Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Protocol Article - (2015) Volume 5, Issue 6
Background: Respiratory infections are considered a potential risk of adverse events in children undergoing surgery. Rhinovirus is a common cause of respiratory infections and congenital heart disease is a risk factor for severe rhinovirus infection. However, we do not know what the impact of, clinical or subclinical, rhinovirus infections is on postoperative course following congenital heart surgery in children.
Based on our clinical experience, one case-controlled study, and a case reported in the literature, we hypothesize that paediatric patients with per-operative rhinovirus positive Polymerase Chain Reaction testing have a longer paediatric intensive care unit admission, compared to children who test negative.
Methods/Design: This is a prospective single-center observational study in the Leiden University Medical Center with approximately 250 children (<12 years) undergoing elective cardiac surgery, for congenital heart disease.
The parents/guardians of the children will be asked to fill out a questionnaire, to asses respiratory symptoms in the last weeks, before the operation of their child. In the operating theatre, a nasopharyngeal swab will be collected. Clinical data will be collected daily during paediatric intensive care admission and paediatric intensive care unit and hospital length of stay will be recorded. If children are still intubated at day 4, a second nasopharyngeal swab and residual blood will be collected. The samples will be tested for rhinovirus with polymerase chain reaction. Primary outcome is the paediatric intensive care unit length of stay in per-operative rhinovirus-positive compared to rhinovirus-negative patients.
Discussion: This is the first study to screen children for rhinovirus before undergoing cardiac surgery and to study the effects on paediatric intensive care unit length of stay. Furthermore, we aim to identify children at risk for prolonged paediatric intensive care admission after cardiac surgery.
Keywords: Rhinovirus; Cardiac surgery; Paediatric intensive care; Congenital heart disease; Respiratory infection
AE: Adverse Events; CAHAL: Center for Congenital Heart Disease Amsterdam Leiden; CONSORT: Consolidated Standards of Reporting Trials; CPAP: Continuous Positive Airway Pressure; CPB: Cardiopulmonary Bypass; CRP: C-Reactive Protein; Ct: Cycle Threshold; ECG: Electrocardiogram; ETT: Eendotracheal Tube Size; FiO2: Fraction of Inspired Oxygen; IC: Intensive Care; IQR: Interquartile Ranges; LMA: Laryngeal Mask Airway; LOS: Length of Stay; LUMC: Leiden University Medical Center; MRI: Magnetic Resonance Imaging; OR: Operation Room; PCR: Polymerase Chain Reaction; PEEP: Peak Inspiratory Pressure and Positive End Expiratory pressure; PICU: Paediatric Intensive Care Unit; RACHS-II: Risk Adjustment Congenital Heart Surgery Score; RISK: Rhinovirus Infection & Surgery in Kids; RNA: Ribonucleic Acid; RSV: Respiratory Syncytial Virus; RV: Rhinovirus; SD: Standard Deviations
Rhinovirus (RV), a ribonucleic acid (RNA) virus of the family Picornaviridae and genus Enterovirus is a major cause of upper respiratory tract infections. The clinical spectrum ranges from asymptomatic to severe, life-threatening-pneumonia [1].
Asymptomatic shedding of RV is very common, especially in children, and tends to be higher in the younger age groups. In a study in the Netherlands, the prevalence of rhinovirus amounted to 20% for children under 2 years of age without nasal symptoms. [2] Risk factors for severe rhinovirus infections (lower respiratory tract infections, infections needing hospitalisation) in children are prematurity, congenital heart disease, respiratory syncytial virus (RSV) co-infections and non-infectious respiratory disease [3].
