Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2012) Volume 2, Issue 4
Background: In acute pancreatitis, development of intestinal damage is of clinically importance. Such that, preventing the intestinal damage may restrain severity of the pancreatitis. Erythropoietin which has pleiotropic effects is shown to decrease inflammation, the damage of ischemia-reperfusion, and apoptosis in intestine. Here, it is aimed to obtain the effects of erythropoietin on the intestinal damage caused by the acute pancreatitis.
Methods: Twenty one Wistar Albino rats were separated into three (Sham-Control-EPO) groups. Experimental acute pancreatitis was formed by infusion of the 4.5% Na taurocholate into the pancreatic duct. A 1000 U/kg/day dose of erythropoietin was applied in the EPO group, intraperitoneally for three days. The experiment was terminated on the fourth day. Leukocyte in blood, CRP and amylase in serum were studied whereas catalase and glutathione reductase levels were measured in intestinal homogenate as anti oxidant capacity markers.
Results: Among all groups, leukocyte CRP, and amylase levels did not show significant difference. Mean catalase and glutathione reductase levels of the intestinal homogenates were higher in the EPO group rather than the Control group and were close to that of the Sham. Histological damage severity of the intestine was significantly low in the EPO group compared to the Control group (p=0.04).
Conclusion: Erythropoietin prevents the decrease of the catalase and glutathione reductase levels as anti oxidant capacity in the intestine, and protects the intestine against damage, which develops secondarily to the AP.
<Keywords: Erythropoietin, Acute pancreatitis, Intestinal damage
The inflammatory reaction cascade activated during Acute Pancreatitis (AP) has various local and systemic effects and complications [1]. In this process, especially intestinal damage and bacterial translocation are important factors. The splanchnic microcirculatory dysfunction developing secondarily to the AP leads to intestinal ischemia, which later in the process results in disturbances in the intestinal secretory and epithelial barriers [2,3]. Impairment in the mucosal integrity, finally, leads to an increase in intestinal permeability, to endotoxemia, and to bacterial translocation [4]. The multiple organ damage developing in relation to the severity of the AP determines morbidity and mortality rates [5].
In adults, the kidneys, and in fetuses, the liver is the primary organs to produce erythropoietin (EPO), the basic function of which is to stimulate and regulate the production of erythrocyte. EPO is known to be produced by many other tissues as well in response to physical and metabolic stress [6]. EPO receptors are found in various cell and tissue structures, such as erythroid progenitor cells, endothelial cells, neurons, cardiomyocytes and enterocytes, where it shows pleiotropic effects [7]. Antioxidant, neuroprotective, antiapoptotic and antiinflammatory effects can be counted among the pleiotropic effects [8,9]. These protective effects of EPO have been found to be valid for intestinal damage as well [10-12].
Research to date has not yet revealed the activity of EPO in intestinal damage related to the AP. The aim of this study is to examine the effects of EPO on intestinal damage developing in an experimental AP.
The study was conducted in the University Experimental Research Center after obtaining the approval of the Animal Research Local Ethics Committee (10.02.2010/2). All the subjects were fed and treated in accordance with the international guidelines. A total of 21 male Wistar Albino rats weighing 150-200 gr were used. These were divided into three groups of 7 rats each, namely Sham (Group 1), Control (Group 2), and EPO (Pancreatitis + EPO - Group 3). In all the groups, the experiment was terminated on the fourth day (96th hour). In the EPO group, a 1000 U/kg/day (5 IU) dose of EPO (Eprex 2000 IU/0.5 ml, Gürel Ilaç Ticaret, Istanbul) was administered intraperitoneally for three times.
Surgical technique
All surgical and medical interventions were realized by the same team. The surgical procedures were carried out in standard and sterile conditions. For general anesthesia, 50 mg/kg ketamine and 10 mg/kg xylazine was administered intramuscularly.
The anterior abdominal wall of the subjects were shaved and scrubbed with povidone iodine. An upper midline laparotomy was performed and the duodenum was pulled downward and laterally. The pancreatic duct was revealed and was entered transduodenally with a 26 G catheter. In the sham group, 0.2 cc of serum physiologic (SF) was administered through slow infusion, while 4.5% Na taurocholate solved in 0.2 cc SF was administered in the Control and EPO groups. The transduodenal catheter entrance was sutured with 6/0 prolene, while the anterior abdominal wall was closed with 3/0 silk. One hour after the operation and the following two days (24th and 48th hours), appropriate volume of EPO in EPO group and a volume of 5 IU SF in Sham and Control groups were applied intraperitoneal. On the fourth day (96th hour) of the experiment, after standard preparation and relaparotomy, all the subjects were sacrificed by drawing blood from the abdominal aorta with a punction. In the blood, leukocytes, and in serum, CRP and amylase were examined.
