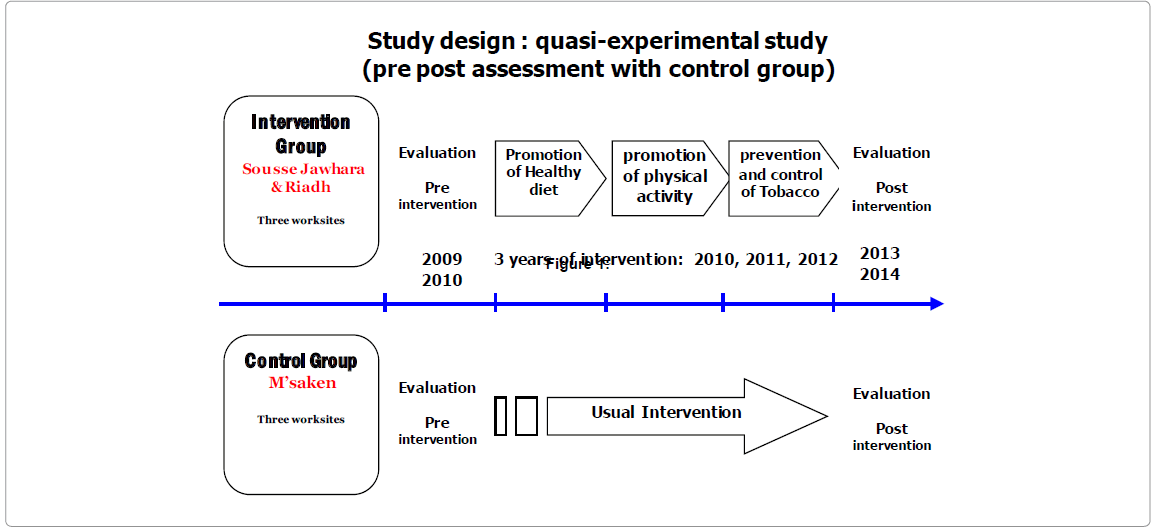
Figure 1:
Studied population
The study population comprised workers in 6 enterprises: 3 in each group. Sample size calculation was based on a significance level (α) of 0.05%, a power (β) of 20%, two-sided test of hypothesis and 6% change in risk factor level (smoking, unhealthy diet and physical inactivity) giving a total sample of 1000 workers per group. We selected a convenience sample of 6 enterprises with similar characteristics regarding the total number of workers and sex composition. The six participating enterprises included textile, car part factories (cable, tire) and food factory. Employees were between ages of 18 to 60 years. Sex demographic varied between worksites in each group, with a majority of males in one site, a majority of females in another and almost equal distribution in the third one. The same distribution was chosen in the intervention and control groups. All workers in Tunisia are required to have a medical assessment prior to beginning a job therefore they are of general good health.
A small proportion of the population belongs to an administrative type job while the majority the rest varied in amount of physical demand. In the food factory in particular, job was more physically demanding than the other settings.
All workers in both groups were invited to participate. The pre and post intervention evaluation concerned two independent samples in the same worksites.
Data collection
We used a pre-tested and standardized questionnaire to evaluate knowledge, attitudes and beliefs about three risk factors for chronic disease: unhealthy diet, physical inactivity and tobacco use. Anthropometric measurements (weight, height, and waist circumference) and blood pressure were taken at baseline and post intervention. Blood pressure was measured by medical doctors twice with digital monitor at rest. The mean value of two measures was used to define high blood pressure. So, our results present a screening of hypertension and not a diagnosis.
All measurements were taken at the worksite. To define overweight and obesity, we used the international BMI cut-off values according to the WHO [18]. The recommended normal blood pressure was as defined by WG-ASH [19].
Intervention program
From September 2010 until September 2013, the intervention group received educational videos, underwent participatory instructional sessions with occupational physicians, animation workshops about healthy diet and motivation to quit smoking, workplace sensitization targeted at three risk factors (smoking, physical activity, diet), free physical activity sessions for employees and free smoking cessation consultations in workplace. Specially designed pamphlets were distributed to the intervention participants in addition to other kind of materials such as posters and streamers. All intervention activities and materials were adapted to socioeconomic and cultural habits of employees. At the end of the study period the same health education program was made available to all participants that were in the control group. All the activities were conducted at the worksite during work hours in order to encourage employee participation; however effort was made to ensure that they were taken away from their duties for too long.
The control group continued to have the existing interventions which are very limited and could consist just on some advices from occupational doctors.
