Angiology: Open Access
Open Access
ISSN: 2329-9495
ISSN: 2329-9495
Research Article - (2018) Volume 6, Issue 3
Objective: Atrial fibrillation (AF) is the most common arrhythmia after coronary artery bypass grafting (CABG) surgery. In our study we aimed to evaluate if syntax score and logistic clinical syntax score (log CSS) predict AF after isolated CABG surgery.
Methods: This study was retrospectively designed and included total of 249 patients who underwent CABG at least 1 vessel lesssion between 2011-2013. The exclusion criteria were preoperative AF, emergent CABG operation, severe valvular diseases need operation, congenital heart diseases, severe organ failure and malignancy. The study population was divided into two groups (postoperative (Po) AF (+) group, PoAF(-) group) according to development of AF after CABG. Syntax score and log CSS were calculated in both groups. NCSS (Number Cruncher Statistical System) 2007 Statistical Software (Utah, USA) pocket programme was used.
Results: Retrospectively collected data showed in (PoAF) (+) group diabetes mellitus (DM) (p<0.001), uric acid (5.96 vs. 5.21 p=0.032), neutrophil count (6.11 vs. 5.08 p<0.01), neutrophil lymphocyte ratio (NLR) (3.48 vs. 2.54 p<0.01) were significantly higher than PoAF (-) group. In PoAF (+) group lymphocyte count (1.94 vs. 2.24 p<0.01) and ejection fraction (EF) (50.06 vs. 53.22 p=0.017) were significantly lower than postop AF (-) group. In Postop AF (+) group left anterior descending (LAD) artery-saphenous grafting (11.27% vs. 4.49% p<0.01) and circumflex (Cx) artery-saphenous grafting were significantly higher than PoAF (-) group (p=0.049). In PoAF (+) group, follow-up in intensive care unit (ICU) (days) (p=0.045) and follow-up in hospital (days) were significantly higher than PoAF (-) group (p=0.002). In PoAF (+) group, SYNTAX score (30.69 vs. 28.52 p<0.01) and log CSS were significantly higher than PoAF (-) group (8.34 vs. 6.49 p=0.001).
Conclusion: In our study, high HbA1c, NLR and SYNTAX score were found to be independent predictors of PoAF. But the power of SYNTAX score and log CSS to make a differential diagnosis of PoAF were not high.
Keywords: SYNTAX score; Logistic clinic SYNTAX score; Atrial fibrillation; Post CABG
Atrial fibrillation (AF) is the most common arrhythmia after cardiac surgery. AF without effective atrial construction is characterized with completely irregular atrial depolarization with 350-600 bpm and on Electrocardiogram (ECG) small, irregular and inconstant atrial amplitude and morphology is seen [1]. Atrial fibrillation is seen most frequently in second and third day after the surgery [2,3]. Although improvement in cardiac surgery and myocardial protection techniques, new onset AF incidence after cardiac surgery still doesn’t decrease. Although PoAF has been regarded as a benign, transient and selflimited complication after cardiac surgery, it has been shown to be associated with perioperative myocardial infarction, renal failure, cognitive dysfunction, and infective complications [4-6] systemic embolization, hemodynamic insitability which increase medical costs and hospital stay [7].
SYNTAX score is an angiographic score that determines the complexity of coronary artery disease and used to predict major advanced cardiovascular events after revascularization [8]. The log CSS is a combined risk scoring system, including clinical (age, creatinine clearance, left ventricular ejection fraction [LVEF]) and angiographic parameters (Syntax score), was found superior to the Syntax score in predicting mortality among patients with STEMI in previous studies [9,10]. We hypothesized that coronary lesion complexity may be associated with PoAF. The role of SYNTAX score and log CSS has not been investigated clearly to be a predictor of PoAF. Thus, we evaluated the relationship between SYNTAX score, log CSS and atrial fibrillation in patients undergoing isolated CABG.