The pancreas and ileum tissues were removed. A part of the pancreas and ileum were placed in a 10% formaldehyde solution for histopathological examination. The other part of the ileum was irrigated with KCL solution and SF, and without delay, preserved at -80°C until antioxidant [catalase, glutathione reductase (GSHrx)] capacity measurement.
Preparation of tissue homogenate
The ileum tissue was irrigated with distilled water and cold 1.15% KCl solution, respectively. Then, it was centrifuged at 10000 g for 20 minutes in a solution (5 ml/mg tissue) with a pH of 7.4 containing KCl (1.15%), EDTA (1 mM), ε-amino caproic acid (0.25 mM) and phenylmethylsulfonyl fluoride (0.1 mM) to form the homogenate. The supernatant part was extracted, distributed over Eppendorf tubes, and preserved in a refrigerator at -80°C until the enzyme activity measurements. Catalase and glutathione reductase enzyme activities were measured with methods described by Aebi and Carlberg [13,14].
Histopathological examination
From the prepared pancreas and ileum paraffin blocks, 6 μm thick sections were taken, stained with hematoxylin-eosin, and examined under a light microscope. The pancreas sections of different regions were evaluated with the modified Schmidt scoring [15]. Accordingly, interstitial edema, leukocyte infiltration, acinar cell necrosis, and hemorrhage were scored between 0 and 3.
The ileum sections were evaluated with respect to inflammation, edema, villus structure, crypt structure and necrosis [16]. The scoring values consisted of those with no change (0), slight change (1), moderate change (2), and serious change (3).
Statistical analysis
For comparison among the groups, Kruskal-Wallis variance analysis, and between pairs of groups, Mann Whitney U tests were used. Statistical significance was determined as p<0.05. Values were presented as mean ± standard deviation (SD) or mean ± standard error (SE) due to the normal distribution of the data or not.
No mortality was observed in any of the subjects. However, intraabdominal abscess developed in two rats (one each in Control and EPO groups). These subjects were excluded from the study.
Biochemical measurement results
Comparative analysis of the three groups did not reveal any significant differences in leukocytes, CRP, and amylase values. The results of the biochemical parameters are presented in table 1.
| WBC (K/mm3) | CRP (mg/L) | Amylase (U/L) | Pancreatic score | |
| Sham | 8.18 ± 0.64 | 0.09 ± 0.01 | 2171.85 ± 106.40 | 0.86 ± 0.26 |
| Control | 8.34 ± 0.67 | 0.12 ± 0.01 | 1990.83 ± 164.50 | 7.33 ± 1.05* |
| EPO | 11.35 ± 1.25 | 0.12 ± 0.02 | 2063.16 ± 272.42 | 3.50 ± 0.42†# |
Table 1: Biochemical and histopathologic evaluations of the pancreatic tissue damage in groups (mean ± SE). WBC: white blood cell, CRP: C-reactive protein. Comparison of the groups *: Sham- Control (p=0.002), †: ontrol-EPO (p=0.023), #: Sham-EPO (p=0.003).
Antioxidant parameter measurements
Mean catalase level was highest in the Sham group and lowest in the Control group (p=0.179). On the other hand, the mean catalase level of the EPO group was slightly lower than that of the Sham group (p=0.442) and higher than that of the Control group (p=0.405). However, the differences were not significant between groups.
The mean GSHrx level was highest in the Sham group. The Control group showed a significant decrease compared to the Sham group (p=0.023). The mean GSHrx level of the EPO group was found to be close to that of the Sham group (p=0.098) and higher than that of the Control group (p=0.292).