Upper respiratory tract infections are considered to carry a potential risk of adverse events in children undergoing surgery. Surgery in children with symptomatic upper respiratory tract infection is commonly postponed, because of the increased risk of complications of anaesthesia in these patients [4]. Adverse events (AE) related to respiratory tract infections are: laryngo-bronchospasm, breath holding spells, atelectasis, arterial oxygen desaturation, bacterial pneumonia and unplanned hospital admission [5,6]. Age below 6 years and cardiac surgery are additional specific risk factors for postoperative complications. The risk of peri-operative adverse events is increased up to 6 weeks after upper respiratory tract infections [4]. Patients undergoing cardiac surgery might have an additional risk, because of the immune-modulatory effect of cardiopulmonary bypass [7-9]. Children with a clinically apparent upper respiratory tract infection at the time of cardiac surgery have higher incidences of respiratory complications, multiple complications, postoperative infections and significantly longer paediatric intensive care unit (PICU) admission [10]. Paediatric patients with postoperative symptomatic rhinovirus infection appear to have a more complicated and prolonged post-operative course compared to other patients undergoing cardiac surgery (unpublished Leiden University Medical Center (LUMC) data). Especially PICU length of stay and duration of mechanical ventilation seem to be longer in patients with a rhinovirus infection. Every year approximately 20 paediatric patients in the LUMC have a complicated post-operative course in combination with a rhinovirus infection (unpublished LUMC data). Little has been published about the impact of rhinovirus infections on the post-operative course after cardiac surgery in paediatric patients. Simsic et al. described a case of nine months old boy with rhinovirus infection and a complicated course after cardiac surgery. Based on this case the authors screen all their paediatric patients with single-ventricle congenital heart disease by polymerase chain reaction (PCR) for respiratory viruses. In case of a positive PCR result, they postpone the operation for 4-6 weeks [11]. Delgado-Corcoran et al. recently published a case-control study of 19 cases of infants who tested positive for rhinovirus after cardiac surgery compared to 56 matched controls, untested symptom free patients. In this study the rhinovirus positive patients had a significantly longer intubation time and a three times longer PICU length of stay [12].
Ideally, these complications may be prevented by screening patients for the presence of respiratory infections with a clinical assessment in combination with PCR on a nasopharyngeal swab prior to their elective surgery.
Based on these retrospective data, we designed a single center prospective observational cohort study to analyse the impact of per-operative rhinovirus infection on the post-operative course in children undergoing elective cardiac surgery, with PICU length of stay as primary outcome. The subsequent goal is to develop an algorithm to identify children with increased risk for prolonged respiratory support after cardiac surgery. We named it the RISK study: Rhinovirus Infection & cardiac Surgery in Kids.
Design
This is a prospective, single-center, observational cohort study of the effects of rhinovirus in children undergoing cardiac surgery in the LUMC.
The LUMC is an academic hospital in Leiden, the Netherlands, and a top referral center for congenital heart disease and congenital cardiac surgery with approximately 250 operations each year. Combined with the two university medical centers of Amsterdam it constitutes the center for congenital heart disease Amsterdam-Leiden, in Dutch CAHAL [13].
Current standard procedures regarding elective cardiac surgery include the following: The day before the planned operation patients are assessed by the cardiologist, cardiac surgeon and anaesthesiologist who decide if the surgery can go ahead or if it will have to be postponed because of possible clinically relevant (respiratory tract) infection.
After surgery, patients are admitted to the PICU, where ventilation and circulatory support are weaned depending on the type of operation, bypass times and clinical stability. If symptoms of respiratory tract infection become apparent during the postoperative PICU stay, patients are routinely tested for either bacterial infections (culture) and/or viral infections by PCR for respiratory viruses on nasal lavage at the discretion of the treating intensive care physician.
In this study we will test all children for rhinovirus who are <12 years of age with congenital heart disease undergoing elective cardiac surgery in the LUMC. The majority of the children will be 0-1 years old, since cardiac surgery is preferably performed at (very) young age.
The primary endpoint of this study is post-operative PICU length of stay in rhinovirus positive compared to rhinovirus negative patients.
Secondary endpoints are:
• Duration of ventilatory support
• Mechanical ventilation conditions (mean airway pressure, Fraction of inspired oxygen (FiO2))
• Antibiotic free days (alive at PICU discharge)
• Inotrope requirement
• Infection parameters
• Hospital length of stay (LOS)
• Secondary infections
Alternative predictors of the endpoints are viral load (strength of PCR value), duration of respiratory shedding, genotype of the different rhinoviruses and rhinovirus viremia.
Inclusion criteria
In order to be eligible to participate in this study, subjects must meet all of the following criteria:
• Children (<12 year) with a congenital heart disease undergoing elective cardiac surgery who were not admitted pre-operatively
• Written informed consent by parents or guardian
Exclusion criteria
A potential subject who meets any of the following criteria will be excluded from participation in this study:
• No informed consent from one of the parents (or the legal representative if applicable)
• Emergency surgery (postponing of surgery not an option)
• Children not admitted to the intensive care unit after cardiac surgery (negligible amount of children)
• Children who will certainly have a prolonged PICU length of stay regardless of a possible rhinovirus infection:
• Children undergoing a second elective cardiac operation during the same intensive care stay
• Children with duct-dependent physiology who remain prostaglandin-dependent after the heart operation. For example: hypoplastic left heart syndrome following pulmonary artery banding who will remain on prostaglandins until the next staged operation.
