Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2014) Volume 2, Issue 3
Objective: To evaluate the decision making of gynecologists in a clinical setting regarding the diagnosis and management of endometriosis. Design: A qualitative questionnaire-based study. Setting: Two local meetings of gynecologists. Participants: Gynecologists in a community and a hospital setting. Intervention: None. Main outcome measure: Physician’s reported management and treatment methods. Results: The questionnaire was answered by 91 gynecologists. Most had at least 10 years of clinical experience (72.2%), 37.8% were community-based, and 5.6% were ultrasound experts. Approximately 62.8% of physicians believe that there is delayed diagnosis of endometriosis. Most would refer the patient to a specialized endometriosis center in the presence of a large pelvic mass, following repeated IVF failure, or due to intractable pain after repeat surgery. Physicians’ seniority or subspecialty did not significantly influence their opinions. Conclusion: It seems that it is not delayed diagnosis that affects the management of endometriosis, but rather delayed referral to targeted investigation and appropriate treatment. Gynecologists in community practice are still largely unaware of the role of specialized care in the management of endometriosis.
<Keywords: Endometriosis, Laparoscopy, Delayed diagnosis, Community care, Treatment
Endometriosis is a common gynecological disorder, which affects 5-15% of women of reproductive age [1]. The prevalence of endometriosis varies depending on the population in question and the presence of infertility [2-7]. It has an unpredictable rate of progression [8]. The chronic nature and severity of endometriosis often leads to deterioration in quality of life and high psychological morbidity [9,10]. Epidemiological studies reveal a high prevalence of chronic pelvic pain in community care settings, with almost half of these women diagnosed as having endometriosis [11].
The diagnosis of endometriosis remains a clinical challenge with many patients left undiagnosed for many years. The gold standard for diagnosis of endometriosis is surgery, which is advocated as a second line investigation in the event of failed therapeutic intervention for the management of chronic pelvic pain [12]. A significant diagnostic delay is often reported with an estimated average delay of 7 years in the USA, 8 years in the UK [10,13], 10.4 years in Austria and Germany [14] and 6.7 years in Norway [15]. Two thirds of women with endometriosis are initially misdiagnosed and almost half are examined by five physicians or more before a correct diagnosis is made [16]. The delay is significantly longer in women presenting with pelvic pain in comparison to those presenting with infertility [10,17,18]. Furthermore, the delay before surgical diagnosis of deep infiltrating endometriosis is significantly longer for patients with advanced stage IV disease than for those with stage I, II or III disease [19]. The endometriosis-associated costs to society are aggravated by delayed diagnosis and ‘hit-and-miss’ treatments, as are the costs to the individual when disease symptoms interfere with daily function [10,20,21].
Ballard et al. investigated possible reasons for this delay utilizing a qualitative questionnaire given to women attending a pelvic pain clinic [22]. These authors found that delays in the diagnosis of endometriosis occur at an individual patient level and at a medical level. Women endured symptoms due to inaccurate perception of normal versus abnormal pain, embarrassment, endurance and individual coping strategies; while family doctors tend to normalize symptoms, symptoms are intermittently suppressed through hormones and nondiscriminatory investigations such as a normal transvaginal scan are relied upon. They highlighted the importance of an early diagnosis for women who suffer at physical, emotional, and social levels when they remain undiagnosed. Other possible reasons for this delay may be related to a lack of awareness or knowledge, or simply lack of confidence in surgery results. Early diagnosis of endometriosis refers, by definition, to early surgery, since surgery is the gold standard for diagnosis. But early surgery is not advocated for all patients. In certain cases, empirical treatment is strongly recommended. Therefore the focus of our questionnaire was to investigate whether there is a delay in the administration of appropriate treatment and to investigate the accepted indications for surgery.
Gynecologists in Israel serve as primary care providers, and therefore often serve as the first physicians seen by the patient presenting with symptoms of endometriosis. The aim of this study was to evaluate how practicing gynecologists perceive their role in the diagnosis and management of endometriosis and to ascertain whether they may contribute to diagnostic delay. Furthermore, we sought to assess the knowledge and acceptance of the concept of specialized endometriosis referral centers.
