Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Protocol Article - (2015) Volume 5, Issue 6
Background: The current standard technique for prostate cancer detection is trans-rectal ultrasound (TRUS) guided biopsy, and is renowned for its low sensitivity. Developments of multiparametric MRI techniques have increased the detection of significant prostate cancer. Currently there are three techniques utilizing MRI for targeted biopsy; MRI-TRUS fusion; ‘cognitive’ TRUS, and in-bore MRI guided biopsy. There is no consensus which should be preferred. The current study aims to compare prostate cancer detection rates of three target biopsy procedures.
Methods: The FUTURE trial is a three-arm randomised controlled, multicentre trial comparing three techniques of MRI targeted biopsy of the prostate amongst subjects with one prior negative TRUS biopsy and a persisting suspicion on prostate cancer. All subjects undergo mpMRI imaging. Images will be centrally reviewed, and evaluated using the ‘Prostate imaging reporting and data system’. An estimated 69% of the subjects will demonstrate tumour suspicious findings on mpMRI, and will be randomised 1:1:1. The primary objective is to compare (significant) tumor detection rates of the three techniques. Secondary objectives include histopathological validation of mpMRI imaging and PI-RADS classification, a cost-effectiveness analysis, and follow-up after a negative mpMRI or negative target biopsy. All biopsy cores will be evaluated by one dedicated uro-pathologists per center. Two sub-investigations were based on the hypothesis that MRI-TRUS fusion and in-bore MRI biopsy demonstrate similar tumor detection, whilst MRI-TRUS fusion demonstrates increased tumor detection compared to ‘cognitive’ TRUS biopsy. A total number 466 of subjects is needed for equal randomization. Assuming that 69% of subjects have tumor suspicious findings on MRI imaging, a total of 675 subjects are required for inclusion.
Discussion: For target biopsy procedures of the prostate the ultimate comparator is histopathological examination of radical prostatectomy specimens, though this leads to insurmountable ethical objections and thus to a methodological dilemma concerning validation.
Keywords: Prostate cancer; mpMRI; Image guided biopsy; Image fusion; Diagnosis; RCT
TRUS: Transrectal Ultrasound; TDR: Tumour Detection Rates; mpMRI: Multiparametric Magnetic Resonance Imaging; ESUR: European Society of Uro-Radiology; T2W: T2 Weighted ; DWI: Diffusion Weighted Imaging; DCE: Dynamic Contrast Enhanced; PI-RADS: Prostate Imaging Reporting And Data System; MRGB: Magnetic Resonance Guided Biopsy; MTF: MRI-TRUS Fusion; CONSORT: Consolidated Standards of Reporting Trials; SPIRIT: Standard Protocol Items: Recommendations for Interventional Trials; DRE: Digital Rectal Examination; UTI: Urine Tract Infection; IPSS: International Prostate Symptom Score; IIEF-5: International Index of Erectile Function-5; iPCQ: Productivity Cost Questionnaire; iMCQ: Medical Consumption Questionnaire; ISUP: International Society of Urological Pathology; PSA: Prostate Specific Antigen; ERSPC: European Randomized Study of Screening for Prostate Cancer; CRF: Case Report Form
Prostate cancer is the most commonly diagnosed malignancy amongst men in the Netherlands, with an increasing incidence under the influence of aging of males [1,2]. The current standard technique for prostate cancer detection is trans-rectal ultrasound (TRUS) guided biopsy of the prostate [3,4]. TRUS guided biopsy has its limitation due to the inability of grey-scale ultrasonography to distinguish prostate cancer from benign prostate tissue [4,5]. Consequently TRUS-guided biopsies are performed in a systematic manner in contrast to targeted biopsies, typically by taking 8-12 biopsy cores from the peripheral zone of the prostate. Due to these limitation TRUS guided biopsy is renowned for its high detection rates of insignificant cancers, and low sensitivity for significant cancers, which is underlined by the fact that repeat TRUS biopsy, due to a persisting clinical suspicion of prostate cancer, has a tumour detection rate (TDR) of 10-25% following prior negative biopsy [6-10].