Study population
This study was designed as a case-control, single center study. 1850 consecutive patients who were admitted to large volume tertiary training and research hospital with a diagnosis of multivessel coronary disease were evaluated. They subsequently underwent CABG surgery with at least 1 graft between October 2011 and December 2013. The excluison criteria were preoperative AF, emergent CABG operation, severe valvular diseases need operation, congenital heart diseases, severe organ dysfunction such as liver or kidney failure and malignancy. Patients whose preoperative SYNTAX score and log CSS could not be calculated because of insufficient data were excluded. After the exclusion criteria, a total 249 patients were enrolled in the present study. Study population divided into two groups according to the development of new onset AF.
Definitions
The patients provided data on their daily smoking habits. Past smokers were included in the smoker category. Hypertension was defined as systolic arterial pressure exceeded 140 mmHg and/or diastolic arterial pressure exceeded 90 mmHg, or the patient was using antihypertensive drugs [11]. DM was defined as fasting glucose levels exceeded 126 mg/dl or the patient used prescribed glucose-lowering agents [12]. Hyperlipidemia was defined as total serum cholesterol levels greater than 240 mg/dl, low-density lipoprotein (LDL) cholesterol more than 130 mg/dl, or serum triglycerides exceeding 180 mg/dl, or if the patient used lipid-lowering agents [13].
Data collection
Demographic informations and cardiovascular risk factors were obtained after a systematic review of the patients’ hospital records. Verbal and written informed consents were obtained from each study participant and the study protocol was approved by the local ethics committee.
All hematological and biochemical parameters were analyzed before CABG operation. Creatinine clearance was calculated with the creatinine level measured before CABG operation according to the Cockcroft-Gault Eduation.
After surgery a 12-lead ECG was obtained every 12 or 24 hours at intensive care unit and in-patient units, respectively. Atrial fibrilation was described as irregular rhythm with absence of p-waves before each qrs complexes.
The Syntax score was calculated using an online SYNTAX score calculator (defined as 50% or greater stenosis in any coronary vessel with a diameter of 1.5 mm or greater) [14,15]. Log CSS was calculated according to the formula developed by Farooq et al. [9]. All Scores were calculated retrospectively by two cardiologists blind to each other and clinical outcomes. The last preoperative coronary angiogram was used for score calculation.
Baseline echocardiographic examinations were performed with standard commercial ultrasound system (Vivid 3, General Electric Vingmed, Horten, Norway) using 2.5-3.5 MHz multiphase-array probe before the operation. Echocardiographic examinations were performed by a single experienced investigator. Ejection fraction was calculated by the modified Simpson’s method from apical 4- and 2-chamber views.
Surgical technique
The CABG operation was performed using standard surgical techniques. Complete revascularization was performed when possible, using arterial conduits or a reverse saphenous venous graft (SVG). General anesthesia was administered, with monitoring of cardiac rhythm and invasive blood pressure. Then median sternotomy was performed. After harvesting of the left internal mammary artery, the right arterial appendage stump was used for venous cannulation. Cardiopulmonary bypass (CPB) was established via cannulation of the ascending aorta and right atrium with a 2-stage venous cannula and the administration of intravenous heparin to ensure the proper amount of anticoagulation. The body temperature of the patient was sustained at a level of mild hypotermia (a nasopharyngeal body temparatue of approximately 32˚С) and a CPB flow rate of 2.4 L/min/m2 and a blood pressure of >60 mm Hg were maintained. After aortic cross-clamping, antegrade blood cardioplegia was administered through the needle in the aortic root. Then SVG was used to bypass the lesions in the other coronary arteries. In addition, left internal mammary graft was anastomosed to the left anterior descending artery (LAD).
