Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2014) Volume 4, Issue 6
Objectives: To determine if there is an association between overall and breast cancer specific-survival and participation in clinical trials (CT’s) in patients with invasive non-metastatic breast cancer.
Materials and Methods: All women (6,794) diagnosed between 1982 and 2008 with invasive non-metastatic breast cancer from our database were used. Survival data was compared between women diagnosed with invasive nonmetastatic breast cancer who participated in a CT and with those who did not.
Results: A total of 1,137 (16.7%) patients participated in a CT. These patients were younger and exhibited more unfavourable prognostic factors compared to non-participant. The crude hazard ratio for the overall survival rate for those who participated in a CT was 0.84 (95% CI [0.73-0.97]; p=0.02), and was 0.90 (CI 95% [0.78-1.04]; p=0.16) after an adjustment for body mass index (BMI), hormone receptors, treatments and histological grade.
Conclusion: Breast cancer patients who participate in a CT exhibit different baseline characteristics. Assuming that difference, trial participation in itself did not improve survival rate in breast cancer patients. However, it can be concluded that the CTs does not have a deleterious effect on the participants.
Keywords: Breast Cancer, Survival, Clinical Trial, Participation, Trial effect
Clinical trials (CTs) are essential for the evaluation of new interventions and therapies prior to their routine use in clinical practice [1,2]. However, less than 10% of cancer patients participate in CTs [3]. Between 1990 and 2011, breast cancer mortality in Canada dropped from 31.3/100,000 to 20.7/100,000 (adjusted for age) [4], and the following hypotheses may explain this decrease: large-scale screening for early-stage cancer [1], more aggressive adjuvant therapies [2,5] and more effective treatments of metastatic diseases [6]. These hypotheses have one common feature: the interventions have been studied and proven to be more effective than previous standards in CTs.
The possible benefits of participating in a CT are: a potentially better treatment under study, follow-ups at a cancer center, contributing to research so that future patients can benefit from the results and a survival benefit [7-9]. This potential survival benefit may be due to the fact that the treatment under study might be superior to the standard treatment. However [10], this occurs in less than a third of phase III trials [11,12]. Braunholtz et al., [13] attempted to explain this possible survival benefit associated with the participation in a CT (“trial effect”) with the following hypotheses. First is the treatment effect, where the new intervention proves to be more effective than standard treatments. The second is theprotocol effect, where intervention processes and procedures are thoroughly described, and where participants and doctors are required to adhere to them: dose adjustments or the use of growth factors to maximise the dose-intensity of chemotherapy is a good example of this effect. Third is the care effect, defined by additional follow-up visits which increase patients’ surveillance by nurses for earlier detection of side effects or disease recurrence. Fourth is the Hawthorne effect, regarding changes in patient behaviours’ when participating in a CT. CT patients who feel observed might exhibit different behaviours’ than non-CT patients. For example, they may be more compliant to oral anticancer therapy. Finally, the placebo effect influences the patient to think that he received the real treatment. He is psychologically conditioned and feels the effects of the treatments under study when the placebo treatment is inert. There is also the question about the efficacy and effectiveness that provide an incomplete picture of the usefulness of a given treatment in daily practice (14). Efficacy relates to whether or not an intervention can work under ideal conditions and effectiveness relates to the pragmatic question whether an intervention works in routine clinical care [14].
There is currently no conclusive evidence indicating that the participation in a CT for breast cancer patients is associated with a benefit in survival rate (trial effect) - even in negative trials. The last twenty years have seen five literature reviews on outcomes differences in CT versus non-CT patients [13,15-19]. Two of these reviews [15,18] dealt exclusively with cancer patients, whereas other medical fields were included in the other three (however, the majority dealt with oncology) [13,16,17]. These reviews observed little scientific evidence to support the assumption that simply being a participant in a CT was clinically beneficial to patients.
The goal of the present study was to determine if there is an association between overall and breast cancer specific-survival and participation in a CT in patients with invasive non-metastatic breast cancer.