This is a qualitative study consisting of a structured questionnaire that was given to gynecologists attending two gynecological meetings in Israel during 2011: A Community Gynecology (CG) conference and a Gynecological Endoscopy (GE) conference. Since no patients were involved in this study, approval by the institution’s review board was not sought. Physicians could reply anonymously and privately. The questionnaire consisted of sixteen questions, the first three relating to the demographical characteristics of the responders followed by thirteen questions about the clinical knowledge and management practices of patients with chronic pelvic pain and endometriosis (Supplement 1).
Data analysis and statistics were performed by “P-value,” a private statistical company. Additional statistics were performed by VHE and AYW. None of the physicians involved in this study received any funding or compensation. Distribution of the questionnaires and the statistical analysis were funded by an unrestricted grant from Bayer pharmaceuticals.
Ninety one gynecologists completed the questionnaire during two gynecological meetings; sixty seven in a CG meeting (73.6%) and 24 in a GE meeting (26.4%). Almost half of the responders (47.7%) were primary community gynecology caregivers, either as their primary professional activity or in combination with other professional activities (such as: obstetrics, gynecological surgery and ultrasound). More than a quarter (25.6%) reported being gynecological surgeons, 11% fertility specialists, and 5.6% physician-sonographers (Figure 1). Most of the responders (44.4%) had more than 20 years of clinical experience, 27.8% had between 11 and 15 years of experience, and the rest were actively practicing for 10 year or less.
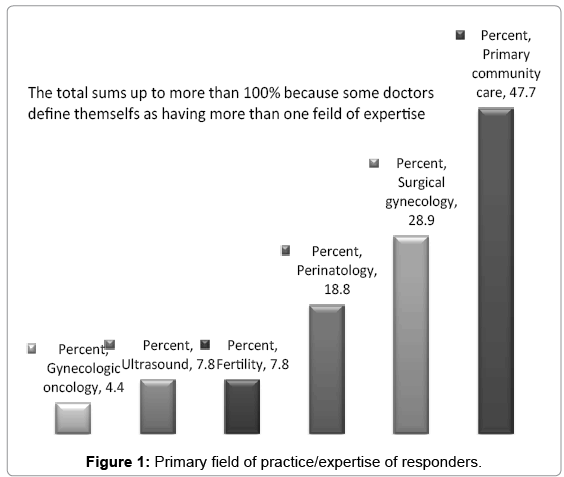
Figure 1: Primary field of practice/expertise of responders.
When asked about the prevalence of reproductive age women suffering from severe dysmenorrhea, the vast majority of responders (91%) believed that 6-20% of women suffer from this disorder. Physicians with greater professional experience (>10 years vs. <10 years) tended to give a higher estimation of the rate of reproductive age women suffering from severe dysmenorrhea (χ2=8.34, p<0.05), but the estimated rate did not vary according to primary subspecialty (χ²=2.58, p=0.27).
About a third of the responders believe that endometriosis accounts for pain in only 5-10% of reproductive age women suffering from severe dysmenorrhea. Another third believe that this rate is higher than 20%, while more than half of these believe that this rate is higher than 40%.
Most doctors (70.3%) agree that the prevalence of women suffering from endometriosis has increased in recent years. More than half of them (56%) attribute this rise to increased physician awareness of endometriosis, whereas only 6.6% believe that there is an actual increase in prevalence of the disease.
The subsequent questions pertained to actual clinical situations and their preferred management. The responders were asked about the first line therapy for a 24 year old single woman with severe debilitating dysmenorrhea who does not desire fertility: The vast majority (almost 95%) agreed that oral contraceptive pills (OCP) were the treatment of choice but they varied in their administration practices (67.0% continuous and 27.5% cyclic use).
When asked about the best second line treatment for the same patient, approximately one third of responders (31.1%) advocated performing a diagnostic and definitive care laparoscopy, 28.9% suggested resorting to continuous OCP treatment, while the remaining chose other treatment modalities such as Levonorgestrel intrauterine device (Mirena, 13.3%), progestins (12.2%), GnRH agonists (4.4%). Some 3.3% thought that the best management was attempting pregnancy as soon as possible even though the patient was a single 24 year old woman.
Over 40% of responders reported that in their experience, more than 10% of women do not improve after OCP treatment, whether cyclic or continuous, and about a fifth believed this rate exceeded 20% of women. This belief differed significantly by main practice location, namely that hospital-based gynecologists reported a higher rate of women not improving after OCP treatment (χ²=13.32, p<0.05).
