Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Review Article - (2015) Volume 3, Issue 3
Objective: To evaluate live birth rates and the influence of pregnancy on the prognoses of young women (<40 years old) with early-stage endometrial cancer (EC) and atypical complex hyperplasia (AH) who were treated by conservative management followed by assisted reproductive technology (ART).
Methods: A meta-analysis of observational studies with a random-or fixed-effects model as appropriate.
Results: A study of 527 women from 23 studies included 201 women to assess how prognosis might be influenced by pregnancy. Analysis of no pregnancy studies as the reference group pointed to a statistically significant positive association between pregnancy and decreased risk for recurrence (RR) of 0.56, 95% confidence interval (CI): 0.37-0.84. Eighteen studies including 104 women enabled determination of live birth rates of women with earlystage EC (79 women) and AH (25 women) following treatment with conservative management followed by ART. For patients with AH, 25 women were treated with ART after pathological remission of disease. Thirteen women achieved intrauterine pregnancies, and nine had 10 live births, with a pooled live birth rate of 0.32 with insignificant heterogeneity (P = 0.925). For those with EC, 79 women were treated by ART, 61 by IVF-ET, 12 by IUI, and 6 by ICSI. Fifty-seven women had intrauterine pregnancies, and 45 had 52 live births, with a pooled live birth rate of 0.60 and insignificant heterogeneity (P = 0.923).
Conclusions: Live birth rates were encouraging using ART in young women with EC or AH who desired fertility after conservative management. Resulting pregnancies could reduce recurrent risk of AH and EC. Additionally, minimizing the time interval between treatment termination and pregnancy was important.
<Keywords: Fertility-sparing treatment; Endometrial cancer; Endometrial atypical hyperplasia; Live births; ART; Systematic review
Endometrial cancer is the most common gynecological malignancy in women, with more than 280,000 cases occurring annually worldwide [1]. Endometrial carcinoma (EC) and atypical hyperplasia (AH) classically affect postmenopausal women. However, a total of 5% of endometrial carcinoma is diagnosed under the age of 40 years, and over 70% of patients are nulliparous at diagnosis [2,3]. An even larger proportion of premenopausal women are diagnosed with complex atypical hyperplasia, a known precursor of endometrial carcinoma [4].
Early stage EC and AH also affect premenopausal women, particularly those with risk factors such as infertility, obesity, and polycystic ovarian syndrome. This situation becomes more common with increasing rates of obesity and delayed childbearing. These women are usually diagnosed with early clinical stage and well-differentiated EC with a good prognosis [5]. Commonly, the standard treatment for endometrial carcinoma is a total extrafascial hysterectomy, bilateral salpingo-oophorectomy (BSO), and pelvic and para-aortic lymph node assessment [6]. The dissection approach is unacceptable for these women who wish to maintain their fertility.
Conservative treatment based on progestins can induce endometrial regression and prevent the progression of the disease. Oral progestogens and the levonorgestrel-releasing intrauterine system are used to treat EC and AH. A systematic review and meta-analysis pooled the studies and literature reviews, indicating that the 12- and 24-month remission probabilities were 78.0% and 81.4%, respectively [7]. Therefore, the available data proposed the relative safety and efficacy of conservative treatment for an opportunity to allow the patients to achieve their reproductive goals.
Research has suggested that hormone therapy followed by assisted reproductive technology (ART) was a good option in carefully selected women with early-stage endometrial carcinoma [8]. However, the treatment of controlled ovarian stimulation or ovulation induction for infertility can lead to hyperestrogenic status, which might be involved in disease recurrence or progression. Nevertheless, in 2013, Ichinose et al. [9] published a review of 36 women with EC/AH who achieved complete response after high-dose medroxyprogesterone acetate followed by infertility treatment including ART, showing that the use of ovulation-inducing drugs after the conservative treatment of endometrial cancer did not increase disease recurrence.
Although several previous studies [9-11] showed that women who achieved pregnancy had a significantly lower risk of recurrence than those without pregnancy, they were limited by a small number of subjects and a lack of relative risk (RR), as evaluated by the recurrence of EC and AH in non-pregnant women as the reference group. Therefore, the objective of this study was to evaluate the live birth rates and influence of pregnancy on the prognoses of young women with earlystage EC or AH who were treated by conservative treatment followed by ART, thus to provide better data for the success of using ART in these patients who desire fertility after fertility-sparing management.
This systematic review was conducted in accordance with the PRISMA guidelines [12] and was also in accordance with the a priori protocol agreed upon by all authors.
Identification of literature
The population of interest in this systematic review included women with AH or early clinical stage EC (1988 International Federation of Gynecology and Obstetrics stage IA). The intervention queried was conservative treatment, and the outcomes were evidence of live births or recurrence. The following electronic databases were searched: PubMed (1950 to 2014) and Web of Science conference proceedings (ISI Proceedings, 1990 to 2014).