Study population
Patients were from the Centre des maladies du sein (CMS) Deschênes-Fabia du CHU de Québec, a tertiary breast cancer center and one of the largest in Canada. The Province of Quebec has a universal health care system. There were a total of 6,794 women diagnosed with invasive non-metastatic breast cancer between January 1st 1982 and April 31st, 2008 in the CMS database. All women with newly diagnosed breast cancer treated in that center were recorded in the CMS database. Women were excluded if they had a previous diagnosis of cancer (any site). Data on survival, cause of death and comorbidity were obtained through linkage with the Province of Quebec administrative registries. The study was approved by the research ethics board.
Data collection
Data on patients’ demographic, tumor and treatment characteristics were available from the CMS database. The date of diagnosis represents the entry to the cohort for the purpose of our analysis. Information about participation in a CT was collected from CT research charts. For information about CTs, the protocol was used and the data collected contained the following: phases (I, II, III, IV), start and end dates and treatment arms classified into standard, experimental or unknown. CTs in the metastatic setting were excluded in the analysis due to the absence of information in the CMS database on eligibility of patients once metastatic disease developed. A total of 1,137 patients participated in 51 adjuvant, neo-adjuvant, surgical or supportive CTs (Table 1). For each participant, the following information was collected: date of entry in the CT, arm (standard, experimental, unknown), medication or intervention and the type of intervention of the CT. The definitions of these types of interventions are described below.
| Clinical trial name | N | Intervention | Type | |
|---|---|---|---|---|
| Standard arm | Experimental arm | |||
| NSABP B-14 | 177 | No TAM | TAM | Adjuvant |
| NSABP B-11 | 5 | L-PAM+5FU | L-PAM+5FU+A | |
| NSABP B-12 | 7 | L-PAM+5FU+TAM | L-PAM+5FU+TAM+A | |
| NSABP B-15 | 16 | CMF | AC vs. AC follow by CMF | |
| NSABP B-16 | 3 | TAM | AC--TAM vs. L-Pam+5FU--TAM | |
| NSABP B-13 | 10 | No chemo. | Chemo. (MF) | |
| NCIC CTG MA.4 | 15 | TAM | TAM+chemo | |
| NSABP B-19 | 12 | CMF | MF | |
| NSABP B-20 | 39 | TAM | Chemo+TAM | |
| NSABP B-18 | 28 | AC post-surgical | AC pre-surgical | |
| NSABP B-22 | 18 | AC x4 | AC intensified vs. AC intensified+ ↑ total dose | |
| NCIC CTG MA.5 | 2 | CMF | FEC | |
| NSABP B-21 | 10 | Radiation only | TAM only TAM+Radiation | |
| NSABP B-23 | 3 | CMF+placebo | CMF+TAM/AC+placebo vs. AC+TAM | |
| NSABP B-25 | 18 | A 60 mg/m2×4 C 1200 mg/m2×4 | A 60 mg/m2×4 C 2400 mg/m2×2 vs. A 60 mg/m2×4+C 2400 mg/m2×4 | |
| NCIC CTG MA.12 | 31 | Standard | TAM | |
| NSABP B-28 | 12 | AC | AC--taxol | |
| NSABP B-27 | 26 | AC-- surgical | AC--docetaxel-- surgical vs. AC-- surgical--docetaxel | |
| NCIC CTG MA.14 | 4 | TAM | TAM+octreotide | |
| ATAC | 55 | TAM | Ana vs. Ana+TAM | |
| TAX 316 | 19 | FAC | TAC | |
| NCIC CTG MA.17 | 13 | Standard | Letrozole | |
| NSABP B-29 | 5 | Control | Octreotide | |
| NSABP B-30 | 69 | AC--TAXOTERE | TAC vs. AT | |
| BCIRG005 | 42 | AC--TAXOTERE | TAC | |
| NCIC CTG MA.20 | 25 | Breast radiation | Breast radiation+armpit | |
| BCIRG006 | 12 | AC--TAXOTERE | AC--TH vs. TCH | |
| HERA | 1 | Control | Trastuzumab | |
| NSABP B-36 | 58 | AC | FEC | |
| NSABP B-31 | 4 | Control | Trastuzumab | |
| SABRE | 3 | Control | Risedronate | |
| NSABP B-38 | 56 | TAC et DD AC--P | AC--PG | |
| NCIC CTG MA.27 | 3 | Anastrozole | Exemestane | |
| HALT | 1 | Placebo | AMG162 | |
| NSABP B-39 | 91 | Standard radiation | Partial radiation | |
| RAPID | 10 | Total radiation | Partial radiation | |
| FACE | 36 | Anastrozole | Letrozole | |
| NSABP B-37 | 1 | Standard | Standard + chemo. | |
| TEACH | 3 | Placebo | Lapatinib | |
| NSABP B-42 | 10 | Placebo | Letrozole | |