Data analyses
Statistical analysis was performed using the SPSS 10.0 software. We used descriptive statistics (frequencies, means and standard deviations) and chi square test to compare categorical variables. A two-tailed p-value of < 0.05 was considered the threshold for statistical significance. The presence of hypertension was coded as yes or no; consequently binary logistic regression models were used to identify the determinants of hypertension in the study. The variables used in the model were: the effect of intervention (which was coded as pre intervention or post intervention), age, sex and weight status.
Ethical considerations
This study was undertaken with respect for the rights and integrity of the participants. Ethical clearance was obtained from the Ethical Committee of Farhat Hached University Hospital. Participation was voluntary and all the participants gave informed consent.
The baseline questionnaire completion rates were76.7% and 72.5% in intervention and control groups, respectively; and 69.7% and 77.5% respectively at post intervention. At baseline, the population was composed of 1775 workers with 914 in the intervention group and 861 in the control group. The intervention group was composed of 64.7% men with a mean age of 32.25 ± 8.1 years, while the control group comprised 59% men with a mean age of 35.40±8.8 years. At post intervention (study completion), there were 2113 study participants: 1098 (65.5% men) in the intervention group with a mean age of 33.86 ± 8.1 years, and 1015 (61.4% men) in the control group with a mean age of 38.90 ± 8.8 years.
The prevalence of hypertension decreased significantly in intervention group from 16.2% to 12.8% (p=0.02), but it increased significantly in control group from 13.3% to 23.3% (p<0.001). This pattern was consistent for both men and women: from 17.9% to 14.3% (p=0.08) among men and from 13.1% to 9.8% (p=0.16) among women in the intervention group. In the control group, hypertension increased significantly from 17.1% to 29.6% among men (p<0,001) and from 7.7% to 13.3% (p=0.01) among women (Table 1).
| Intervention group | Control group | ||||||
|---|---|---|---|---|---|---|---|
| Pre n(%) | Post n (%) | p | Pre n (%) | Post n (%) | p | ||
| Men | Overweight | 190 (32.5) | 264 (36.8) | 0.11 | 207 (43.1) | 264 (42.7) | 0.89 |
| Obesity | 71 (12.2) | 120 (16.7) | 0.02 | 107 (22.3) | 162 (26.2) | 0.13 | |
| hypertension | 105 (17.9) | 103 (14.3) | 0.08 | 86 (17.1) | 184 (29.6) | <0.001 | |
| Women | Overweight | 91 (29.4) | 122 (32.4) | 0.39 | 101 (29.6) | 143 (37.1) | 0.03 |
| Obesity | 63 (20.3) | 105 (27.9) | 0.02 | 54 (15.8) | 112 (29.1) | <0.001 | |
| hypertension | 41 (13.1) | 37 (9.8) | 0.16 | 26 (7.7) | 52 (13.3) | 0.01 | |
Table 1: Hypertension and excess of weight in the intervention and control groups after workplace intervention to reduce cardiovascular risk factors in the region of Sousse Tunisia, 2009/2014.
Obesity increased significantly in the intervention group from 15.2% to 20.7% (p=0.001), and from 19.7% to 26.3% (p<0.001) in the control group at post assessment. According to sex, obesity increased significantly in intervention group among both men and women, but in the control group it increased significantly only among women (Table 1).
Hypertension decreased significantly in intervention group among normal weight participants from 11.5% to 6.6% (p=0.009), however it increased but not significantly in control group. Among overweight participants, hypertension decreased in the intervention group from 18.9% to 13.5% (p=0.058) and increased significantly in the control group from 13.1% to 23.1% (p=0.001). Among obese participants, hypertension decreased but not significantly in the intervention group from 27.8% to 24.4% (p=0.48), but increased significantly in the control group from 22.4% to 34.3% (p=0.009) (Table 2).
| Intervention group | Control group | |||||
|---|---|---|---|---|---|---|
| Hypertension | Pre n(%) | Post n (%) | p | Pre n (%) | Post n (%) | p |
| Normal weight | 55 (11.5) | 32 (6.6) | 0.009 | 32 (9.2) | 45 (14.0) | 0.056 |
| Overweight | 53 (18.9) | 52 (13.5) | 0.058 | 40 (13.1) | 94 (23.1) | 0.001 |
| Obesity | 37 (27.8) | 55 (24.4) | 0.480 | 36 (22.4) | 94 (34.3) | 0.009 |
| Age <35 years | 80 (12.3) | 58 (8.3) | 0.01 | 41 (9.5) | 54 (14.2) | 0.04 |
| Age >35 years | 64 (26.8) | 82 (20.6) | 0.07 | 71 (17.8) | 182 (28.7) | <0.001 |
Table 2: Hypertension in the intervention and control groups by age and weight category after workplace intervention to reduce cardiovascular risk factors in the region of Sousse Tunisia, 2009/2014.