These findings indicate that EPO prevents catalase and GSHrx enzyme activity loss in the ileum but not in a significant manner. The mean catalase and GSHrx levels measured in the ileum homogenates are presented in table 2.
| Catalase (nmol/min/mg) |
GSHrx (nmol/min/mg) |
Ileal score | |
| Sham (I) | 6.37 ± 1.27 | 76.28 ± 1.70 | 1.14 ± 0.14 |
| Control (II) | 5.60 ± 1.36 | 73.71 ± 1.97 | 2.33 ± 0.55 |
| EPO (III) | 6.05 ± 0.69 | 74.71 ± 1.38 | 1.33 ± 0.33 |
| P values of the group comparisons | |||
| I vs. II | 0.179 | 0.023 | 0.027 |
| I vs. III | 0.442 | 0.098 | 0.917 |
| II vs. III | 0.405 | 0.292 | 0.04 |
Table 2: Antioxidant capacities (mean ± SD) and histopathologic scores (mean ± SE) of the ileal tissues in groups. GSHrx: glutathione reductase.
Histopathological analysis results
In three subjects of the Sham group, examination of the pancreatic tissue revealed minimal edema and leukocyte infiltration in interacinar regions. However, in general the acinars and the structure of the Langerhans islets were normal in this group. In the Control group, more edema, leukocyte infiltration in the interacinar regions, and necrosis was observed (Figure 1A). The pancreatic tissues of some subjects were found to exhibit more degeneration, necrosis, and fibrin accumulation. In the EPO group edema and leukocyte infiltration persisted. However, these were less in severe than that of the Control group (p=0.023). Necrotic areas were small in number and fibrin accumulation was not observed either (Figure 1B). In the EPO group the acinars and Langerhans islets of the pancreatic tissue of some subjects were of similar structure to those of the Sham group. However, the significant difference between these two groups was obtained (p=0.003). Histopathologic scoring of the pancreas is presented in table 1.
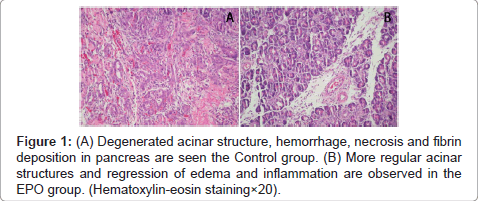
Figure 1: (A) Degenerated acinar structure, hemorrhage, necrosis and fibrin deposition in pancreas are seen the Control group. (B) More regular acinar structures and regression of edema and inflammation are observed in the EPO group. (Hematoxylin-eosin staining×20).
Histopathological examination of the ileum revealed that the ileal structure in the Sham group was normal: edema and shedding of the epithelium and deterioration of the villus and crypt structure were not observed. The deeper layers of the ileum were not damaged. There was a normal amount of inflammatory cells in the lamina propria and submucosa. In contrast, in the control group, generally edema, epithelial shedding at the villus tips and deterioration of the villus and crypt structure were observed in combination with separation from the lamina propria layer (Figure 2A). An increase in inflammatory cells and capillary congestion were found in the lamina propria. In addition, in the intestinal gland epithelium cells, mitotic figures were often seen. Like in the Sham group, no edema and shedding of the epithelium, or degeneration in the villus and crypt structure were found in the EPO group (p=0.917). The tunica submucosa, tunica muscularis, and serosa were intact (Figure 2B). Intestinal gland structure was normal. Ileal damage was found to be considerably less in the EPO group than in the Control group (p=0.04). No necrotic focus in ileum was observed in any of the groups. The histopathologic scoring of the ileum is presented in table 2.
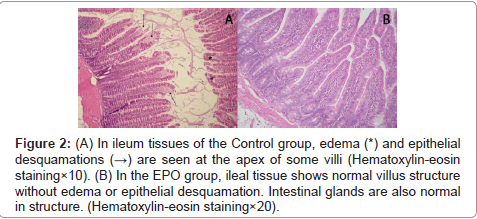
Figure 2: (A) In ileum tissues of the Control group, edema (*) and epithelial desquamations (→) are seen at the apex of some villi (Hematoxylin-eosin staining×10). (B) In the EPO group, ileal tissue shows normal villus structure without edema or epithelial desquamation. Intestinal glands are also normal in structure. (Hematoxylin-eosin staining×20).
The above findings indicate that EPO prevents the decrease in antioxidant capacity of the ileum of subjects with pancreatitis and prevents/minimizes the damage to the pancreas and ileum.
AP leads to local and systemic complications over a wide spectrum. Especially intestinal damage affects the clinical process. Circulatory dysfunction in the splanchnic region causes intestinal ischemia [2]. Inflammatory cells, particularly neutrophils accumulate in this region and increase the release of free oxygen radicals, inflammatory response, and worsen the ischemic effect [2,17]. Damage of the mucosal integrity leads to an increase in intestinal permeability and damage in interstitial Cajal cells and myenteric neurons causes ileus progressing through endotoxemia and bacterial translocation [4,17-19]. Moreover, apparently MMP-9 related changes also occur in the intestinal capillary endothelial barrier [20]. In the intestine, not only the epithelial barrier but also the secretory immune barrier is impaired. Thus, the amount of IgA decreases both in the mucosa and mucus [21,22]. Consequently, all these processes aggravate the severity of the AP and its systemic effects.