Statistical analysis
In the present study, statistical analysis was performed by using NCSS (Number Cruncher Statistical System) 2007 statistical software (Utah, USA) pocket programme. All data were analyzed descriptive methods (as mean ± SD) and comparison of parametric values between 2 groups was performed by means of an independent samples t test. Comparison of qualitative values Chi 2 test was used. Logistic regression analysis was used to assess the predictors of PoAF. Variables with p values <0.05 by univariate analysis were included in the multivariate logistic regression analysis model and the respective odds ratios (OR) with 95% confidence intervals (CI) were calculated. Receiver Operating Characteristic (ROC) analysis was used to detect the cutoff values of the SYNTAX score and CSS in the prediction of PoAF. All statistical tests were 2-sided and level of significance was set at p<0.05. Intraobserver and interobserver agreements for Syntax score and log CSS were also assessed by Spearman correlation for absolute agreement.
The patients’ demographic, clinical and laboratoary parameters were given in the Table 1. There was no statistically significant difference between PoAF (+) and PoAF (-) groups (p>0.05) according to the age and sex, strikingly DM was statistically higher in PoAF (+) group than PoAF (-) group (61% vs. 35%; p<0.001). Hypertension (HT) and smoking were not found significantly different in two groups (p>0.05). Also in PoAF (+) group, HbA1c (8.28 vs. 6.71 p<0.01) uric acid (5.96 vs. 5.21 p=0.032), neutrophil count (6.11 vs. 5.08 p<0.01), NLR (3.48 vs. 2.54 p<0.01) were found to be statistically higher than the PoAF (-) group. Lymphocyte count was statistically lower in PoAF (+) when compared with PoAF (-) group (1.94 vs. 2.24 p<0.01).
| Postop AF (-) n:178 | Postop AF (+) n:71 | p | |
|---|---|---|---|
| Age, years | 60.94 ± 6.47 | 61.69 ± 8.15 | 0.444 |
| Gender | |||
| Female, n (%) | 36 (20.22%) | 22 (30.99%) | 0.07 |
| Male, n (%) | 142 (79.78%) | 49 (69.01%) | |
| Diabetes mellitus, n (%) | 44 (35.39%) | 63 (61.97%) | 0.0001 |
| Hypertension, n (%) | 97 (54.49%) | 38 (53.52%) | 0.889 |
| Smoking, n | 71 (39.89%) | 33 (46.48%) | 0.341 |
| LVEF, % | 53.22 ± 9.01 | 50.06 ± 10.3 | 0.017 |
| Total cholesterol, mg/dl | 199.94 ± 54.03 | 205.24 ± 47.97 | 0.472 |
| HDL, mg/dl | 39.28 ± 12.15 | 38.24 ± 10.35 | 0.528 |
| LDL, mg/dl | 129.85 ± 43.57 | 133.54 ± 40.5 | 0.540 |
| Triglicerids, mg/dl | 187.6 ± 107.55 | 223.06 ± 196.73 | 0.07 |
| Glucose mg/dl | 128.61 ± 47.02 | 165.25 ± 77.37 | 0.0001 |
| HbA1c, % | 6.71 ± 1.67 | 8.28 ± 6.1 | 0.002 |
| Uric acid, mg/dl | 5.25 ± 1.71 | 5.96 ± 1.88 | 0.032 |
| Creatinin, mg/dl | 1.16 ± 1.54 | 1.95 ± 3.27 | 0.341 |
| GFR mL/min | 92.92 ± 29.52 | 86.65 ± 30.07 | 0.133 |
| Leucocyte K/µl | 8.76 ± 2.56 | 9.1 ± 2.93 | 0.366 |
| Hemoglobin g/dl | 15.53 ± 26.55 | 13.55 ± 1.53 | 0.536 |