When asked whether there was a significant delay in the diagnosis of endometriosis, almost two thirds of responders believed that indeed there was. This was mainly attributed to low awareness but also to the absence of a valid simple non-invasive diagnostic test.
Each responder was asked to estimate the average amount of women with a clinical suspicion of endometriosis that he sees per month. More than half (58.6%) claimed to see 3-5 endometriosis patients a month. Another 25.3% reported seeing 6-10 endometriosis patients a month, 9.2% reported seeing more than 10 endometriosis patients a month, and only 6.9% reported seeing 1-2 endometriosis patients per month.
When asked whether delayed diagnosis causes any harm to patients, almost a half of the responders (48.8%), believed that earlier diagnosis of endometriosis cannot prevent the course of the disease since there is no effective treatment. On the other hand, 41.7% acknowledged that delayed diagnosis of endometriosis can harm their patients: namely, 27.4% believe that earlier diagnosis of endometriosis can prevent disease progression and 14.3% believe that earlier diagnosis can prevent fertility impairment. A small but significant percentage of responders (8.8%) did not know whether there was any impact on patient wellbeing. Interestingly, the more experienced gynecologists were more likely to believe that there was no impact to delayed diagnosis (χ²=5.10, p<0.05).
When asked about the optimal treatment for endometriosis, the majority of doctors (44.8%) thought that conceiving as soon as possible is the best treatment for endometriosis (Figure 2). Surprisingly, less than 20% recommended using a medication that was proven in randomized controlled trials to improve quality of life and prevent pain in endometriosis patients. Only 3.4% thought that the patient should be offered surgery and even that, was only under the assumption that during surgery all lesions could be removed.
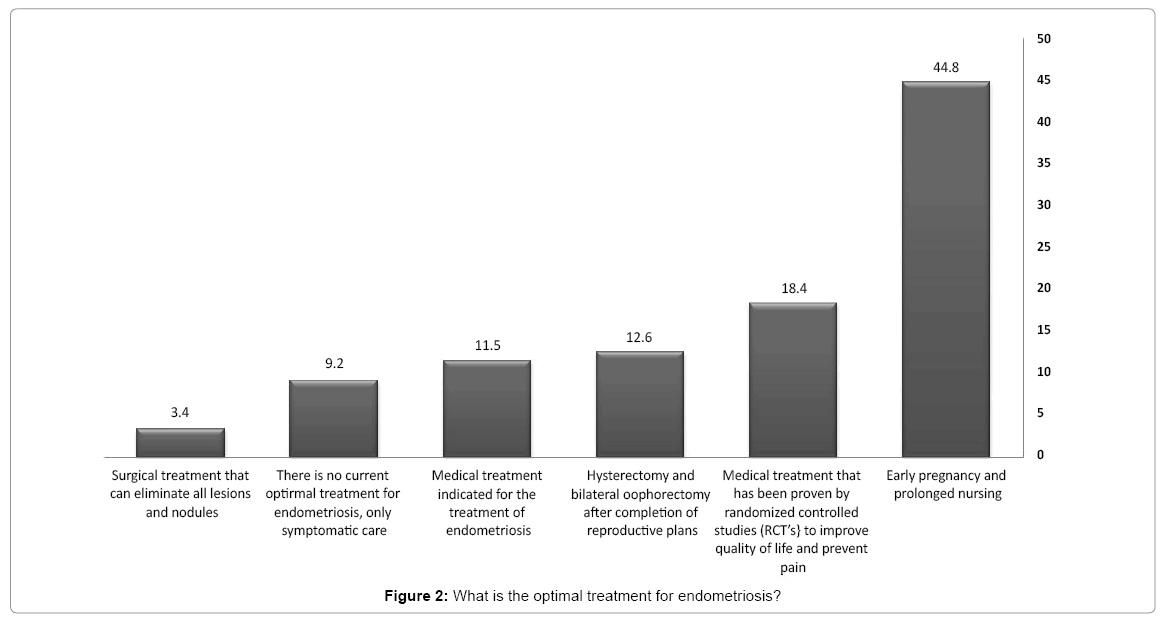
Figure 2: What is the optimal treatment for endometriosis?