Sample size calculation
This study will include approximately 250 children. The sample size calculation is based on the expected percentage of rhinovirus positive children and the expected difference in duration of PICU admission, our primary end point.
The estimated prevalence of preoperative children with rhinovirus of 20% was based on a prospective birth cohort study in the Netherlands among healthy children followed until the age of 2 years. In that study, the prevalence of rhinovirus among children without nasal symptoms was 20% (range 14-28%) (and 40% among children with rhinitis/upper respiratory tract infection) [2].
The mean duration of PICU admission following cardiac surgery in our PICU is 3.6 days. The study of Delgado-Corcoran et al., demonstrated almost a tripling of intensive care (IC) length of stay in rhinovirus infected children after surgery for congenital heart disease (up to one year of age), 2,14 (IQR 2.00-3.22) versus 6,03 days (IQR 2.98-14.22, p<0.0001). Since the control patients in this study were not tested for rhinovirus and therefore could be (asymptomatic) rhinovirus positive, the difference within our study might turn out to be smaller [12]. Combining these published data with a clinically relevant difference of 1 day and more, we aim to distinguish a difference between the two groups of 2 days. We base our sample size calculation on the comparison of two independent exponential means (PICU LOS in both groups).
Given these data for a power of 80% ((β=0.20), tested with a significance level of 5% (α=0.05), we calculated n 49 (sample size rhinovirus positive group and n=196 (sample size rhinovirus negative group) (ratio 1:4).
Data collection
Study procedure: If a patient is eligible for the study, the parents/ guardians will receive the information folder and a questionnaire by mail (see additional file 1) (asking for signs and symptoms of current and/or recent respiratory infections) approximately one week prior to the date of operation.
On the day of admission (day 0) all parents of eligible children will be asked to participate in this study and fill out a written informed consent form.
At day 1, the operation day, in the operating theatre, a nasopharyngeal swab will be collected following anaesthetic induction and tested for rhinovirus. All clinicians will be blinded for the PCR results which will only be accessible for the investigator from the virology department.
Clinical and laboratory data will be collected from all patients until discharge from the PICU. Of the patients still on mechanical ventilation at day 4, an additional rhinovirus PCR will be tested on a nasopharyngeal swab and residual blood will be used to determine rhinovirus viremia in the nasopharyngeal rhinovirus positive patients.
Collection of clinical data
On admission (i.e., day 0)
Baseline and demographic characteristics will be collected, including:
• Age, gender, cardiac diagnosis and medical history, including vaccinations, medication, respiratory conditions (asthma) and family medical history of atopic diseases
• History of respiratory infections: amount, prior viral testing, symptoms, medication use and symptoms of family members
• Passive smoking
• Physical examination: temperature – blood pressure- hearts rate- respiratory rate- cardiac sounds – breath sounds – rhinorrhoea (all part of routine preoperative medical screening/ care)
• Additional examination: Chest x-ray- Electrocardiogram (ECG)- Blood tests (C-reactive protein (CRP), Leukocytes) (all part of routine preoperative medical screening/ care)
On day of operation (i.e., day 1)
Collection of operating conditions, including:
• Anaesthesia: dexamethasone given because of bypass yes/no-type of induction-endotracheal tube size (ETT)-redness or swelling during laryngoscopy – secretions (pus) seen during intubation-high pressures needed during mechanical ventilation in the operation room (OR)-duration of anaesthesia-administration of ketamine yes/no-continuous administration of ketamine yes/no-amount of red blood cells, fresh frozen plasma and platelet concentrate transfused
• Operation: Type of operation, risk adjustment congenital heart surgery score (RACHS-II) [14]-duration of cardiopulmonary bypass (CPB)-duration of aortic-cross clamping-antegrade cerebral perfusion
Daily until PICU discharge
Collection of clinical condition, including:
• Administered steroids
• Infection: Infection parameters (routinely performed)-use of medication (antiviral/ antibacterial)-recording of any bacterial/ viral testing of respiratory tract- temperature (highest recorded per day)
• Ventilation: settings (mean airway pressure, fraction of inspired oxygen (FiO2), Peak inspiratory pressure and positive end expiratory pressure (PEEP) (maximal values))-use of non-invasive ventilation (continuous positive airway pressure (CPAP), optiflow, face mask ventilation)- use of nitric oxide- failure of extubation (reintubation within 24 hours after extubation)
• Inotropes, vasoactive medication (milrinone, adrenaline, noradrenaline, dobutamine, dopamine, levosimendan)
Date of PICU and hospital discharge.