A combination of medical subject headings (MeSH) and text words were used to generate 3 subsets of citations including the following: [1] studies on EC (“endometr* cancer*,” “malignant endometr*”) or endometrial hyperplasia (“endometr* hyperplas*,” “premalignant endometr*,” “precancer* endometr*”); [2] studies on fertility-sparing therapies such as progestogens and intrauterine devices or systems (“intrauterine devices medicated,” “Levonorgestrel,” “Mirena,” “intrauterine progest*,” “LNG-IU*,” “progest*,” “gestag*,” “fertilitysparing therapy,” “conservative therapy,” “hormone*therapy”); and [3] studies on pregnancy (“reproduct*,” “fertiliza*,” “gravid*,” “pregnan*”). [1] and [2] were combined with the word “and” to get [4], and [1] and [3] were combined with the word “and” to get [5]. Then, [4] and [5] were combined with the word “or” and limited to the words “humans and female” to generate a subset of citations. The reference lists of all known primary and review articles were examined to identify cited articles that were not captured by electronic searches. Language or geographical restrictions were not applied during the search or selection.
Study selection and data extraction
Inclusion and exclusion criteria for the selection of articles were developed. Inclusion criteria were studies including women diagnosed histologically with AH or stage I adenocarcinoma of the endometrium, the intervention of fertility-sparing therapy, and the outcomes of live births or recurrence. Exclusion criteria included the following: case reports and small study series with fewer than five women; women with tumors invading the myometrium; conservation due to high risk of perioperative morbidity; data not extractable; unknown mode of conception; other uterine neoplasia than endometrioid adenocarcinoma; and women with simple hyperplasia.
Studies were selected in a 3-stage process. First, the reduplicated records were removed. Second, 2 reviewers scrutinized the titles and abstracts from the electronic searches independently (H.C. and S.Y.Z.), and full manuscripts of all citations that met the predefined selection criteria were obtained. Third, final inclusion or exclusion decisions were made upon the examination of the full manuscripts. Any disagreements about inclusion were resolved by consensus or arbitration by a third reviewer (Y.L.). Each of the 23 articles were read by two different readers (S.Y.Z. and L.P.Y.), and a database was created with the following two types of items: [1] the pregnancy outcomes of different modes of conception in fertility-sparing management of AH and EC, and [2] the influence of pregnancy on the prognosis of EC/AH.
Databases from these studies were saved separately on a Microsoft Excel 2010 file for each article. A line was created for each study detailing the live birth rates of different modes of conception and the influence of pregnancy on the recurrence of EC/AH. The studies selected to assess the live birth rates and influence of pregnancy on EC/AH recurrences are shown in Table 1.
| First author, year [reference] |
Participants | Design | Study size | Investigations prior to treatment to rule out invasion |
Intervention | Outcomes studied | Follow-up | |
|---|---|---|---|---|---|---|---|---|
| Imaging | Tumor markers | |||||||
| Elizur, 2007 [41] |
EC, referred to ART after conservative treatment | Unclear | 8 EC Ia G1 | MRI and hysteroscopy | CA125 | MPA=2 MA=6 | Pregnancy outcomes | NA |
| Fujiwara, 2009 [42] | EC/AH detected on infertility studies | Retrospective | 6(3 AH, 3 EC Ia G1) | TVS | No | MPA=6 | Pregnancy outcomes | NA |
| Hahn, 2009 [24] | EC women treated with fertility-preserving management | Retrospective | 35(31 EC Ia G1, 4 EC Ia G1 or G2 | MRI, CT, and TVS | No | MPA=20 MA=8 Both=7 |
Pregnancy outcomes | Mean follow-up of 39 mo |
| Han, 2009 [23] | EC/AH, age 40 or younger, desire to preserve fertility, treated with conservative management followed by ART |
Retrospective | 10 (of the 11 women, 1 patient did not undergo ART and was excluded): 5 EC Ia G1 or 2 G2, 3 AEH |
MRI and USD | CA125 | MPA=3 MA=7 | Pregnancy outcomes |
Mean follow-up of 21 mo |
| Ichinose, 2013 [9] | EC/AH achieved complete response after high-dose MPA |
Retrospective | 36(13 AEH, 23 EC Ia G1) | MRI and USD | No | MPA=32 | Pregnancy outcomes, recurrence |
Mean follow-up of 91.4 mo |