The combination of serum PSA (prostate specific antigen) screening and systematic TRUS biopsy has lead to an increased detection of early prostate cancer. A disadvantage of PSA screening is the risk of over-diagnosis and over-treatment of clinical insignificant or low-risk prostate cancer [11]. The Gleason score is the current standard grading system used to assess the differentiation grade of adenocarcinoma of the prostate. The Gleason score is the sum of the predominant and the highest most common histological pattern of tumor growth. Gleason scores 2-4 are not assigned on needle biopsy, thus Gleason sum score varies from 5 to 10 [3,4,12]. Based on the serum PSA concentration, clinical stage, Gleason sum score, number of core positivity, and cancer core length a distinction is made between clinically significant and insignificant prostate cancer according to the Epstein criteria [13,14]. Clinically insignificant prostate cancers represent indolent, low-risk malignancies that require no immediate form of active treatment, whereas clinically significant disease represents intermediate and high-risk malignancies that warrant some form of active treatment [3,13,14].
Development of multiparametric MRI (mpMRI) techniques has increased the detection of significant cancers and the sensitivity for the determination of its aggression [15-22]. Clinical guidelines advise performing an mpMRI when the clinical suspicion on prostate cancer persists despite prior negative TRUS biopsy results to investigate the possibility of ventrally located lesions [3,4]. According the European Society of Uro-Radiology (ESUR) 2012 and the ESUR/American College of Radiology (ACR) 2014 guidelines an mpMRI consists of high-resolution T2-weighted images (T2W), and at least two functional MRI techniques (such as Dynamic Contrast Enhanced (DCE) imaging and Diffusion Weighted (DWI) imaging) [3,4,15,23,24]. Usage of a 3 Tesla (3-T) magnet has enhanced resolution and quality of imaging compared to 1.5-T, and possibly leads to an even better detection of prostate cancer using MRI imaging [23]. A method to systematically evaluate mpMRI of the prostate is by using the ‘Prostate Imaging Reporting And Data System’ (PI-RADS) scoring system, by which imaging abnormalities are scored 1-5 based on each MR imaging modality [15,23,24]. The higher the PI-RADS score, the higher the risk of presence of malignancy [25,26].
Following the development of enhanced quality of imaging, MRI guided interventions have been introduced. There are several techniques available to utilize MRI information for direct targeted biopsies of the prostate. Using in-bore MRI guided biopsy (MRGB) real-time MR imaging is performed to guide the biopsy procedure. A recent systematic review demonstrated increased TDR of significant prostate cancer in a large cohort using MRGB [17,22,27]. Despite these results MRGB remains controversial due to impracticalities, as its low availability, required expertise and time consuming nature. An upcoming technique is MRI-TRUS fusion (MTF) targeted biopsy [28-38]. MTF devices utilise the high diagnostic yield of the mpMRI for prostate cancer in combination with the practicality and affordability of TRUS biopsy systems by fusing the pre-interventional MR images with real-time ultrasound images. Thus enabling MRI-targeted biopsy without the necessity of performing the biopsy in an MRI suite. A third commonly applied technique for MRI target biopsy is ‘cognitive’ TRUS target biopsy. The mpMRI information is used to ‘cognitively’ by the physician to target tumour suspicious areas of the prostate using TRUS without applying image fusion [39,40]. All these techniques demonstrate an increased TDR of significant prostate cancer compared to systematic TRUS biopsy [17,25-36,39-42]. There is no consensus which technique for targeted biopsy should be preferred. So far no multicenter, randomized controlled trials have been performed comparing prostate cancer detection rates of MTF, ‘cognitive’ TRUS, and MRGB respectively.
Objectives and hypothesis
The main objective of this study is to evaluate the clinical role of MTF biopsy on prostate cancer detection, compared with MRGB and ‘cognitive’ TRUS biopsy, in men with a persistent clinical suspicion on prostate cancer and at least one negative TRUS guided biopsy session. The hypothesis is that MTF demonstrates a similar TDR of prostate cancer compared to MRGB, whilst demonstrating an increased TDR compared to ‘cognitive’ TRUS biopsy.
Secondary objectives include histopathological validation of mpMRI imaging and PI-RADS classification in all subjects undergoing target biopsy of the prostate using biopsy cores (and radical prostatectomy specimen), a cost-effectiveness analysis of all three target biopsy techniques, and an evaluation of the follow-up amongst subjects with a negative mpMRI or negative target biopsy outcome. It is hypothesized that all three techniques of targeted biopsy demonstrate similar TDR compared to systematic biopsy, but an increased TDR of significant prostate cancer compared to systematic TRUS. Furthermore targeted biopsies are expected to predict the definitive Gleason sum score of radical prostatectomy specimens more accurately compared to systematic TRUS. Our hypothesis is that MRI is a crucial factor in patient selection for subsequent target biopsy procedures. Patients without tumour suspicious abnormalities on mpMRI will demonstrate a low TDR during follow-up.