On day of operation (i.e., day 1): nasopharyngeal swab.
On day 4, if still intubated: nasopharyngeal swab and blood from the biochemical laboratory (residual material).
After collection, respiratory specimens (nasopharyngeal swabs) will be transported to the Clinical Microbiology Laboratory for further processing and storage. Respiratory specimens will be processed daily (with routine diagnostics) and stored at –80°C. Blood samples will be stored at –80°C until testing. After the first testing is done, all samples will be stored 15 years after the study inclusion has ended.
Viral testing
Testing of rhinovirus in specimens (nasopharyngeal swab, blood) will be performed at the Clinical Microbiological Laboratory of the LUMC using a validated internally controlled real-time rhinovirus PCR, yielding semi–quantitative results based on Cycle threshold (Ct) values.[15] Rhinovirus genotyping will be performed by PCR and/or amplification and sequence-analysis of the capsid proteins VP3/VP1, VP4/VP2 or the 5’UTR genome regions previously described by Zlateva et al. [16].
Other respiratory viral pathogens
In case of suspected clinical infectious respiratory problems during PICU admission, clinical routine microbiological diagnostics will be performed for respiratory viral pathogens at the discretion of the treating physician. The results of these clinical tests will also be evaluated in the final data analysis to help establish the role of potential co-infections in rhinovirus positive patients and the role of other viral infections in rhinovirus negative patients.
In rhinovirus negative patients with a prolonged duration of mechanical ventilation and/or PICU length of stay (>3 days), at final analysis of the study results, the initial per-operative nasopharyngeal swabs will be re-tested for other viral pathogens with in-house real-time multiplex PCR (eg RSV, influenza, parainfluenza, etc) to analyse the effect of possible other viral pathogens on the prolonged LOS [15].
Statistical analysis
Dichotomous variables will be expressed in numbers and percentages.
Continuous variables will be expressed as (exponential) means with standard deviations (SD) or medians with interquartile ranges [IQR], where appropriate.
Outcome measures, viral load and demographic features will be expressed for the total study population. In addition, these data will be shown for the following subgroups: rhinovirus infection (overall), symptomatic rhinovirus infection, asymptomatic rhinovirus infection and no rhinovirus infection at admission.
Multivariate analysis
The primary and secondary outcome measures will be compared between the rhinovirus PCR positive patients versus the rhinovirus PCR negative groups.
Because we expect the distribution of our primary outcome (IC length of stay) to be skewed, we will use exponential regression for our primary analysis. We will correct for potential confounders: gender and perfusion time. Numerical outcomes that do not show strong deviation from normality will be analysed with multivariate linear regression. Logistic regression or log-binomial regression where appropriate, will be used for all dichotomous or categorical outcome measures, corrected for potential confounders.
In children with rhinovirus infection investigate the association between viral load (strength of PCR), duration of shedding, symptomatic or asymptomatic infection, genotype, viremia and the primary and secondary outcome measures shall be investigated.
Adjustment and stratification
Variables that can affect both LOS and peroperative RV PCR positivity (confounders) are adjusted for (age) (Figure 2).
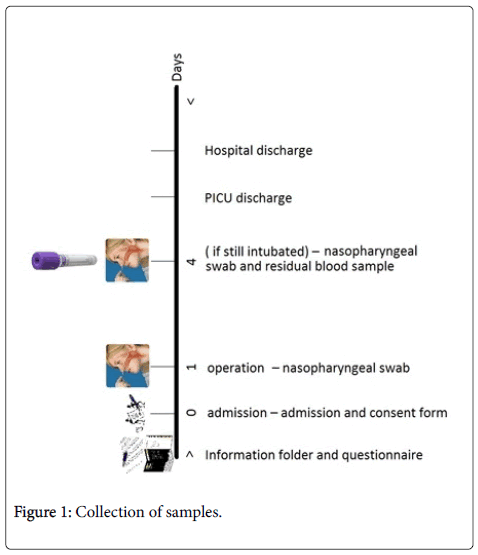
Figure 1: Collection of samples.