| PROACT | 3 | TAM | Ana | Neo-adjuvant |
| CDC 1590 | 1 | TAM | Droloxifen | |
| TAX-301 | 5 | CVAP | CVAP--docetaxel | |
| MA-22e | 4 | None | Epirubicin vs. Docetaxel vs. Pegfilgrastim | |
| 517/280 | 8 | Control | Ondansetron | Support |
| 517/320b | 57 | Control | Ondansetron | |
| EPO-CAN-17 | 8 | Control | EPO | |
| NKV102549 | 2 | Dexamethasone+Ondansetron | Casopitant+Dexamethasone+ ndansetron | |
| NSABP B-06 | 14 | Mastectomy | SBS+Radiation vs. CSS only | Surgical |
| NSABP B-32 | 168 | Sentinel+ALND | Sentinel+ALND if sentinel positive | |
Table 1: Characteristics of opened CTs during study (1982-2008).
Adjuvant: Patients eligible for this type of CT had previously undergone surgery to remove the breast tumor.
Neo-adjuvant: This type of CT is offered to patients who receive systemic therapy before the surgery; it might be used for locally advanced breast cancer or early breast cancer with more aggressive characteristics.
Supportive: CTs studied intervention to decrease side effects (e.g. anti-nausea drugs).
Surgical: Surgical CTs involve surgical intervention and the comparison of surgical techniques. Women were attributed to the CT group from the date of the first randomization. Before that time, or for women never randomized in a CT, they were attributed to the non-CT group from the date of the diagnosis. This method allowed adjustment for the immortal time bias (19). The exposition to a CT began from the first randomization in the event of participation in multiple CTs. A woman who participated in a CT for metastatic disease was excluded from the CT group. If she previously participated in another CT category (i.e. adjuvant CT) then she was included in the CT group.
All analyses were conducted using SAS 9.2 (SAS Institute, Cary, NY, USA). The statistical significance level was set to 5% and a confidence interval (CI) of 95%.
Survival rates for CT and non-CT patients were calculated using the Kaplan-Meier (KM) method. Multivariate Cox proportional hazard models with time-dependent CT indicators were used to account for possible differences between both groups and to determine if a change in survival rate could be attributed to confounding prognostic factors. To estimate HRs and confidence intervals (CIs), all Cox regressions were adjusted for ages (≤49, 50-59, 60-69, ≥70 years old) and stages (I, II, III, unknown) by a different approach using the STRATA option in SAS. The process fits separate models for each level of treatment under the constraint that the coefficients are equal but that the baseline hazard functions are not equal. The following adjustment variables were used: body mass index (BMI) (≤ 24.9, 25.0-29.9, ≥ 30) (hormone receptors status (ER+ or PR+, ER- and PR-, unknown), histologic grades (well differentiated, moderately differentiated, poorly differentiated, unknown), adjuvant systemic therapies (none, chemotherapy only, hormone therapy only, chemotherapy and hormone therapy, unknown), lymphovascular invasion (yes, no, unknown) and Charlson comorbidity index (0, ≥ 1, unknown).
Four Cox proportional hazard models were performed. All models were adjusted for age and stage. Models 1 and 2 were constructed based on the entire study population including a non-CT group of 5,657 women and a CT-group of 1,137 women. Model 2 provides a HR adjusted for hormone receptors, histological grade and adjuvant systemic therapies. Models 3 and 4 were restricted to the patients for whom the comorbidity index was available (n=6,063). All women for whom the comorbidity variable was not available in the hospital records prior to April 1987 were excluded (n=731) from model 3 and 4 analyses. Model 4 is adjusted for comorbidity index, hormone receptors, histologic grade, lymphovascular invasion and adjuvant systemic therapies. The lymphovascular invasion variable was added only in model 4 because missing values were high before 1987.