Study design
The FUTURE trial is a three-arm randomized controlled, multicentre trial. Primarily all subjects will undergo mpMRI imaging of the prostate in accordance to the ESUR guidelines. If imaging does show abnormalities equivocal or suspicious for tumour (PI-RADS>2), subjects will be randomised to undergo one of three target biopsy strategies. If mpMRI imaging does not show abnormalities suspicious for tumour (PI-RADS ≤ 2) subjects will enter a biochemical follow-up course of at least 2 years. See Figure 1 for a schematic overview of the trial design. Based on our hypothesis 2 sub-investigation were proposed; sub-investigation 1 consists of superiority study comparing the TDR of MRF and ‘cognitive’ TRUS biopsy; and sub-investigation 2 consists of a non-inferiority study comparing the TDR of MRF and MRGB. The study design and protocol drafting for the FUTURE trial was performed in adherence to the CONSORT, SPIRIT and START recommendations for reporting on interventional trials [16,43,44].
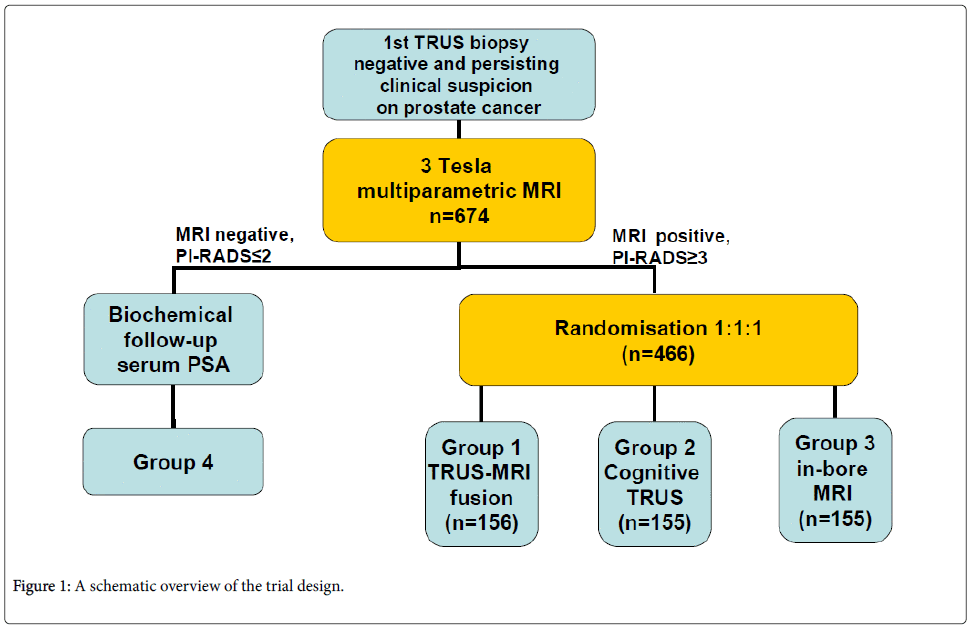
Figure 1: A schematic overview of the trial design.
Setting and participants
The FUTURE trial is conducted in two large, non-academic teaching hospitals and one academic hospital in the Netherlands. Eligible patients can be referred to inclusion centres from surrounding health care centres for study recruitment. Eligible patients for study participation must meet all the following inclusion criteria:
• Subject is at least 18 years old and mentally competent.
• Subjects have undergone at least one prior negative TRUS guided biopsy session within the last 4 years, with a minimum of 8 biopsy cores taken from the peripheral zone.
• Subjects have a persisting clinical suspicion on prostate cancer based on a PSA value of>4.0 ng/ml and/or suspicious digital rectal examination (DRE).
Subjects are excluded if one of the following criteria applies:
• Prior diagnosed or treated prostate cancer, including subjects with histologically proven low-risk prostate cancer submitted to active surveillance protocols.
• Prior targeted biopsy procedures of the prostate based on MR imaging.