| Platelets, 103/mm3 | 248.46 ± 69.2 | 246.01 ± 67.25 | 0.802 |
| Neutrophil K/µl | 5.08 ± 1.32 | 6.11 ± 2.27 | 0.0001 |
| Lymphocyte % | 2.20 ± 6.63 | 1.94 ± 0.52 | 0.002 |
| NLR % | 2.54 ± 1.18 | 3.48 ± 1.50 | 0.0001 |
| Previous MI, n (%) | 78 (43.82%) | 32 (45.07%) | 0.858 |
| Previous PCI, n (%) | 60 (33.71%) | 31 (43.66%) | 0.141 |
| LAD Lima, n | 174 (97.75%) | 69 (97.18%) | 0.791 |
| LAD Saphenous, n | 8 (4.49%) | 8 (11.27%) | 0.049 |
| D1 Saphenous, n | 89 (50.00%) | 32 (45.07%) | 0.482 |
| IM Saphenous, n | 19 (10.67%) | 7 (9.86%) | 0.849 |
| CX Saphenous, n | 44 (24.72%) | 11 (15.49%) | 0.113 |
| CXOM Saphenous, n | 107 (60.11%) | 47 (66.20%) | 0.372 |
| RCA Saphenous, n | 96 (53.93%) | 33 (46.48%) | 0.288 |
| RCA PDA, n | 39 (21.91%) | 17 (23.94%) | 0.729 |
| RCA Pl, n | 5 (2.81%) | 3 (4.23%) | 0.567 |
| Grafts per patient, n | 3.25 ± 0.81 | 3.2 ± 0.79 | 0.622 |
| SYNTAX score | 28.52 ± 5.62 | 30.69 ± 6.28 | 0.008 |
| Log CSS | 6.49 ± 3.75 | 8.34 ± 4.39 | 0.001 |
| Follow-up in ICU, days | 1.12 ± 0.66 | 1.18 ± 0.76 | 0.540 |
| Follow-up in hospital, days | 8.63 ± 3.85 | 9.61 ± 5.86 | 0.124 |
EF: Ejection Fraction, HDL: High Density Lipoprotein, LDL: Low Density Lipoprotein, GFR: Glomerular Filtration Rate, NLR: Neutrophil/Leynfocyte Ratio, LAD: Left Anterior Descending, IM: Intermediar ,CX: Circumflex, RCA: Right Coronary Artery, ICU: Intensive Care Unit
Table 1: Baseline demographic, clinical and laboratory characteristics of the study groups.
There was no statistically significant differences between two groups according to totalcholesterol, LDL, HDL, TG, creatinine, GFR, leucocyte, hemoglobin, platelet count (p>0.05). Ejection Fraction (EF) of PoAF (+) group was statistically lower than PoAF (-) group (50.06 vs. 53.22 p=0.017)
In PoAF (+) group LAD-saphenous anostomosis (11.27% vs. 4.49%, p<0.01) and CX-saphenous anostomosis were statistically higher than PoAF (-) group (p=0.049). Other hand, previous myocardial infarction (MI), previous percutaneous coronary intervention (PCI), LAD-LIMA, DL-saphenos, IM-saphenous, CXOM-saphenous, RCA-saphenous, RCA PDA, RCA PL and number of graft were not statistically different between two groups (p>0.05) Follow-up in intensive care unit (p=0.045) and in hospital (day) (p=0.002) in PoAF (+) group were significantly higher than PoAF(-) group.
SYNTAX score (30.69 vs. 28.52, p<0.01) and CSS (8.34 vs. 6.49, p=0.001) were found statistically higher in PoAF (+) group than PoAF (-) group.
DM, HbA1c, uric acid, NLR, LAD-saphenous, SYNTAX score, CSS variables were evaluated by logistic regression analysis to find out the independent predictors of AF after CABG (Table 2). High HbA1c (OR: 1.41; 95%:1.11-1.77; p=0.04), NLR (OR:1.54; 95%Cl:1.12-2.12; p=0.008) and SYNTAX score (OR:1.07; 95%Cl:1.00-1.14; p=0.047) were found as independent predictors.