| Jadoul and Donnez, 2003 [14] | EC/AH, age between 27 and 38 years, treated with conservative management | Retrospective | 7 (2 complex AH, 5 EC Ia G1) | hysteroscopy | No | GnRH agonists=7 | Pregnancy outcomes |
Mean follow-up of 28 mo |
| Jafari, 2013 [25] | EC, younger than 35 years, nulliparous, strong desire to preserve fertility | Prospective | 8 EC Ia G1 | MRI and TVS and CT | CA125 and CEA | MA=8 | Pregnancy outcomes |
Mean follow-up of 34.5 mo |
| Koskas, 2012 [20] | EC/AH treated with conservative management | Retrospective | 22(14 AEH, 8 EC Ia G1) | MRI | No | MPA=4 MA=5 NMA=7 CA=3 Lynestrenol=3 |
Pregnancy outcomes |
NA |
| Kudes Ia, 2014 [43] | EC/AH, younger than 45 years, treated with fertility-sparing management | Retrospective | 23(13 AEH, 10 EC Ia G1) | MRI | No | Oral progesterone only=9 LNG-IUD only=6 Both oral and LNG-IUD =8 | Pregnancy outcomes |
Mean follow-up of 13 mo |
| Mao, 2010 [26] | EC treated with fertility-sparing management with the use of progesterone | Retrospective | 6 EC Ia G1 | MRI and TVS and CT | CA125 | MPA=4 MA=2 | Pregnancy outcomes |
NA |
| Minaguchi, 2007 [13] | EC/AH, desire to preserve fertility, included one patient of age over 40 (60 years old) who had to receive conservative therapy due to complications |
Unclear | 31(12 complex AEH, 19 EC Ia G1) |
MRI and TVS and CT | No | MPA=31 | Pregnancy outcomes |
Mean follow-up of 40.7 mo |
| Minig, 2011 [21] | EC/AH, age between 20 and 40 years, desire to preserve fertility | Prospective | 34(20 AEH, 14 EC Ia G1) | MRI and TVS and hysteroscopy | No | LNG-IUD for 1 year and GnRH analogue for 6 months=34 | Pregnancy outcomes |
Mean follow-up of 29 mo |
| Niwa, 2005 [28] | EC, age 40 or younger, nulliparous, strong desire to preserve fertility |
Prospective | 12 EC Ia G1 | MRI and TVS | CA125 | MPA=12 | Pregnancy outcomes |
Mean follow-up of 59 mo |
| Park, 2012 [29] | EC, age younger than 40 years, strong desire preserve fertility |
Retrospective | 14 EC Ia G1 | MRI and TVS and hysteroscopy | No | MPA=12 MA=2 | Pregnancy outcomes |
NA |
| Park, 2013 [10] | younger than 40 years | Retrospective | 141 EC Ia G1 | MRI and TVS and CT | CA125 | MPA=85 MA=56 | Recurrence | Mean follow-up of 66 mo |
| Parlakgumus, 2014 [8] | EC, strong desire preserve fertility | Retrospective | 5(3 EC Ia G1, 2 EC Ia G2) |
MRI and USD | CA125 | MA=4 Dydrogesterone=1 | Pregnancy outcomes |
NA |
| Perri, 2011 [11] | EC, had been treated conservatively to preserve fertility | Retrospective | 27 EC Ia G1 | MRI and TVS | No | MPA=3 MA=21 norethisterone acetate =1 hydroxyprogesterone caproate=2 | Pregnancy outcomes, recurrence |
Mean follow-up of 57.4 mo |
| Ushijima, 2007 [22] | EC/AH, age between 20 and 39 years | Retrospective | 45(17 AEH, 28 EC Ia G1) | MRI and hysteroscopy | No | MPA=45 | Pregnancy outcomes |
Mean follow-up of 47.9 mo |
| Wang, 2002 [27] | EC, younger than 40 years, nulliparous, desire to preserve fertility |
Retrospective | 9 EC Ia G1 | MRI and TVS | CA125 | MA+tamoxifen=8 MA=1 | Pregnancy outcomes |
Mean follow-up of 66 mo |
| Yahata, 2006 [44] | EC, treated with MPA for over 6 months because of treatment failure or relapse | Retrospective | 8 EC Ia G1 | MRI and TVS | No | MPA=8 | Pregnancy outcomes |
Mean follow-up of 76.5 mo |
| Yamazawa, 2007 [45] | EC, age younger than 40 years, nulliparous, strong desire to preserve fertility | Prospective | 9 EC Ia G1 | MRI and TVS and CT | CA125 | MPA=9 | Pregnancy outcomes |
NA |
| Yang, 2005 [30] | EC, desired to preserve fertility |
Prospective | 6 EC Ia G1 | MRI and USD and CT | CA125 | Megace=6 | Pregnancy outcomes |
Mean follow-up of 44.8 mo |
| Yu, 2006 [15] | EC/AH, younger than 35 year, treated with progestin | Retrospective | 25(17 severe AH, 8 EC Ia G1) |
MRI and USD | CA125 | MPA=22 MA=3 | Pregnancy outcomes |
NA |
Note: AH=atypical hyperplasia; EC=endometrial cancer; G=grade; CT=computed tomography; MRI=magnetic resonance imaging; USD=ultrasound; TVS=transvaginal ultrasonography; GnRH=gonadotropin releasing hormone; LNG-IUD=levonorgestrel-releasing IUD; IUD=intrauterine device; MA=megestrol acetate; MPA=medroxyprogesterone acetate; NMA=nomegestrol acetate; CA=chlormadinone acetate; NA= not available; mo=month
Table 1: Characteristics of studies included in the meta-analysis investigating pregnancy outcomes and/or influence of pregnancy on the recurrence of AH and EC after fertility-sparing management.