• Proven urine tract infections (UTI).
• Contra-indications for MR imaging.
• Unwillingness or inability to undergo target biopsy procedures and biochemical follow-up.
Recruitment
Recruitment for study participation will be initiated by the treating urologist. If a subject is found to meet in- and exclusion criteria an appointment will be made at one of the inclusion centres for enrolment. At this appointment the study design will be discussed with subjects, inclusion and exclusion criteria will be reviewed, written informed consent will be obtained and all baseline data will be collected. Further appointments for study activities will be made (e.g., date of MRI imaging). By recruiting subjects from surrounding referral health care centres inclusion rates are to be boosted. In order to facilitate recruitment amongst referral centres oral presentation will be held at for participating urologists per centre and during the annual meeting of the Dutch Uro-Oncological Studygroup (DUOS). Written and digital information concerning the trial is to be disseminated amongst urologists.
Intervention
Primarily all included subjects will undergo 3 T mpMRI imaging of the prostate in accordance to the ESUR guidelines using one of the following scanners (MAGNETOM Skyra® Siemens; MAGNETOM Trio® Siemens; Ingenia® Philips) [15]. The imaging modalities used include high resolution T2W, DWI and DCE. Anti-peristaltic drugs (Buscopan®) and gadolinium intravenous contrast-agent will be administered during imaging. All images will be evaluated by a single experienced urogenital radiologists by applying central review. Images will be evaluated using the PI-RADS 2.0 scoring system [23,24]. Furthermore all subjects are required to fill in 5 sets of validated questionnaires at baseline. Questions are directed at micturition (IPSS), erectile function (IIEF-5), global health perception (EQ-5D-5L), medical consumption (iMCQ) and productivity (iPCQ). These questionnaires will be repeated one month following biopsy procedure.
If imaging demonstrates equivocal or suspicious findings (PI-RADS>2) subjects will be subjected to one of three targeted biopsy procedures. Axial T2W and DWI imaging are used to direct all biopsy procedures. Starting the day prior to the biopsy all subjects will receive a 3 day course of prophylactic antibiotics (typically a fluorchinolone).
MRI-TRUS fusion (MTF) targeted biopsy is performed using the BiopSee® transperineal device for stereotactically navigated biopsies by Medcom. This system fuses pre-interventional mpMRI images with real-time ultrasound images, as described earlier. Using the BiopSee® fusion device a transperineal approach is used for prostate biopsies under ultrasound guidance. At least 2 biopsy cores are taken per identified lesion. Additionally this technique allows systematic biopsy cores to be taken during the same procedure as target biopsy. The systematic biopsy cores are taken using a predefined schema which includes at least 2 transition zone cores and 2 ventrally directed cores. The number of systematic cores taken varies between 8-12 depending on the volume of the prostate. The biopsy procedures are performed on the operating room under spinal or general anaesthesia, in day care clinical setting. Prior to biopsy subjects receive an enema (Mircolax®).
‘Cognitive’ TRUS targeted biopsy using either the Hitachi Preirus®, Hitachi Avius® or BK UltraView 800® ultrasound system. Both systems are equipped with a bi-plane transrectal ultrasound transducer and a needle guidance application (end-fire and side-fire respectively). The prostate is biopsied using a transrectal approached under ultrasound guidance. The mpMRI images are reviewed directly prior to ‘cognitive’ TRUS biopsy. At least 2 biopsy cores are taken per identified lesion. Additionally this technique allows systematic biopsy cores to be taken during the same procedure as target biopsy using the same biopsy scheme as described above. The biopsies are performed in the outpatient urology clinical setting without the use of anaesthesia.
In-bore MRI guided biopsy (MRGB) using a 3-T MRI scanners (MAGNETOM Skyra® Siemens) described earlier. The prostate is biopsied using a transrectal approached using an MRI compatible biopsy gun (Invivo®) under MRI guidance. At least 2 biopsy cores are taken per identified lesion. MRGB is performed in the out-patient clinical setting without the use of anaesthesia. This technique does not allow systematic biopsy cores to be taken during the target biopsy procedure.
All biopsy specimens will be reviewed by one dedicated uropathologists per centre. Biopsy cores will be potted with a maximum of three specimens per vial. Target cores will be potted, and analysed separately from systematic cores. Cores will be evaluated in accordance to the 2005 International Society of Urological Pathology (ISUP) conference on Gleason grading of prostatic carcinoma [12]. Evaluation of the biopsy cores will at least include histological diagnosis, Gleason sum score, length of core, length of prostate cancer within the core, and number of cores with/without cancer.