Factors associated with hypertension post assessment were age > 35 years, male sex, overweight and obesity. The intervention was negatively associated with hypertension (OR= 0.61, IC95% [0.47- 0.8]) (Table 3).
| Intervention group | Control group | |||
|---|---|---|---|---|
| OR | CI 95% | OR | CI 95% | |
| Intervention affect | 0.61 | 0.47 - 0.80 | 1.76 | 1.36 - 2.28 |
| Age >35 years | 2.23 | 1.70 - 2.92 | 1.59 | 1.20 - 2.11 |
| Sex (men) | 1.56 | 1.16 - 2.09 | 2.35 | 1.76 - 3.15 |
| Overweight | 1.76 | 1.29 - 2.40 | 1.39 | 1.02 - 1.91 |
| Obesity | 3.39 | 2.41 - 4.79 | 2.62 | 1.88 - 3.64 |
Table 3: Determinants of hypertension in intervention and control group after workplace intervention to reduce cardiovascular risk factors in the region of Sousse Tunisia, 2009/2014.
We have demonstrated that a three-year worksite health promotion intervention program for hypertension control was feasible and we noticed a significant decrease of the proportion of hypertension in intervention group among employees, but this improvement was seen mainly among normal weight participants. Elderly participants and men had higher risk of hypertension. The intervention consisted mainly of individual and group education to prevent and decrease main risk factors such as tobacco use, unhealthy diet and lack of physical activity. Worksite health promotion initiatives often develop strategies based on educating employees at risk [20-24]. Although education is an important component of effective health promotion, education alone may be insufficient to modify health risks that tend to be habitual, chronic behaviors such as unhealthy eating and lack of exercise, or powerful environmental determinants [25]. In this context, the workplace represents a critical setting for health promotion [26] due to potential direct influence on employee health [27], however to be effective it should incorporate behavioral, environmental and policy approaches [28].
Other recommendation for successful interventions includes the importance of targeting multiple risk factors, specifically those that represent the highest disease burden in the region where the workplace is located [29]. In fact, Tunisia is actually facing an epidemiological transition and adults are at high risk of chronic diseases and their risk factors such as hypertension [2-4]. Furthermore, workplace health initiatives need to be underpinned by management buy-in and employee ownership, and targeted to each unique workplace and cultural setting [29].In our intervention, we tried to adapt the intervention program to cultural habits of participants particularly regarding physical activity and eating habits.
Different dietary regimens for blood pressure control have been proposed. Dietary Approaches to Stop Hypertension (DASH) diet permitted substantial blood pressure control in persons with prehypertension or stage 1 hypertension [30]. In Japan, a non-randomized controlled trial demonstrated that Japanese-style healthy workplace lunch aimed to prevent and/or improve metabolic syndrome among middle-aged men decreased blood pressure and serum lipids [31]. The potential value of promotingthe health of employees within individual businesses is well known [20], and the obesity epidemic has substantial implications for employers [22].The presence of obesity increases the likelihood of several chronic conditions, including hypertension [32,33]. Obesity is associated with increasedrisk of mortality [34], excess costs [35], and reduced productivity [36]. That’s why, it’s important to follow recommendations to reduce obesity. The effectiveness of the intervention program to decrease hypertension could be easier among normal weight workers who had less risk factor.
Interventions to change the lifestyle include mainly guidelines, training courses, movement training, cognitive behavior therapy, nutrition interventions, information campaigns, and focus groups [37]. Compared to a normal diet, nutritional advice has only small effects on weight loss, which further is reduced in the course of time. As a result, cognitive behavior therapy can have an influence on nutrition and physical activity and this can result in more permanent weight loss benefits [37]. This approach could be incorporated into future workplace interventions to decrease obesity in Tunisia. The sustainability of a prevention measure must be ensured, thus long-term studies are necessary to make valid statements regarding the sustainable effectiveness [37]. The nonrandomized design is the major limitation of this study. Also, the use of pre post design couldn’t pass by the impact of secular trends. However, comparison of the intervention group with a comparable control industrial population improved the quality of the results. Furthermore, we are unaware of the long-term effect of the intervention and the continuity of some interventions by the occupational physicians who were trained during this program. In this study, it was necessary to offer a minimal intervention to the control (comparison) worksite for ethical reasons. It consisted of open days for healthy eating and physical activity promotion.
It seems that hypertension decrease is more feasible among normal weight workers. To achieve a greater impact of worksite healthpromotion, future strategies should aim at providinga more condutive environment to facilitate individual behavior change. Managementshould support individualized interventions byimplementing or modifying some work policiesthat promote and sustain healthy lifestylebehaviors.
This project was funded by UnitedHealth Group and NHLBI Chronic Disease initiative.