Concerning histology, most studies did not distinguish the various subtypes of AH (complex or simple), only making the distinction between EC and AH. Atypical hyperplasia was not divided into simple and complex AH. In none of the studies did the authors report cases of simple AH managed conservatively. In two studies [13,14], the authors specified that all AH cases managed were complex, and in one study [15], the authors reported that the AH cases managed were “severe”. In all the other studies, the degree of AH was not reported. Treatments were classified into three categories: MA, MPA, and other hormone therapies. Other hormone therapies included GnRH agonists, lynestrenol, oral contraceptives, levonorgestrel-releasing IUD, dydrogesterone, norethisterone acetate, hydroxyprogesterone caproate, tamoxifen, and megace.
Recurrence was defined as the reappearance of AH or cancerous cells that had initially disappeared. Different modes of conception were defined as spontaneous conception, ovulation induction, and ART including IUI (intrauterine insemination), IVF-ET (in vitro fertilization and embryo transfer), and ICSI (intracytoplasmic sperm injection). In the present study, the pregnancy rate was defined as the percentage of women who succeeded in achieving pregnancy among patients who had been attempting to conceive. Live birth was defined as the birth of a healthy infant during the follow-up period, and its rate was calculated as the percentage of women who delivered live infants among those who had been attempting to conceive.
Statistics and data analysis
Three studies were identified, and the pooled effect estimates for relative risk (RR) were calculated by recurrence probabilities between pregnancy and non-pregnancy. The meta-analysis was performed using the STATA metan command. Fixed- (Mantel-Haenszel) or randomeffects (DerSimonian-Laird) models were used to calculate the pooled effect estimates. Between-study heterogeneity was assessed by chisquared test (significance level at P < 0.1) and by estimating I2. In cases of significant heterogeneity, irrespective of the I2 estimation, randomeffects models were employed to allow for it.
Live birth rates were extracted from eighteen studies, and the log of the ratio and its corresponding standard error were computed for each study. The meta-analysis was performed using inverse-variance weighting to calculate the random-effects summary estimates [16]. An estimate of the between-study variance with a random-effects metaanalysis was obtained. The square root of this number was the estimated SD of the underlying effects across studies. Upon gaining the relative measures of effects, the confidence intervals were centered on the natural logarithm of the pooled estimate and the limits exponentiated to obtain an interval on the ratio scale [17]. Forest plots were created for each live birth rate, showing individual study proportions with confidence intervals (CIs) and the overall DerSimmonian-Laird pooled estimate [18]. Heterogeneity of the treatment effects was assessed graphically with forest plots and statistically analyzed using the chisquared test [19]. Statistical analyses were performed using Stata 12.0.
Selection and characteristics of the primary studies
The electronic search strategy yielded 3321 citations, and another 4 citations were achieved by manually checking the reference lists of all primary articles. Of the 3180 total studies that were initially identified, 3129 were excluded after review of the title or abstract. A total of 51 articles reporting medical treatment for AH or EC were therefore included for a thorough review. After detailed review, 23 studies reporting the conservative management of AH and EC in young women wishing to preserve their fertility were eligible for use in the meta-analysis, including 527 women, of which 413 were, diagnosed with EC and 114 with AH (Figure 1). The main characteristics of the 23 studies are presented in Table 1.