Follow-up
Subjects without tumour suspicious findings (PI-RADS ≤ 2) on mpMRI will enter a biochemical follow-up course consisting of annual PSA measurements. In case PSA measurements surpass a subject specific threshold (based on baseline value and prostate volume) a repeat mpMRI will be performed. Repeat biopsy will follow in case of rising PSA above predefined threshold and/or progression on mpMRI. Biochemical follow-up will be performed by principle referring urologist. Two years following inclusion a patient file review will be performed to determine whether the diagnosis prostate cancer has been made, what diagnostic tools have been used and their outcomes.
Subjects with equivocal findings (PI-RADS 3) on mpMRI and negative outcomes of subsequent targeted biopsy procedures will also enter a biochemical follow-up course consisting a biannual PSA measurement and repeat mpMRI after one year. Repeat biopsy will follow in case of rising PSA above the predefined threshold and/or progression on mpMRI. Two years following inclusion a patient file review will be performed to determine whether the diagnosis prostate cancer has been made, what diagnostic tools have been used and their outcomes.
Subjects with tumour suspicious findings (PI-RADS>3) on mpMRI and negative outcomes of subsequent targeted biopsy procedures are offered to undergo direct repeat MRGB (cross-over). Two years following inclusion a patient file review will be performed to determine whether the diagnosis prostate cancer has been made, what diagnostic tools have been used and their outcomes.
Subjects with equivocal or tumour suspicious findings (PI-RADS>2) on mpMRI who have undergone subsequent targeted biopsy procedures will be contacted one month following the biopsy procedure. During this contact morbidity due to biopsy procedure will be discussed, and subjects will be required to complete a follow-up round of questionnaires.
Outcomes
The primary outcome of the FUTURE trial is overall prostate cancer TDR. Overall prostate cancer TDR will be presented per subject and per biopsy core for both target biopsy alone, systematic biopsy alone, and the combination of systematic and target biopsy. Target biopsy is assumed to demonstrate an increased TDR of significant prostate cancer. The definition of significant prostate cancer derived from the internationally accepted Epstein criteria and d’Amico risk classifications [13,14,45,46].
Criteria for insignificant prostate cancer are:
• PSA<10 ng/ml.
• PSA-density<0.15ng/ml/ml.
• Gleason 3+3, <2 cores positive and maximum cancer core length<6mm.
• Gleason 3+4, <2 cores positive and maximum cancer core length<4mm.
• Clinically organ confined disease.
Primary parameters are histological diagnosis, Gleason sum score, cancer core length, and ratio of (systematic/targeted) core positivity. Secondary parameters include number of mpMRI suspicious lesions, PI-RADS score of lesions, imaging staging, and pathological staging (if applicable). Furthermore baseline data will be collected on PSA value, prostate volume (TRUS), clinical stage (based on DRE and TRUS), age, number of previous negative biopsy sessions, MR imaging parameters used, risk on prostate cancer based on the ERSPC algorithm [47], self-reported outcomes on micturition, erectile function, global health perception, medical consumption and productivity (prior/following biopsy). Furthermore data will be collected concerning the occurrence of adverse events following biopsy. See Table 1 for an overview of outcomes and the moment of measurement.
| Parameters | T1 (inclusion) | T2 (following MRI imaging) | T3 (1 month following biopsy) | T4 (follow-up 2 years) |
|---|---|---|---|---|
| Age | X | |||
| PSA value | X | |||
| Biopsy history | X | |||
| Prostate volume | X | |||
| Clinical stage | X | |||
| Risk algorithm | X | |||
| EQ-5D-5L/IPSS/IIEF-5 | X | X | ||
| iPCQ/iMCQ | X | X | ||
| UTI screening | X | |||
| MRI parameters used | X | |||
| Lesion number, size | X | |||
| PI-RADS score | X | |||
| Imaging stage | X | |||
| Biopsy allocation | X | |||
| Histological diagnosis | X | |||
| Gleason score | X | |||
| Core positivity; cancer length | X | |||
| Diagnosis prostate cancer | X | X | ||
| Adverse events/treatment | X | |||
| Pathological stage | X | |||
| Follow-up | X |
Table 1: An overview of all outcome measures and the moment of measurement.