The physicians were asked about the criteria for referral to a specialized endometriosis clinic or center of excellence (Figure 3). The vast majority of physicians would refer women in the presence of significant clinical problems, such as large pelvic masses and a significant increase in CA-125 levels, repeated In Vitro fertilization (IVF) failures, refractory pain after repeated surgery, or significant involvement of other organs, such as intestines and urinary bladder. Only 2.3% thought that there is no need for such a clinic or center.
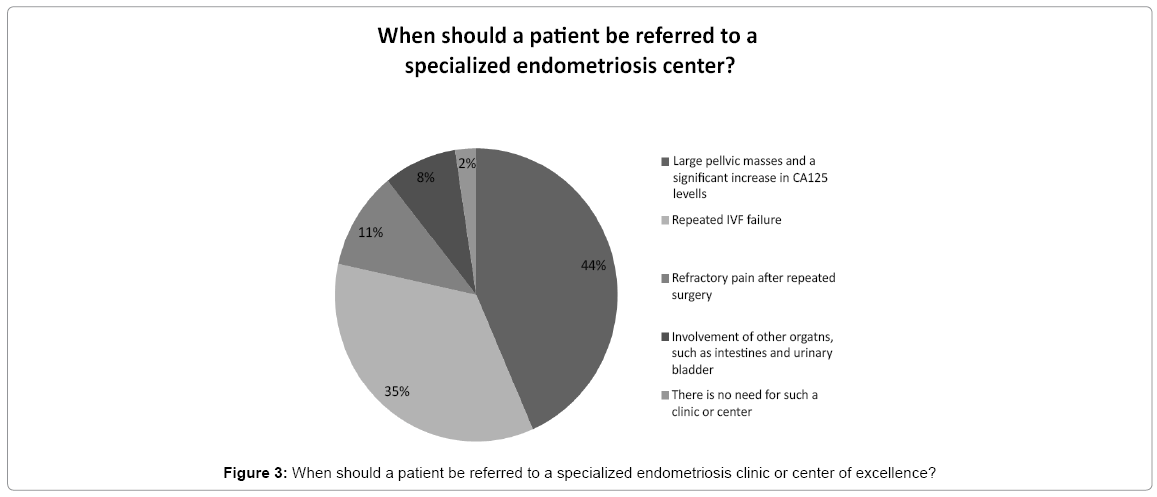
Figure 3: When should a patient be referred to a specialized endometriosis clinic or center of excellence?
Finally, they were given two clinical questions. When asked about the management of a patient with a clinical suspicion of endometriosis, severe pain, a 5 cm ovarian cyst with opaque contents, who desires fertility there was no consensus among the responders (Figure 4). Less than 10% suggested attempting pregnancy either spontaneously or with ovulation induction. A fifth of the responders would have referred the patient to a specialized clinic (17.6%) or for laparoscopic surgery (3.3%). Yet, the vast majority would have continued follow-up and surveillance with repeated ultrasound examinations and measurement of serum CA-125 with or without continuous OCP. When presented with a case of a similar patient (suspected of having endometriosis, suffering severe pain and a 5 cm ovarian cyst with opaque contents) who does not desire fertility (Figure 5), as few as 15.9% of the responders would have referred the patient to a specialized clinic and another 11.0% would have referred the patient for laparoscopic surgery. Around three quarters of the doctors would have offered the patient different treatment modalities including continuous OCP, GnRH agonist therapy and ultrasound and CA-125 evaluation.