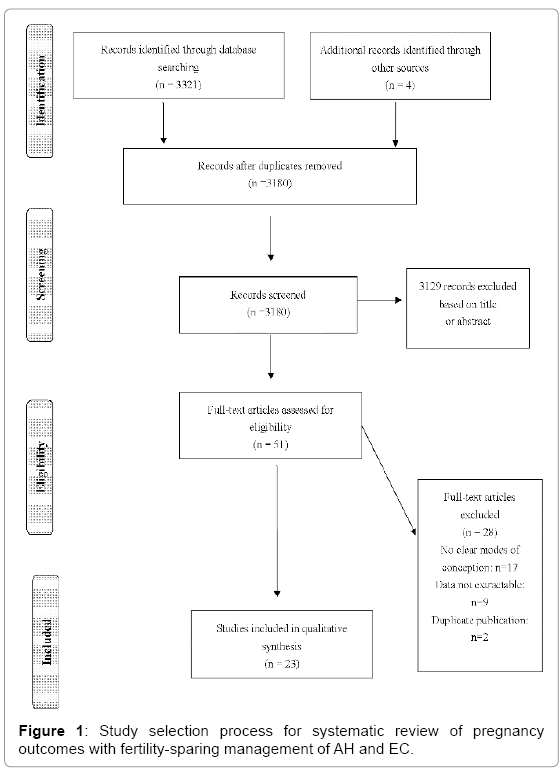
Figure 1: Study selection process for systematic review of pregnancy outcomes with fertility-sparing management of AH and EC.
Five studies were prospective, and 16 were retrospective; the distinction was not clear for 2 studies. The primary studies included women with well-differentiated EC, with 405 women classified as G1 and 8 women with moderate or poor differentiation (G2 or G3). In all studies, the women enrolled underwent diagnostic imaging to rule out myometrial invasion or distant disease. In 11 studies, the serum CA-125 marker was measured to also rule out concurrent ovarian malignancy.
Influence of pregnancy on the recurrence of EC/AH
Three studies with a total of 201 women; including 188 and 13 women with EC and AH, respectively, were used to investigate the relationship between a resulting pregnancy and disease recurrence. From the 81 women who achieved pregnancy, 23 experienced recurrence, and 55 of the 120 women who did not achieve pregnancy experienced recurrence. The synthesis of studies with non-pregnancy as the reference group pointed to a statistically significant positive association between pregnancy and a reduction in the risk of recurrence of AH and EC (pooled effect estimate = 0.56, 95% CI: 0.37-0.84, fixed effects, Figure 2). The P value for the chi-squared test for heterogeneity was 0.176, and I2 = 42.4%, indicating an insignificant variability in the RR among the studies. Pregnancy can reduce the risk of recurrence of AH and EC of 0.44.
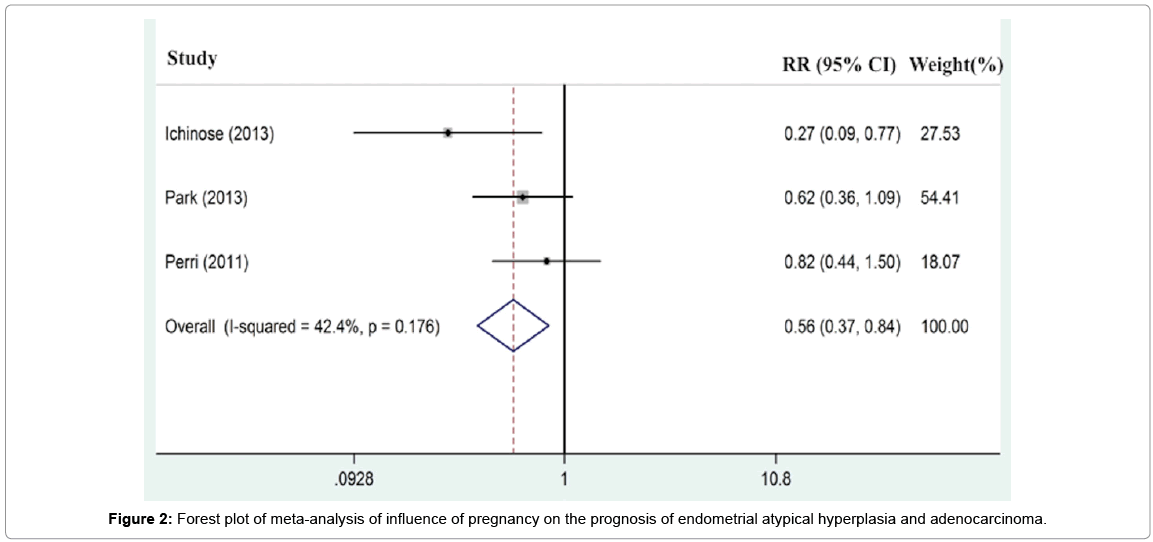
Figure 2: Forest plot of meta-analysis of influence of pregnancy on the prognosis of endometrial atypical hyperplasia and adenocarcinoma.