Sample size calculation
The sample size calculation was determined by the estimated TDR of the three biopsy techniques, an estimation of the incidence of tumour suspicious findings within our cohort and the applied sub-investigation. Based on a recent systematic review an estimated 69% of the subjects with prior negative biopsy outcomes and a persisting clinical suspicion on prostate cancer will demonstrate tumour suspicious findings on MRI (PIRADS ≥ 3).(41) Based on peer reviewed literature an estimated yield of TDR was 40% for MRGB, 40% for MTF, and 25% for ‘cognitive’ TRUS within this population [22,26,41]. A power of 80%, a significance level of 5%, and a range of indifference of 15% were used for subsequent calculations. Sample size calculations were performed using WINPEPI software version 11.29.
For sub-investigation 1 (superiority study) group sample sizes of 152 per group achieve an 80% power to detect a difference of 0.15 between the null hypothesis (‘cognitive’ TRUS) and alternative hypothesis (MTF) using a two-sided Chi-square test without continuity correction and with a significance level of 0.05, assuming that cognitive biopsy has a TDR of 0.25 and MTF of 0.40.
In sub-investigation 2 (non-inferiority study) group sample sizes of 131 per group achieve an 80% power at a significance level of 0.05 using a one-sided equivalence test of proportions when the proportion in the standard group (MRGB) is 0.40 and the proportion in the experimental group (MTF) being tested for non-inferiority is 0.40 and the maximum allowable difference between these proportions that still results in non-inferiority (the range of indifference) is 0.15. The range of indifference of 0.15 was chosen because the TDR of MTF biopsy is estimated to lay in between the TDR of ‘cognitive’ TRUS biopsy (0.25) and the TDR of MRGB (0.40). The basis to perform a one-sided equivalence test instead of a two-sided equivalence test is that the MTF performs biopsies on MRI derived targets, and consequently is not expected to show a superior TDR compared to MRGB.
A sample size of 152 per group for sub-investigation 1, and a sample size of 131 per group are needed to achieve statistical significance. To facilitate the randomization procedure identical group sizes were chosen for all three groups. This implicates 21 additional subjects in the MRGB group only and results in a sample size of 152 per group, and 456 subjects for all three biopsy procedures combined. 10 additional subjects are to be included to correct for possible lost-to follow up. By including subjects of the MTF group for the analysis of both the superiority and non-inferiority study, a total number of 466 subjects is needed for equal randomization amongst the three target biopsy strategies. Assuming that within this population 69% of subjects demonstrate tumour suspicious findings on MRI imaging, a total of 675 subjects are required for inclusion.
Randomisation
All subjects with equivocal or tumour suspicious findings (PI-RADS>2) on mpMRI imaging will be randomized to undergo target biopsy strategy. Randomization is performed by applying bloc-randomization using a web-based randomization system. The administrator of the web-based system was not involved in any trial activities. The administrator of the web-based system generated a computer based random sequence assigning intervention arms. All subjects will be randomized 1:1:1 to undergo MRF, MRGB or ‘cognitive’ TRUS target biopsy. To prevent uneven distribution amongst the three intervention arms bloc-randomization was applied. The number of subjects per bloc varies. The investigators are blinded for the random sequence used and the bloc size used. Following randomization the allocated intervention will be revealed to both investigator and subject.
Data collection and management
Upon enrolment all subjects will be assigned a trial code. This code consist of the name of the trial, the inclusion centre were subject was enrolled, and a subject specific number. All data will be collected on a tailored CRF, under mention of the subject specific trial code. The key for encoding is stored by principle investigators at each of the inclusion sites. Access to data will be limited to main-investigators and supervising urologist. Collected data will be recorded digitally in the electronic patient file on secured hospital servers used by each inclusion site, as well as on the hardcopy CRF.