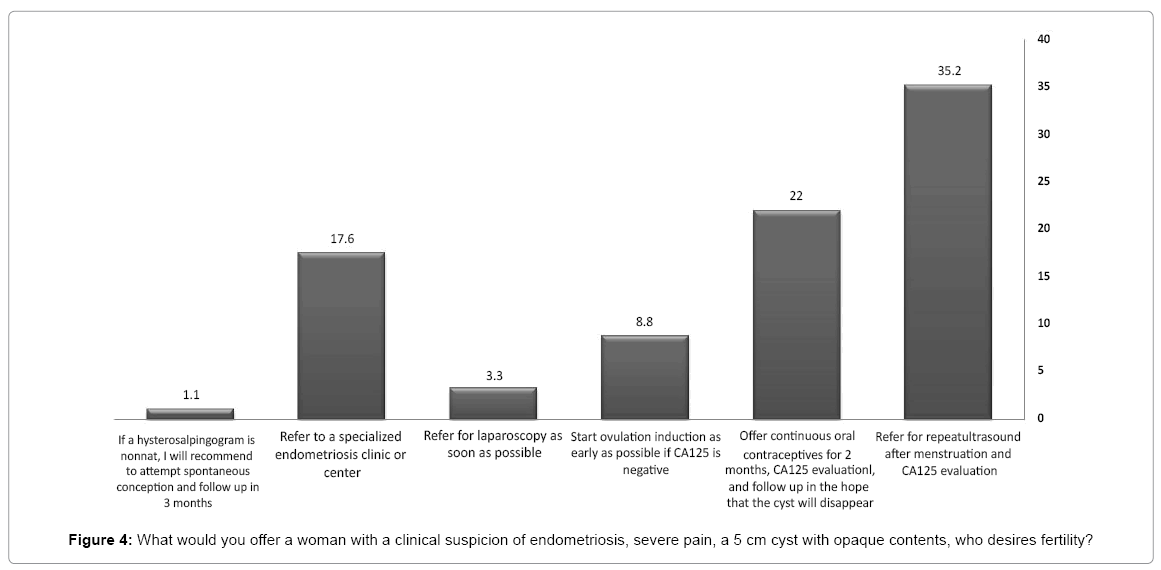
Figure 4: What would you offer a woman with a clinical suspicion of endometriosis, severe pain, a 5 cm cyst with opaque contents, who desires fertility?
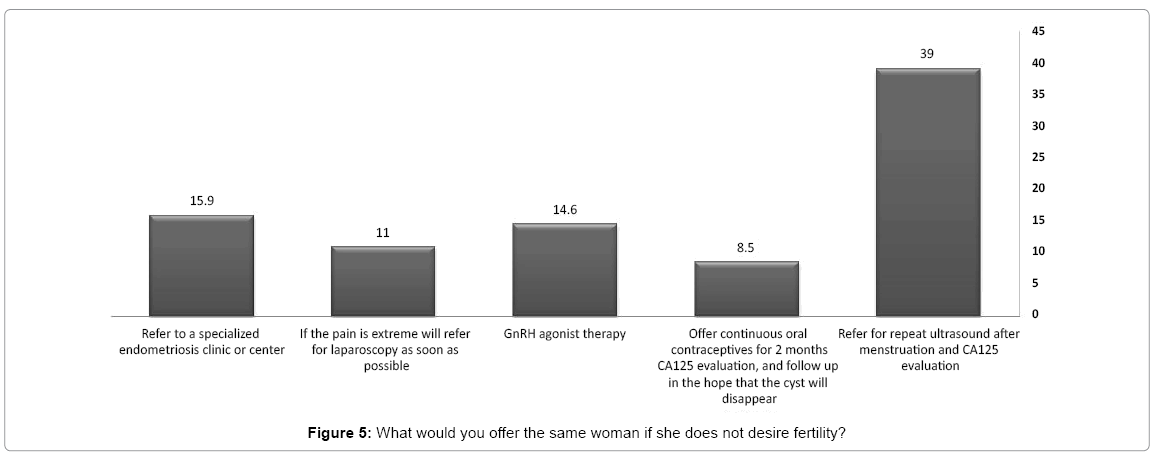
Figure 5: What would you offer the same woman if she does not desire fertility?
The purpose of the current study was to evaluate whether a diagnostic delay in endometriosis exists based on the decision making of gynecologists in a clinical setting regarding the management of endometriosis. The most notable finding in our study was that, although knowledge and awareness regarding dysmenorrhea and endometriosis have increased in recent years, there is still much inconsistency regarding the appropriate modality, timing and provision of adequate treatment.
Diagnostic delay is normally considered as the time interval between the appearance of symptoms and diagnostic surgery. Delay ranging from 7 to 12 years is well documented in endometriosis [10,13-15] and contributes to the impaired quality of life and significant personal and societal costs associated with the condition [10]. This seems consistent with the recent findings of Nnoaham et al., [10] showing a delay of 6.7 years in affected women, which was mainly due to delays in referral from the primary care physician to the gynecologist, with women reporting an average of seven visits before specialist referral. In our study, gynecologists in community practice seem to be largely unaware of the role of specialized care in the management of endometriosis.
Laparoscopic surgery under general anesthesia is most commonly required to reach a definitive diagnosis of endometriosis, but this is expensive and potentially associated with complications [23].