We also conducted exploratory analyses using three different time period (1982-1990, 1991-1999, 2000-2008) and limited to the category of intervention (adjuvant and neo-adjuvant, given that we did not expect a survival benefits in trials of supportive or surgical interventions).
Patient characteristics
Figure 1 show the flow chart of the selection process of patients who participated to at least one CT between January 1st 1982 and April 31st 2008. Table 2 shows the population characteristics at diagnosis among CT and non-CT patients. A total of 6,794 women were diagnosed with invasive non-metastatic breast cancer between 1982 and 2008 at the CMS. During this period, 1,137 (16.7%) women participated in one or more CTs and were eligible for our analysis. The 1,137 who participated where distributed as follow in the intervention categories: 873 (12.8%) in the adjuvant, 10 (0.1%) in the neoadjuvant, 182 (2.7%) in the surgical and 72 (1.1%) in the support interventions. The median interval between diagnosis and entry into a CT, for those who participated, was 36 days. The median follow-up duration for all women was 6.1 years.
| Participation in a CT | P value | ||
|---|---|---|---|
| No n=5,657 | Yes n=1,137 | ||
| Mean age (years) at diagnosis ±SD* | 58.0 ± 12.8 | 51 ± 10.3 | <0.0001 |
| % | % | ||
| Stagea I II III Unknown |
44.6 40.2 13.7 1.5 |
33.5 49.8 16.2 0.5 |
<0.0001 |
| BMI ≤ 24.9 25.0-29.9 ≥ 30 Unknown |
53.6 28.0 12.6 5.8 |
58.0 27.5 11.8 2.7 |
<0.0001 |
| Lymphovascular invasion Yes No Unknown |
19.7 68.5 11.8 |
25.9 61.3 12.8 |
<0.0001 |
| Histological grade Well differentiated (I/III) Moderately differentiated (II/III) Poorly differentiated (III/III) Unknown |
21,6 27,1 30,5 20,8 |
16,9 26,7 35,8 20,6 |
<0,0001 |
| Hormone receptors Positive (ER+ or PR+)b Negative (ER- and PR-) Unknown |
76.0 17.0 7.0 |
82.3 15.2 2.5 |
<0.0001 |
| Comorbidity 0 ≥ 1 Unknown |
80.6 6.8 12.6 |
82.8 3.2 14.0 |
<0.0001 |
| HER2 status Positive Negative Unknown |
5.2 30.6 64.3 |
7.0 37.2 55.8 |
<0.0001 |
| Breast surgery None Breast conserving surgery Total mastectomy |
2,1 66,7 31,2 |
0,4 69,0 30,6 |
0.0005 |
| Axillary surgery None Sentinel node only Node dissection |
12.0 20.1 67.9 |
1.0 18.0 81.0 |
<0.0001 |
| Adjuvant radiotherapy Yes No Unknown |
68.3 30.8 0.9 |
74.0 25.8 0.2 |
<0.0001 |
| Systemic therapy None Chemotherapy only Hormone therapy only Combination of both therapies Unknown |
24.7 16.3 37.5 19.8 1.7 |
10.5 23.1 25.9 39.4 1.1 |
<0.0001 |
Table 2: Baseline characteristics.
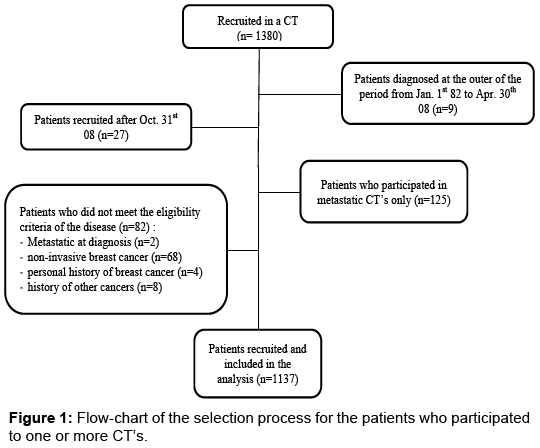
Figure 1: Flow-chart of the selection process for the patients who participated to one or more CT’s.