Live birth rate after fertility-sparing treatment therapy for AH
For AH, eight studies with a total of 45 women were used to assess pregnancy outcomes. Of the 45 women, 10 had achieved 11 spontaneous pregnancies, and 9 normal infants were delivered after pathological remission of the disease (Koskas et al. [20], Minig et al. [21], Ushijima et al. [22]); 10 had achieved 11 pregnancies, and 6 normal infants were delivered after ovulation induction therapy (Minaguchi et al. [13], Yu et al. [15], Han et al. [23], Minig et al. [21], Ushijima et al. [22]); and 25 women had achieved 13 intrauterine pregnancies, and 10 normal infants were delivered after ART therapy. The pooled live birth rate was 0.32 (95% CI: 0.14-0.51) with insignificant heterogeneity (P = 0.925, Figure 3), including 22 by in vitro fertilization and embryo transfer (IVF-ET), 2 by intrauterine insemination (IUI), and 1 by intracytoplasmic sperm injection (ICSI).
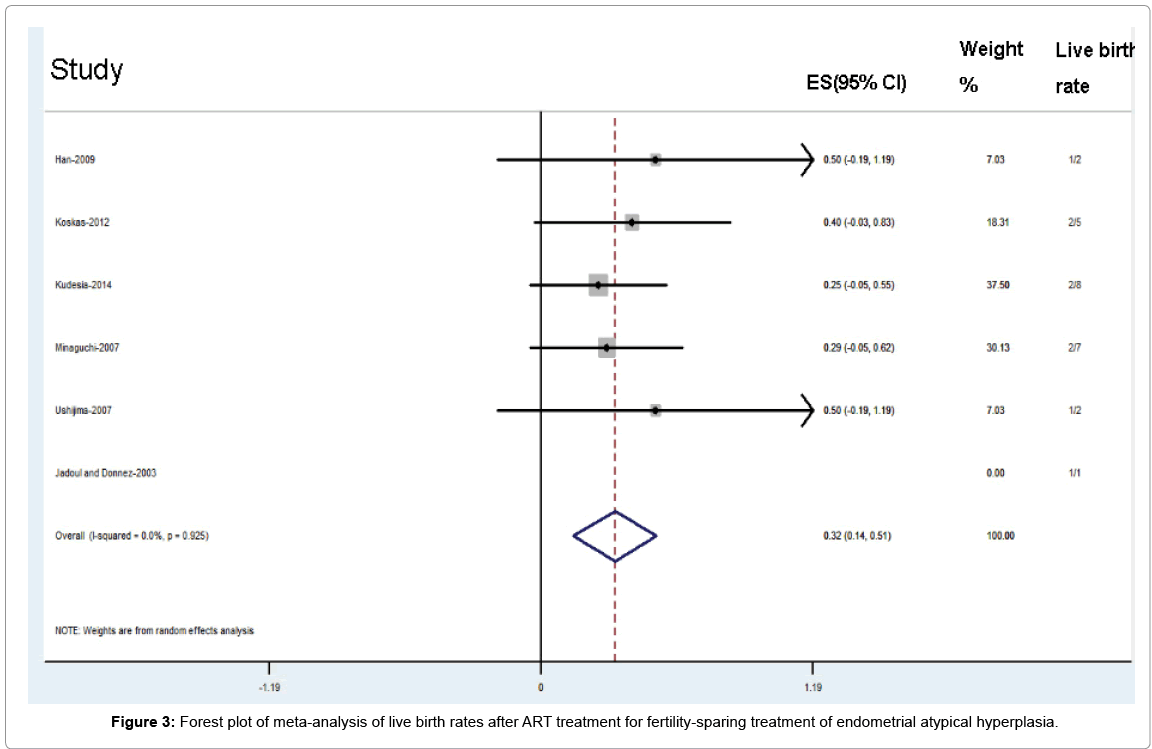
Figure 3: Forest plot of meta-analysis of live birth rates after ART treatment for fertility-sparing treatment of endometrial atypical hyperplasia.
Live birth rate after fertility-sparing treatment therapy for EC
For EC, 20 studies with a total of 111 women were used to assess pregnancy outcomes. Of the 111 women, 17 women had achieved 24 spontaneous pregnancies, and 16 normal infants were delivered, after pathological remission of the disease (Perri et al. [11], Jadoul et al. [14], Hahn et al. [24], Jafari et al. [25], Koskas et al. [20], Mao et al. [26], Minig et al. [21], Ushijima et al. [22], Wang et al. [27]); 15 women had achieved 10 pregnancies, and 9 normal infants were delivered after ovulation induction therapy (Minaguchi et al. [13], Han et al. [23], Koskas et al. [20], Niwa et al. [28], Park et al. [29]); and 79 women had achieved 57 intrauterine pregnancies, and 52 normal infants were delivered after ART therapy. The pooled live birth rate was 0.60 (95% CI: 0.49-0.71) with insignificant heterogeneity (P = 0.923, Figure 4), including 61 by IVF-ET, 12 by IUI, and 6 by ICSI.