Statistical analysis
All analyses will be conducted using SPSS version 22.0 (Statistical Package for Social Sciences, IBM). A 0.05-significance level will be adopted in all statistical tests. Descriptive statistics will be used to describe baseline characteristics as means and standard deviation. To assess comparability between the three target biopsy groups baseline characteristics will be analysed using a Chi square test, or t-test (depending on variable type). The overall TDR, and clinically significant TDR will be compared between the three intervention groups using a t-test. If despite randomization confounding factors have been found in baseline characteristics a multivariate logistics regression test will be applied. Furthermore the overall TDR, and clinically significant TDR will be compared between the systematic biopsy outcomes and targeted biopsy outcomes in subjects that have undergone both systematic and targeted biopsies using a Mc Nemar test. A sub-group analysis will be performed on subjects with PI-RADS 3, 4, and 5 abnormalities on mpMRI imaging respectively. Statistical analysis will be performed on an intention-to-treat basis. Subjects with missing data will not be substituted for other subjects. Missing and incomplete data will be described.
Ethical considerations
This study will be conducted in accordance with the principles of the Declaration of Helsinki (version 10, amended in October 2013 by the 64th WMA General Assembly). The research protocol was examined and approved by the regional accredited Medical research Ethical Committee ‘MEC-U’ (Medical research Ethics Committees United) (reference R14.021, dossier NL48777.100.14). Institutional review board approval was granted for each of the participating centres. The research protocol was registered in the Dutch National Trial Register (reference NTR4988). All participating subjects will sign a written informed consent form.
The FUTURE trial is a multicentre randomized controlled trial on three target biopsy techniques in the diagnostic work-up of prostate cancer. Typically diagnostics are compared to a ‘golden standard’ as reference standard for the outcome of the diagnostic tool being investigated. For a diagnostic intervention such as biopsy the ultimate comparator would be histopathological examination of the target organ, in this case the prostate. Though this results in insurmountable ethical objections due to the fact that the reference standard of radical prostatectomy may harbour considerable morbidity, and on ethical grounds cannot be performed on subjects without histologically proven prostate cancer. Consequently a methodological dilemma is inevitable on how to validate the findings of biopsy procedures. An alternative methodological strategy is to perform a repeat of the current standard diagnostic procedure (systematic TRUS biopsy) on all subjects, but as previously described this intervention has a limited sensitivity. Furthermore it is technically not feasible to perform systematic biopsies in the MRGB group during in the same session. Consequently subjects would have to undergo MRGB followed by systematic TRUS biopsy in a subsequent session. Potentially this would result in significant resistance amongst subjects undergoing these procedures and could therefore negatively influence subject’s willingness to participate in the trial.
In recent years a lot of experience has been gained using targeted biopsy strategies. From the three techniques currently being investigated the most experience has been acquired with MRGB. The medical scientific research validating this technique of targeted biopsy has been most extensive. For that practical reason this test was chosen as validation test in subjects with tumour suspicious findings on mpMRI (PI-RADS>3), and a negative outcome of primary targeted biopsy procedures of these lesions. Furthermore validation is performed by systematic biopsy during the same target biopsy session (in the MTF and ‘cognitive’ biopsy groups), and by a serum PSA test follow-up course of at least 2 years.
In summary the current standard technique for prostate cancer diagnosis has its limitations. Improvement of mpMRI techniques has enabled targeted biopsy. There are three techniques of targeted biopsy. The main objective of this study is to evaluate prostate cancer detection rates of three target biopsy procedures by comparing MTF biopsy with MRGB and ‘cognitive’ TRUS biopsy, in men with a persistent clinical suspicion on prostate cancer and at least one negative TRUS guided biopsy session. Furthermore target biopsy outcomes will be compared to systematic biopsy outcomes in subjects that have undergone both targeted and systematic biopsy procedures.
This trial is currently recruiting patients. The start date was December 2014. The initial patient inclusion is expected to take approximately 24 months. Patients will be followed for two years.
This research project has been funded by the St. Antonius Research fund and the St. Antonius Innovation Fund (reference BI13G04EA).
We would like to thank the following hospitals for their cooperation: Zuwe Hofpoort, Woerden; Diakonessehuis, Utrecht/Zeist; Rivierenland, Tiel; Rivas, Gorinchem; St. Jansdal, Harderwijk; VUmc, Amsterdam; Gelre, Apeldoorn; Slingeland, Doetinchem; Bernhoven, Uden; Gelderse Vallei, Ede; Rijnstate, Arnhem. Streekziekenhuis Koningin Beatrix, Winterwijk.
All authors participated in study design, writing, and final approval of the final manuscript.
Trial registration
The Dutch National Trial Register, reference: NTR4988, registration date: December 3rd 2014.
The authors have no conflict of interests to declare.