Each characteristic was significantly different between the CT and non-CT patients. In fact, women who participated in a CT were younger (51 years old ± 10.3) than those who did not (58 years old ± 12.8 years). As for prognostic factors, 49.8% of CT patients had stage II cancer and 16.2% had stage III cancer compared with 40.2% and 13.7%, respectively in the non-CT group. A higher proportion of CT patients showed poorly differentiated histological grade (35.8% vs. 30.5%) and demonstrated lymphovascular invasion (25.9% vs. 19.7%). Status was hormone receptors positive in the majority of women under CT (82.3% vs. 76.0%). HER2 status was positive for a higher proportion in the CT group (7.0% vs. 5.2%) A larger number of CT patients received combinations of adjuvant systemic chemotherapies and hormone therapies versus the non-CT group (39.4% vs. 19.8%). Radiotherapy was administered to a higher proportion of patients the CT group (74% vs. 68.3%).
Overall survival
Figure 2 shows Kaplan-Meier curves for overall survival rate in CT versus non-CT patients. The overall survival curve was higher for women participating in a CT compared to non-CT women (p<0.0001). Overall survival rate for CT patients was 88%, 79%, 70% and 62% at 5, 10, 15 and 20 years, respectively. As for non-CT patients, survival rates were 84%, 71%, 59% and 49% at 5, 10, 15 and 20 years, respectively. Table 3 shows that the crude HR for survival in women who participated in CTs was 0.84 in model 1 (CI 95% [0.73-0.97]; p=0.02). However, adjusted HR (model 2) for overall survival was 0.91 (CI 95% [0.79-1.05]; p=0.19). Models 3 and 4 were restricted to the patients for whom the comorbidity index was available (n=6,063). The results are sensibly the same as models 1 and 2 but with less power.
| Model 1a | Model 2b | Model 3c | Model 4d | |||||
|---|---|---|---|---|---|---|---|---|
| All-Cause | Specific | All-Cause | Specific | All-Cause | Specific | All-Cause | Specific | |
| HR | 0.84 | 0.88 | 0.91 | 0.93 | 0.89 | 0.89 | 0.95 | 0.93 |
| CI (95%) | 0.73-0.97 | 0.75-1.03 | 0.79-1.05 | 0.80-1.10 | 0.75-1.05 | 0.74-1.07 | 0.80-1.13 | 0.77-1.12 |
| P value | 0.02 | 0.12 | 0.19 | 0.40 | 0.15 | 0.22 | 0.56 | 0.44 |
Table 3: Cox proportional hazard models* for all-cause survival and specific breast cancer survival.
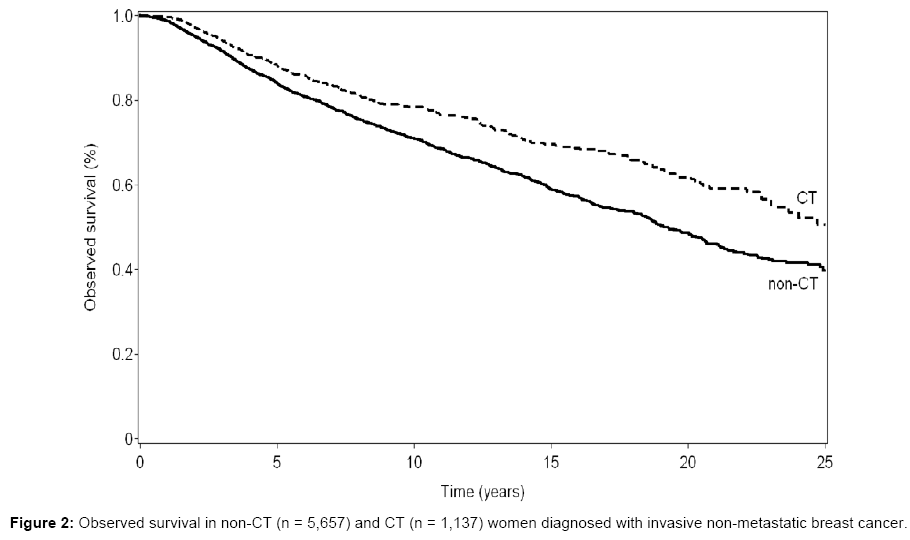
Figure 2: Observed survival in non-CT (n = 5,657) and CT (n = 1,137) women diagnosed with invasive non-metastatic breast cancer.