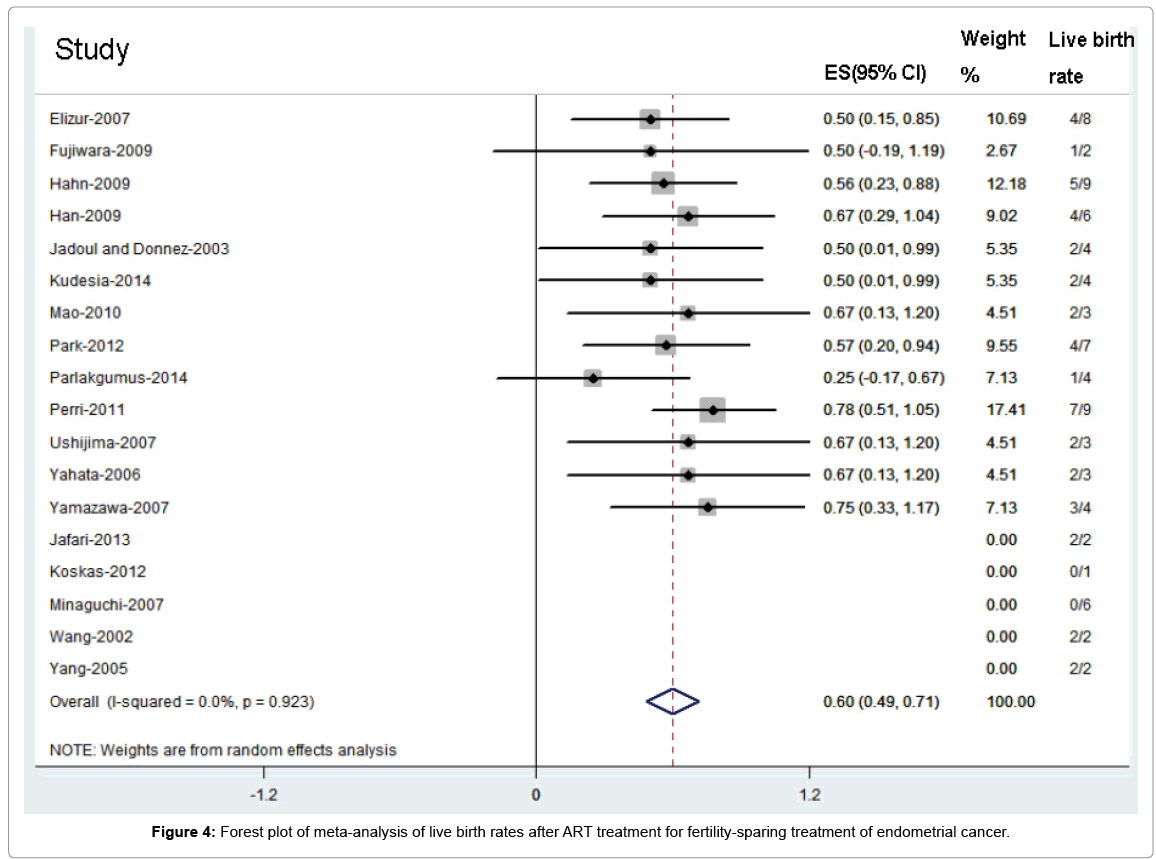
Figure 4: Forest plot of meta-analysis of live birth rates after ART treatment for fertility-sparing treatment of endometrial cancer.
Endometrial cancer and AH are rarely encountered in young women. This meta-analysis, which included 413 women with EC and 114 with AH, investigated two major dimensions of the conservative, fertility-sparing management of EC and AH. First, it was found that pregnancy could reduce the risk of recurrence of AH and EC of 0.44, which is very promising. Second, the meta-analysis identified that the live birth rates were very promising using assisted reproductive technology in young women with EC or AH who desire fertility after conservative management (60% of women with EC and 32% of women with AH).
Use of the meta-analysis was aimed to overcome the lack of literature on fertility-sparing management for women with AH and EC. Other systematic reviews produced a mean of the observed rates, which did not account for the specific weights of the studies and their variability [30]. The use of a random-effects model to combine the data across studies helped control for differences between the studies. Considering the studies included in this meta-analysis were all observational studies, there is an added layer of potential bias that is introduced. However, for a better interpretation of the results, several limitations must be discussed.