Numerous reasons have been advocated in an attempt to explain the diagnostic delay of endometriosis. Traditionally these could be divided into three groups:
1. Disease related factors, such as overlapping of endometriosis symptoms with other morbidities (i.e. urinary tract infection, interstitial cystitis, pelvic inflammatory disease and others), and the lack of good nonsurgical methods of diagnosing the disease or at least predicting its presence.
2. Patient related factors, including symptom endurance due to inaccurate perception of normal versus abnormal pain, embarrassment, and individual coping strategies.
3. Physician related factors, such as lack of awareness or knowledge, or simply lack of confidence in surgery results.
Although these traditional explanations for the delay in diagnosis may account for a large portion of the delays, we would like to point out some additional factors that may be even more substantial. These have to do with health care medical policy. There is a considerable void in clinical guidelines to direct clinicians regarding the appropriate investigation and appropriate modality, timing and provision of adequate treatment. These could be explained by several factors including:
1. A diversity in symptoms (cysts, pain, infertility or a combination of these) and in clinical settings (adolescence, chronic pain patients, patients desiring fertility, etc.), has led to lack of guidelines.
2. Many of the existing recommendations advocate delaying surgery resulting in a delay in diagnosis.
3. Due to a shortage in adequately powered randomized controlled trials that aim to answer some of the important clinical questions, good evidence-based recommendations cannot be made.
4. Some of the existing clinical recommendations are too general at best and contradicting and confusing at times (i.e. Does surgery for ovarian endometrioma improve fertility performance or impair ovarian reserve and which type of patient should it be recommended for?).
In our study there was general agreement between the responding physicians regarding knowledge of the disease. Thus, lack of awareness is less likely to be the explanation for the tendency to delay referral of patients with suspected endometriosis to targeted investigation and appropriate treatment. Furthermore, women were not likely to be referred to specialized centers of care, unless they endured severe symptoms of the disease (i.e. suffered from large pelvic masses and a significant increase in CA125 levels, repeated IVF failure and refractory pain after repeated surgery, or significant involvement of other organs, such as intestines and urinary bladder). This suggests that women could suffer for an extended period of time, even after being diagnosed with probable endometriosis, sometimes even after surgical diagnosis by diagnostic laparoscopy, and still adequate therapy would not be administered.
Another reason that can explain the delay in diagnosis is refraining from surgery. Surgery is hardly ever the initial treatment of choice in most clinical settings. Indeed, in our study when the physicians were asked about the first line therapy for a 24 year old single woman with severe debilitating dysmenorrhea who does not desire fertility, responders unanimously agreed (almost 95% of responders) that OCP were the treatment of choice.
When asked about the best second line treatment for the same patient, responses were variable and inconsistent. This emphasizes much of the confusion around the appropriate modality, timing and provision of adequate treatment. Hence, not only is surgery not considered the first line of therapy for patients with endometriosis but its role as a second line therapy is questionable as perceived by the responding physicians in our study. This fact further contributes to the delay in reaching a definitive diagnosis, and individualized treatment and care.
Our results raise a very troubling issue, namely that many doctors believe that early diagnosis is of no benefit because there is no good treatment. Hence, not the lack of knowledge and awareness of the disease, but rather lack of uniform guidelines for the adequate management and treatment of these patients may be the cause of the delay in referral to specialized centers. We believe that there is room for significant education of our caregivers in order to achieve a change of practice aimed at channeling affected patients to receive early specialized care rather than to be continuously followed in a primary care setting. It may no longer be the delay until diagnosis that worries us, but rather delay in offering adequate therapy, even after proper diagnosis has been made.
From the patients’ point of view, intermittent hormonal alleviation of symptoms, the most common first line therapy, may cause the patients to refrain from returning to their primary caregiver for a significant length of time. After this time patients may return to the primary caregiver due to fertility concerns, possible side effects of hormonal treatments, or worsening and intractable pain. In our study, even though the primary care physician was in fact a gynecologist, there was still a delay to be expected before referral to a specialized endometriosis clinic or center.
In a recent large international study, Nnoaham et al. [24] attempted to generate and validate a symptom-based model to predict endometriosis among symptomatic patients prior to undergoing their first laparoscopy. They found that their model poorly predicted anystage of endometriosis but predicted stage III and IV quite well [24].