Specific survival
During follow-up, there were 1,106 deaths due to breast cancer in the cohort study. In CT patients, there were 193 deaths specifically related to breast cancer. Using Cox proportional hazard models, no association was observed for cancer-specific survival in women who participated in CT compared to those who did not (Table 3). The HR for specific survival in women who participated in CT was 0.88 in model 1 (CI 95% [0.75-1.03]; p=0.12) and 0.93 (CI 95% [0.80-1.10]; p=0.4) in model 2.
Exploratory analysis by time period and CT category
In the exploratory analyses according to the time period (Table 4), there was a trend for a benefit of participating in CT in the more advanced period (2000-2008). The interactions tests were statistically significant in the sensitivity analysis for the diagnosis period. When adjusted for age, stage, hormone receptors and adjuvant systemic therapies, HR for overall survival was 0.66 (p=0.02) in the 2000-2008 period.
| 1982-1990 | 1991-1999 | 2000-2008 | ||||
|---|---|---|---|---|---|---|
| All-Cause | Specific | All-Cause | Specific | All-Cause | Specific | |
| HR | 0.87 | 0.87 | 1.04 | 1.13 | 0.66 | 0.54 |
| CI (95%) | 0.71-1.07 | 0.67-1.10 | 0.83-1.30 | 0.88-1.44 | 0.46-0.95 | 0.36-0.83 |
| P value | 0.19 | 0.24 | 0.74 | 0.35 | 0.02 | 0.005 |
Table 4: Cox proportional hazard models for all-cause survival and specific breast cancer survival by period of diagnosis*
In the second exploratory analysis, analyses were restricted to adjuvant and neo-adjuvant CTs. The crude HR for all-causes survival in women who participated in adjuvant and neo-adjuvant CTs was 0.73 (CI 95% [0.63-0.85]; p=0.0001) and the adjusted was 0.94 (CI 95% [0.78-1.13]; p=0.52) (Table 5).
| All-cause survival | Specific breast cancer survival | |||
|---|---|---|---|---|
| Crude HR | Adjusted HR* | Crude HR | Adjusted HR* | |
| HR | 0.73 | 0.94 | 1.01 | 0.98 |
| CI (95%) | 0.63-0.85 | 0.78-1.13 | 0.86-1.19 | 0.79-1.20 |
| P value | 0.0001 | 0.52 | 0.90 | 0.82 |
Table 5: Exploratory analyses restricted to adjuvant and neo-adjuvant CT’s.
Characteristics of CT versus non-CT patients varied from patient, tumor and treatment characteristics, reflecting that CT are available for specific populations, and a tendency for clinicians to offer a trial to patients with a more aggressive disease. The largest number of participants was observed in adjuvant CT. A tendency for better survival among women participating in a CT compared with non- CT patients was observed in the analysis adjusted for age and stage only, but it became non-statistically significant once the analyses were adjusted for patient mix. The breast cancer-specific survival analysis did not show statistically significant results on an eventual CT protective effect in patients with non-metastatic breast cancer. However, because modalities of treatment have changed dramatically in this long period of time the exploratory analysis shows that CT’s were protective in the recent period. In our center specifically, participation in a CT may not increase quality of follow-up nor survival because all patients treated at our center are treated by a team of physicians and professionals with expertise in breast cancer and who are aware of most of the up-to-date information in breast cancer [20].