First, the present meta-analysis aimed to evaluate the impact of pregnancy on recurrence. The ratio of AH and the duration it took to achieve a complete response between the pregnancy group and nonpregnancy group were not calculated, both of which could be related to early disease recurrence. Therefore, the strength of the findings in this review including 3 studies is limited by the dearth of primary literature [31]. Second, the vast majority of the studies only reported women who had achieved pregnancies naturally, without including the amount of women who tried to be pregnant once remission was obtained. Consequently, the pregnancy and live birth rates were significantly higher than the actual in women who attempted natural pregnancies.
A meta-analysis determined that the 12- and 24-month remission probabilities were 78.0% and 81.4%, respectively. The 12- and 24-month recurrence probabilities were 9.6% and 29.2%, respectively. In the multivariate analysis, which included age, gravidity, previous infertility, histology, and hormonal therapy, none of the factors studied were associated with higher recurrence probability [7]. Moreover, Ichinose et al. suggested that women who achieved live birth had a significantly lower risk of recurrence than those without live birth [9]. Meanwhile, Han et al. [23] supported the negative correlation between the number of full-term pregnancies and the incidence of endometrial cancer [32] and suggested that early pregnancy after remission had benefits. The present study determined that pregnancy could reduce the risk of recurrence of AH and EC of 0.44, consistent with previous reports. Since pregnancy reduced the risk of recurrence, it seems important to minimize the time interval between treatment termination and pregnancy.
A meta-analysis determined that the live birth rates, including those after infertility treatment and natural pregnancies, were 28% for women with EC and 26% for women with AH [5]. Park et al. [29] published a review of 70 women with EC showing that the pregnancy rates (86.4% compared with 50%; P = 0.001) and live birth rates (70.5% compared with 42.3%; P = 0.020) were significantly higher in women who received infertility treatment than in those who attempted natural pregnancies [10]. In a recent meta-analysis that calculated the live birth rate after fertility-sparing management, the live birth rate after ART (39.4%) was significantly higher than after spontaneous pregnancy (14.9%) (P = 0.001) [33]. Seventy-nine and 25 women with EC and AH, respectively, were used to assess the live birth rates after ART therapy. The results showed that the live birth rates after ART therapy were 60% of women with EC and 32% of women with AH. It indicated that the live birth rates were very promising after the use of ART.
The goal of conservative treatment in young patients with EC/ AH is fertility preservation and pregnancy. Ichinose et al. [9] showed that the use of ovulation-inducing drugs after conservative treatment of endometrial cancer did not increase the recurrence of the disease. Consequently, it was recommended that the patient undergo infertility treatment as soon as possible after achieving a complete response. For women with no history of infertility treatment, ovulation induction drugs and timed intercourse or intrauterine insemination was recommended. For those who did not conceive after conventional infertility treatment and who had a history of infertility treatment or other infertility factors, ART was recommended. Because young women with EC or AH commonly have coincident polycystic ovarian syndrome or chronic anovulation, the implementation of ART not only maximized their chances of a live birth, but also decreased the interval to conception. Pregnancy itself was certainly a highly effective treatment because the placenta was a high progestin source. Pregnancy can help avoid prolonged unopposed estrogen stimulation, which could cause women to relapse [34].
However, women with EC/AH might have undesirable endometrial responses to ART therapy because of their primary endometrial disease, the high-dose progestin treatment, and repeated endometrial curettage in the treatment and examination of the disease [35], which can cause mechanical damage to the normal endometrial cells [36]. Cui et al. [37] determined that an endometrial thickness between 8-14 mm predicted a better clinical outcome. Recently, several studies reported the efficacy of hysteroscopic resection combined with hormonal therapy for early stage EC [38,39]. Additionally, a meta-analysis study reported that hysteroscopic resection for early stage EC would not increase the risk of peritoneal dissemination [40]. This new method is a new alternative for women who want to adopt conservative treatment.
This review of observational studies found that pregnancy can reduce the risk of recurrence, and the live birth rates were very promising using assisted reproductive technology in young women with EC or AH who desired fertility after conservative management. Assisted reproductive technology is a feasible option to achieve immediate conception after achieving complete remission. The patients should be well-informed about the risks and limitations of conservative treatment, and a close and long-term follow-up is necessary until the uterus is preserved. We would like to recommend that these women undergo prophylactic hysterectomy with bilateral salpingo-oophorectomy once their family is complete because of the high rate of recurrence after fertility-sparing management. Our systematic approach included published literature that had only observational evidence, so prospective randomized trials in larger numbers of patients and with longer follow-up times are warranted to evaluate the effects of fertility-sparing treatments.
The authors thank Professor J. Guo for expert analytical advice. This study was supported by the National Natural Science Foundation Project (81471520), the State Scholarship Fund (2011911033), Beijing Natural Science Foundation Project (5122015), and Project Training High-Level Medical Technical Personnel in the Health System in Beijing (2014-3-075).