| OR %95 GA | ||||||
|---|---|---|---|---|---|---|
| B | S.E. | p | OR | Low | High | |
| DM | 0.01 | 0.50 | 0.983 | 1.01 | 0.38 | 2.70 |
| HbA1c | 0.34 | 0.12 | 0.004 | 1.41 | 1.11 | 1.77 |
| Uric Acid | 0.23 | 0.13 | 0.064 | 1.26 | 0.99 | 1.61 |
| NLR | 0.43 | 0.16 | 0.008 | 1.54 | 1.12 | 2.12 |
| LAD Safhenous | -1.31 | 0.89 | 0.142 | 0.27 | 0.05 | 1.55 |
| SYNTAX Score | 0.07 | 0.03 | 0.047 | 1.07 | 1.00 | 1.14 |
| Clinical SYNTAX Score | -0.05 | 0.06 | 0.384 | 0.95 | 0.85 | 1.07 |
Table 2: Multivariate Regression Analysis for evaluation of the independent predictors of PoAF.
In the ROC analysis, for Syntax score area under curve (AUC) was 0.586 for predicting PoAF after CABG (SE: 0.041; 95% CI: 0.522– 0.648), for log CSS AUC was 0.596 (SE: 0.041; 95% CI: 0.532–0.657). The power of both SYNTAX score and log CSS to make a differential diagnosis of PoAF were not high (Table 3 and Figure 1).
| AUC | SE | 95% | CI | |
|---|---|---|---|---|
| SYNTAX Score | 0.586 | 0.041 | 0.522 | - 0.648 |
| Clinical SYNTAX Score | 0.596 | 0.041 | 0.532 | - 0.657 |
Table 3: SYNTAX score and log CSS.
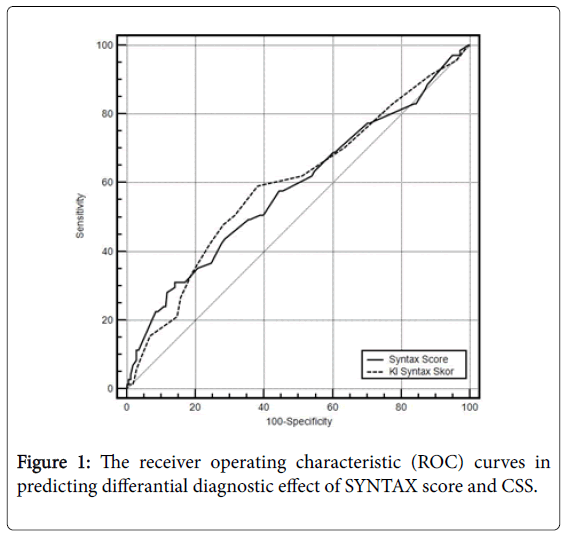
Figure 1: The receiver operating characteristic (ROC) curves in predicting differantial diagnostic effect of SYNTAX score and CSS.
Spearman correlation of intraobserver and inter-observer agreements for Syntax score were 0.956 (P<0.001) and 0.933 (P<0.001), respectively; for log CSS were 0.974 (P<0.001) and 0.980 (P<0.001), respectively.
Main findings of our study;
• Syntax score was an independent predictor of PoAF.
• Additionally HbA1c and NLR were significant independent predictors for our study population.
• Log CSS was not an independent predictor for PoAF.
Post-operative AF was a frequent complication developing after cardiovascular surgery [2,3,16,17]. PoAF can limit itself generally, but it can cause systemic embolization and hemodynamic instability and increase in hospital stay and medical cost [2,3,7,18].
Several PoAF predicting factors have been found such as anatomy of heart (left or right atrial enlargement), functional conduction disturbances, excitability of atrium or ventricule, age, sex, beta-blocker usage prior the operation, sterile inflammation on the atrium wall due to surgical trauma, multiple coronary artery stenosis, sinoatrial or atrioventricular nodal artery disease, number of distal anostomouses, previous MI and PCI, post-operative increase in creatinine –urea levels [3,19,20], fragmented QRS [21], p wave duration [22].
PoAF insidence in the literature is 20-40% [17], in this study 28% of our patients developed PoAF, similar to literature. PoAF can be seen early or late but the average days are 2 and 4 days after the surgery [23]. In our study PoAF was detected between 0 day and 6 day, average day was 2.22 ± 1.16 (Figure 2).