In order to reduce endotoxemia and bacterial translocation by preventing or reversing the intestinal barrier damage, various substances have been studied. It is reported that enteral immune nutrition and probiotics reduce endotoxemia, bacterial translocation, apoptosis and histopathological damage of the intestine and that it also increases the IgA concentration in serum and intestinal mucus [21,23]. Blocking the secretion of the neutrophil MMP-9, or preventing the accumulation of neutrophil in the region through different ways also has a regressive effect on bacterial translocation and intestinal damage [18,24]. In addition, PAF inhibitors, NF-κΒ inhibitors, and substances such as dexamethasone with anti-inflammatory effects reduce the blood concentration of the inflammatory cytokines TNF-α, IL-1β, IL-6 and the MPO activity in the intestine [17,24,25].
EPO is a cytokine and hormone with receptors, production, and pleiotropic effects in many organs [6]. EPO, the production of which mostly increases with hypoxia/ischemia, reduces the production of free oxygen radicals, oxidative stress, inflammation and apoptosis. It protects tissues from damage and allows the repair of tissues because of such features as angiogenesis and neuroprotection [6-12]. EPO also improves the immune response by increasing the number of T and B lymphocytes and the amount of immunoglobulin [9]. However, EPO reduces accumulation of neutrophil in tissue; thus, prevents apoptosis and mortality [8].
These effects are also valid for the intestine. It is found that in the case of hemorrhagic shock, EPO reduces bacterial translocation and the endotoxin concentration, prevents intestinal permeability, and limits the intestinal damage [11]. Moreover, it restores the disrupted intestinal microcirculation [12]. The effects of EPO on oxidative stress reduction and protection against the intestinal damage following the intestinal ischemia and reperfusion are considerable [10]. However, its effects may vary in relation to doses administered. The administration of a low dose of EPO in the presence of endotoxemia results in an increase in the concentration of biochemical substances and cytokines. Thus, a low dose of EPO may worsen the pancreatic damage or have only a minimal protective effect [26,27]. In contrast, administration of a high dose of EPO decreases the inflammatory cytokines and the oxidative damage in the pancreas, prevents apoptosis in the intestine as well, and stimulates the proliferation of intestinal muscle cells and enterocytes [28,29].
In this study CRP, amylase levels and leukocytes increased in all groups and did not reveal any significant difference among the groups. We did not try to obtain whether the increases of leucocytes and amylase level are dose dependent effect of EPO or not. However, the increase of the biochemical parameters in all groups was considered to be related to the invasive nature of the pancreatitis model used even in the Sham group [30]. Amylase and lipase levels are useful markers just for the diagnosis of the AP. However, these markers are of limited value for predicting the severity and the course of the AP [31]. Compatible to this knowledge, we found no correlation between the biochemical results and histopathologic scoring of the pancreas in this study. This model causes pancreatitis in a wide range of severity (mild to hemorrhagic and necrotizing forms). Therefore, it has limitation for investigating the course of the pancreatic injury. However, this model is suitable for investigating damage of the other organs and the systemic effects of the pancreatitis [30]. Our primary aim was to investigate the intestinal damage. Pancreatic damage and its discussing are beyond the scope of this study. Our results which obtained the protective effect of EPO in intestinal damage were parallel to the suggestions reported and mentioned above. The results showed that EPO had significantly prevented edema and epithelial shedding in the ileum and degeneration of the villus and crypt structure, and had preserved the structural integrity of the intestinal glands. Moreover, EPO protected the antioxidant capacity of the ileum by slightly preventing catalase and GSHrx enzyme activity loss. Glutathione level is a reliable marker of antioxidant capacity and its high level correlates with EPO usage and less tissue damage [10]. However, the low number of the subjects in the groups and a few parameters assessed could be suggested as limitations of this study.
To conclude, EPO prevents the decrease of the catalase and GSHrx levels as the anti oxidant capacity in the intestine and protects the intestine against damage, which develops secondarily to the AP. However, this issue requires further experimental and clinical studies.