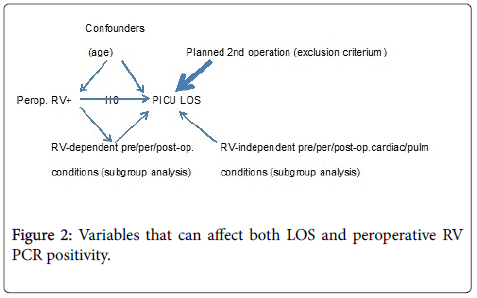
Figure 2: Variables that can affect both LOS and peroperative RV PCR positivity.
Variables that can affect LOS without affecting RV PCR positivity are either implemented as
(a) exclusion criteria, when having an absolute effect on LOS, independent of RV PCR positivity, e.g.:
• planned 2nd operation for single ventricle physiology
• planned prolonged intubation because of (MRI) procedure or transport to other hospital
• unplanned 2nd operation (exclusion retrospectively)
(b) subgroup, when having a less absolute effect on LOS, e.g.,
• pre-operative cardiac condition
• pre-operative viral co-infection
• Here, subgroup analysis might indicate patients vulnerable for enhanced LOS when per-operative RV positive
(c) other predictors for LOS that are either theoretically independent of RV or potentially resulting from RV positivity: no adjustment:
• Per-operative perfusion time (cardio-pulmonary-bypass-time)
• Post-operative cardiac condition e.g., heart failure leading to prolonged inotrope support and/or respiratory support
• Pre/post-operative pulmonary condition (e.g., tracheabronchomalacia)
Number of patients excluded from the study will be presented in a Consolidated Standards of Reporting Trials (CONSORT)-flow-chart.
This is, to our knowledge, the first study to screen all children undergoing elective cardiac surgery for rhinovirus and to monitor postoperative outcome. It is important to determine whether rhinovirus is a risk factor for prolonged LOS in children undergoing heart surgery as it might have important implications in timing of the operation.
We expect that the effect of rhinovirus on the difference in PICU LOS is the largest in children undergoing open heart surgery using cardiopulmonary bypass compared to operations without cardiopulmonary bypass (e.g., repair of coarctation of the aorta, placement of a modified Blalock-Taussig shunt).
Secondary aim of the study is to develop an algorithm, based on clinical parameters and nasopharyngeal swab results, to help identify asymptomatic children with an increased risk of prolonged PICU LOS after cardiac surgery, in the pre-operative stage. The ultimate goal is to prevent prolonged PICU admission due to respiratory complications.
In this study the children will be tested for rhinovirus at the moment of operation.
Though this moment may not exactly represent the moment of admission (one day earlier), we have chosen this moment to minimize the burden for the participating children.
It must be noted that if rhinovirus positivity is indeed predictive for prolonged PICU LOS, this study is not designed to determine whether postponing the operation is effective in preventing prolonged PICU LOS, which would require a specific future trial randomizing between different postponement times (e.g., 2, 4 or 6 weeks). We chose not to perform this trial immediately because we think the effect of rhinovirus needs to be determined on forehand. Furthermore the organisation and costs, as well as the emotional burden for the children and their family of postponing an operation are considerable and can only be warranted if rhinovirus actually is a risk factor.
While duration of mechanical ventilation seems to be more directly related to rhinovirus infection than PICU length of stay, we selected PICU length of stay as primary endpoint. Duration of mechanical ventilation as an endpoint is more difficult to define, given the several types of respiratory support (invasive and non-invasive) and less clear-cut situations like extubation failure and or re-intubation. Because PICU length of stay is a more clear endpoint, easier to compare between studies, and of clinical and economical relevance, we chose this as primary endpoint.
Rhinovirus will be the only respiratory pathogen that is routinely tested on the pre-operative nasopharyngeal swabs in this study. However, all nasopharyngeal swabs will be stored and can be retested for an entire respiratory viral panel in rhinovirus negative patients with prolonged LOS (>4 days) to exclude patients with prolonged length of stay due to another virus.
We have designed a prospective observational study to determine the effect of rhinovirus on the postoperative course in children who are admitted from home to undergo elective congenital heart surgery. The primary endpoint is PICU LOS.
Approved by the Medical Ethical Committee Leiden University Medical Center (Protocol 14.303). Planned start date is 23 June 2015.
Trial registration: ClinicalTrials.gov Identifier NCT02438293; registration date 5 May 2015.
The author’s declare that they have no competing interests.