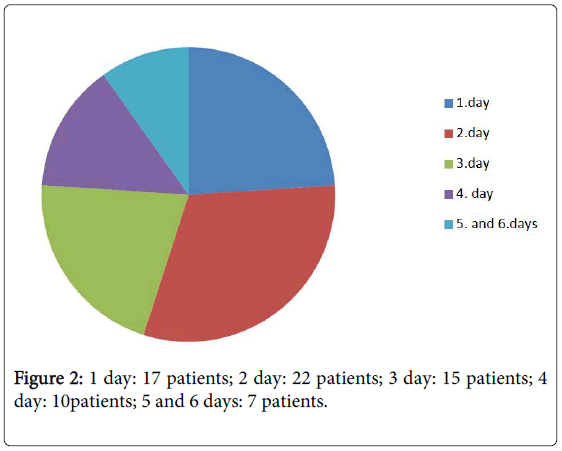
Figure 2: 1 day: 17 patients; 2 day: 22 patients; 3 day: 15 patients; 4 day: 10patients; 5 and 6 days: 7 patients.
Advanced age has been shown to be a strong predictor of PoAF in many studies. It was explained by atrial dilatation, atrophy, conduction disturbances and fibrosis [23]. In the present study, we found that in PoAF (+) group patients’ ages were higher than PoAF (-) group similar with literature.
In literature previous MI or PCI’s effects on PoAF development are controversial. Previous MI may lead ischemia of the myocardial tissue, that’s why we thought that prevıous PCI could be a predictor of PoAF but there was no statistically differences between groups.
DM with inflammatory pattern can affect PoAF development by directly or indirectly with microangiopathy and neuropathy. In our study, in PoAF (+) group there were 63(61.97%) patients with DM, in PoAF (-) group there were 44(35.39%) patients with DM. DM was found statistically higher in PoAF (+) group but it was not an independent predictor.
NLR is an inflammatory marker which has been shown to be a strong predictor of AF after CABG [24]. It can be explained by neutrophils participate in perioperative myocardial damage and are associated with increased blood viscosity and hypercoagulability [25]. Lymphopaenia may indicate that the immune response is suppressed and this condition has been associated with adverse cardiac outcomes. Reduction of lymphocytes has reflected elevation of serum catecholamines and cortisol levels formed during a systemic stress response [25]. An elevated NLR is an independent predictor of nonvalvular AF [25,26] which is consistent with our results.
SYNTAX score determines the complexity of coronary artery disease and help us to predict major advanced cardiovascular events after revascularization. SYNTAX score has been shown at the same time prediction of both short and long term major adverse events after revascularizaton. Till now SYNTAX score and PoAF association data is limited. In the present study we showed that SYNTAX score is an independent predictor for PoAF, but log CSS is not found as an independent predictor.
The log CSS, a combined risk score, was developed by Farooq et al. [9] and includes patient’s clinical (age, LVEF and creatinine clearance) and anatomical (SYNTAX score) parameters. Log CSS score was first used to predict the 1-year cardiovascular mortality after PCI procedures and it was found to be better than the SYNTAX score for this purpose [10]. Later in a different study, log CSS was also found to enhance risk stratification for 3-year mortality after PCI compared with the SYNTAX score [27]. In our study, log CSS was not found as an independent predictor and not powerful to make differential diagnosis of PoAF.
The main limitations of this study were relatively small sample size and contrary to cohort study with its observational and retrospective nature. The method of the determining of AF, based on clinical documentation with ECG findings, likely underestimated the actual number of incident asympthomatic or paroxysmal AF. The other limitation was long term clinical course of the patients was not recorded, late AF occurrence cannot be followed. The present study mainly focused on the preoperative and postoperative data for predicting AF, but surgical procedures and anesthetic drugs may play a role in the development of AF.
In our study high HbA1c, NLR and SYNTAX score were found to be independent predictors of PoAF. SYNTAX score and CSS were not found as strong factors for making differential diagnosis of PoAF.