Few studies on breast cancer women measured the difference in survival rate of patients who participated in CT compared to those who did not. Schwentner et al., [21] analyzed the association between patients who received adjuvant treatment according to the guidelines and those who participated in adjuvants CT in 9,433 patients with breast cancer in an observational retrospective study. Between 1992 and 2008, they observed an adjusted non-significant trend for better overall survival in CT versus non-CT patients (HR=0.87 CI 95% [0.72-1.05]; p=0.15). Moreover, CT patients were significantly younger, as in our study. Different authors explored CTs’ effects on various health issues, including the survival rate. In a meta-analysis, Djulbegovic [10] shows that new treatments are associated with a 5% or 10% improvement in relative survival or primary outcomes. Robinson et al., [22] observed the effect of CT participation on the survival of ovarian cancer patients. Survival analysis revealed, higher overall survival rates for CT (n=53) compared with non-CT patients (n=105). However, unlike our study, CT and non-CT patients shared similar characteristics in terms of age, histological grade, surgical treatments and chemotherapy. Rajappa et al. [23] evaluated the survival of all causes in a cohort of patients with small lung cancer cells. They compared patients who received chemotherapy in CT versus those not on CT who received the treatment according to the guidelines. At two years of follow-up, there was a higher but not significant overall survival in CT patients compared with non-CT patients (14.8% vs. 7.8%, p=0.17). Finally, Hébert-Croteau et al., [24] demonstrated a more favorable survival rate for CT patients in a population-based study of breast cancer patients in the province of Quebec; for women who participated in a CT, the adjusted hazard ratio (HR) for all-cause death was 0.45 (p=0.001), compared with women who did not participate in a CT and not treated according to guidelines (reference group). Among non-CT patient treated according to guidelines, the HR for all-cause of death was lower (0.70, p=0.006).
Furthermore, since the observed adjusted HR are non-significant, our study findings are consistent with those of other literature reviews [13,15,17] that suggest no conclusive evidence of a direct correlation between the participation in a CT and an associated “trial effect”. In our study, CT patients’ characteristics vary greatly compared to those of non-CT patients [13,15,17,23,25]. Literature reveals that CTs are offered to younger patients [26-28], and our study confirms those findings. A selection bias may be related to the types of CTs in the open cohort period who favoured younger patients with hormone receptor positive. Also, physicians may be more inclined to offer participation to younger patients. As we adjusted for age and treatment, the impact on the results should be negligible. To assess whether the type of CT had such an impact on survival and to avoid potential selection bias caused by the selection of trials, we conducted exploratory analyses excluding supportive and surgical CT’s. Data showed no difference between allcause and specific survival with or without those types of CT’S.
In a clinical consultation, the doctor’s motivation to propose a CT may be biased by its interpretation of the aggressiveness of the cancer. For example, the doctor would be more inclined to suggest a CT to a woman with stage III hormone receptor-negative breast cancer with lymphovascular invasion compared to a patient with stage I hormone receptor-positive breast cancer. This could introduce an indication bias [29].
The limitation of our study could be the power. With the population we had,with 80% power (α=0.05), the study would had enough power to detect a HR of 0.83 favouring women in CTs [20,21]. Further information bias includes not taking into account the women having participated only in a metastatic CT; these women were considered as not exposed to a CT. This might have resulted in a biased measure of association, since the metastatic disease is associated with unfavourable prognosis for survival in breast cancer. On the other hand, only 1.4% (n=92) of the entire cohort had participated in one or more metastatic CTs with no prior participation in other CTs; therefore, the conclusion is unlikely to have changed. Lastly, HER2 status, a prognostic and predictive factor was not included in our study since it was available only in the last few years of the study cohort. The difference between the characteristics of women who participate in CTs and those who do not participate is an important element that influenced the results of this study.
The strength of our study is the long follow-up period. Such a long period provided more relevant results. Also, the large amount of information available in the CMS database enabled analyses with adjustment for prognostic factors of breast cancer. Strength of our study is that all patients were followed and treated by the same team that applied the standards of each year of the study. It minimizes the possible confounding bias from difference in practice by different hospital, team, etc.
In conclusion, participation in CTs per se does not improve the survival of patients with breast cancer. These results, which take into account all the variables of adjustment, have not demonstrated a statistically significant difference in survival rates between CT versus non-CT patients. However, with the adjusted measures of association, being close to the null value, it can be concluded that the CTs does not have a deleterious effect on the participants. Furthermore, regardless of the arm to which patients are assigned, they are guaranteed to receive, at the very least, standard treatment in accordance with practice guidelines.
St-Sacrement Hospital Ethical Review Board approval was obtained for the present study.