Persistent pelvic pain usually leads to referral for ultrasound investigation in order to exclude pelvic pathology. While, transvaginal ultrasound, performed in a primary care setting has a high specificity and sensitivity for endometriomas [25], it used to be a poor measure for non-ovarian pelvic endometriosis (uterosacral ligaments, vagina, and rectovaginal septum [26]), and is not a good discriminator of pelvic pain pathology [27]. A normal ultrasound in a primary care setting seems to falsely reassure the caregiver that further investigation or treatment is unnecessary, and that endometriosis had been ruled out, raising questions about the continuing use of transvaginal ultrasound to exclude non-ovarian endometriosis. More recent studies suggest that transvaginal ultrasound should be the first line examination in the diagnosis of non-ovarian endometriosis, with a sensitivity and specificity of 78-98% and 90-100%, respectively, which still raises the issue of a large number of false negatives. Most studies state that transvaginal ultrasound should be performed in the setting of a specialized center and by an experienced operator [28-30], since clinical and sonographic-based models for diagnosis of endometriosis are limited, in many countries laparoscopy is performed as a diagnostic procedure. This is not so in Israel where the surgical practice routine is ‘see and treat’. Since surgical treatment is still controversial in many clinical settings especially in the context of infertility, many physicians are reluctant to refer their patients to specialized centers for surgery. This may be another contributor to the delay in definitive diagnosis and treatment.
Another interesting aspect is the notion that delays in diagnosis are frequently a result of the absence of a non-invasive valid simple diagnostic blood test. In our study, almost two thirds of responders believed that indeed there was a diagnostic delay as a result of this. In contrast to our findings, the responders attributed this mainly to low awareness but also to the absence of a valid simple non-invasive diagnostic test. There is a continual search for such a test, which will ultimately replace our dependence on the non-specific CA-125, and would help avoid unnecessary diagnostic laparoscopies [23,31]. Furthermore, such a test can be used in the presence of a normal diagnostic ultrasound [32-35]. However, a diagnostic biochemical panel as suggested by Vodolazkaia et al. [34], may do more harm than good, by subjecting patients to unnecessary or even potentially harmful procedures, since the benefits of treating women with asymptomatic endometriosis is unclear. On the other hand, a blood test could identify those most likely to have endometriosis or other pelvic conditions and likely to benefit from surgical therapy for both sub-fertility and pain. The question remains whether such a test will be the best answer in all clinical situations? will it in fact change primary care practice?, and can it inadvertently turn into a “non-formal” screening test? [36].
As mentioned earlier, in our clinical setting the primary care gynecologist is often the first to see the patient with a clinical suspicion of endometriosis, rather than the general practitioner. This means at least in theory that part of the diagnostic delay period could be shortened. For this purpose our experience may not be applicable to other countries, which may be a drawback of our study. But our findings suggest that this is probably not the case, because there is apparently a delay caused by many gynecologists who still advocate inadequate or insufficient care.
We have vastly discussed numerous reasons for the diagnostic delay in endometriosis. Based on our findings, it seems that it is not a delay in the diagnosis that adversely affects the management of endometriosis, but rather a lack in uniform management guidelines and a delayed referral to targeted specialized centers. However, recently the World Endometriosis Society (WES) has published a global consensus on the management of endometriosis [37]. Among many other issues that are discussed in the consensus statement, Johnson et al. [37] discussed empirical medical treatment for symptoms of endometriosis. They state that many clinicians support empirical medical treatment of endometriosis either prior to or without laparoscopic confirmation of endometriosis. Advocators of empirical medical treatment state that time to surgery may delay appropriate treatment, there is a false negative rate in laparoscopic diagnosis, surgery is invasive and expensive compared with empirical therapies, and it carries a risk of morbidity [37].
Depending on the severity of symptoms, patient’s age and fertility desires, in many cases delaying surgery is considered and even recommended. Delaying time to surgery, by definition, causes delaying time to diagnosis. However, it is not synonymous with delaying appropriate treatment. This was strengthened in the recent consensus statement previously discussed [37].
In conclusion, physicians in community practice are still largely unaware of the role of specialized care in the optimal management of endometriosis. The focus on the delayed diagnosis of endometriosis should be abandoned, and attention should be directed to the administration of appropriate treatment even in the absence of surgical and histological diagnosis. It is important to dedicate efforts and resources to research and perform randomized clinical trials that will aid in establishing significant evidence based guidelines for the management of endometriosis.