Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2011) Volume 1, Issue 1
Background: Standardizing patient care is a challenging task in studies of patients with acute illness. Use of a lung-protective ventilation (LPV) protocol in studies of patients with acute lung injury is associated with reduced mortality and is the current standard for invasive ventilation in such studies. However, achieving the goals of an LPV protocol can be challenging. Methods: In a Phase III clinical study of pulmonary surfactant administration to patients with acute respiratory insufficiency due to pneumonia or aspiration of gastric contents, we performed an observational analysis to assess whether the goals of a specified ventilation protocol were achieved. Ventilation parameters, including tidal volume (VT) and peak inspiratory pressure (PIP), of the first 200 patients enrolled were analyzed. Subsequently, an intensified training program was initiated to improve achievement of protocol goals, and this achievement was assessed again in the next 643 randomized patients. Results: Implementation of intensified training measures was accompanied by a significant reduction in median values of VT from 7.8 to 7.0 mL/kg predicted body weight (PBW) and PIP from 29.5 to 28.5 cm H2O. Use of VT based on actual body weight, as opposed to PBW, may impair goal achievement. Goal achievement varied among countries and improved significantly in some with intensified training measures. Conclusions: Specific training measures may be effective in promoting achievement of goals of a pre-specified ventilation protocol in multinational clinical trials. Strategies described in this study may be helpful in achieving compliance with complex protocol demands in a variety of clinical trials.
Keywords: Clinical trial; Multicenter trials; Critical illness; Pulmonary surfactant
ABW: Actual Body Weight; APACHE II: Acute Physiological and Chronic Health Evaluation II; ARDS: Acute Respiratory Distress Syndrome; FiO2: fraction of inspired oxygen; ICH: International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use; LPV: Lung-Protective Ventilation; PaO2: partial pressure of arterial oxygen; PBW: predicted body weight; PEEP: positive end-expiratory pressure; PIP: peak inspiratory pressure; SECB: Scientific Enrollment Coordination Board; SOFA: Sequential Organ Failure Assessment; VT: Tidal Volume
Standardization of care in studies of critically ill patients is challenging. This is particularly true for mechanical ventilation. Although mechanical ventilation plays an important part in the treatment of acute respiratory failure, it can cause lung injury when alveoli are over-distended by high tidal volume (VT) or high inflation pressures [1,2]. Such ventilator-induced lung injury results in inflammatory responses that cause further damage to the lungs [3-5].
Numerous studies have investigated different strategies to minimize the adverse impact of mechanical ventilation on patients’ lungs, but only a protocol-based lung-protective ventilation (LPV) strategy has resulted in significant improvement in survival [6]. However, despite the clear benefit of LPV, many patients with acute lung injury have received mechanical ventilation with VTs above the goal of 6 mL/kg predicted body weight (PBW) [4,7-13].
Within multinational clinical trials, achievement of LPV protocol goals has been variable. For example, in the STRIVE study, goal achievement was excellent (mean VT 6.8 mL/kg PBW) [14], whereas in several subsequent clinical trials it was less favorable (mean VTs of 8.4 to 8.8 mL/kg PBW) [13,15].
Such variability in achieving LPV goals and conflicting reports of concordance between trials and clinical practice demonstrate that standardization of patient care remains a challenge in studies of critically ill patients [16,17].
As pointed out by Cooke et al, there has been no investigation of factors that promote adherence to an LPV protocol [18]. To encourage investigation in this area, we have conducted an observational analysis of data from the VALID study, a randomized Phase III investigation of the benefit of intratracheal instillation of a surfactant suspension (Venticute®; Nycomed GmbH, Konstanz, Germany) to patients with pneumonia or aspiration of gastric contents who are intubated and mechanically ventilated [19].
In this study the use of the Acute Respiratory Distress Syndrome (ARDS) Network LPV protocol was strongly recommended. However, after the initial analysis of the first 200 patients, it became apparent there was a need for further training measures to reduce VT levels to the recommended values. Here we describe: changes in achieving goals of a LPV protocol that were observed after implementing intensified training measures; the variability among countries in initial and post-training choice of VT; and the discrepancy caused by use of actual body weight (ABW) as opposed to PBW.
Study description
The VALID study (clinicaltrials.gov identifier: NCT00074906) was a randomized, parallel-group, double-blind, controlled study enrolling patients with lung injury in 161 medical centers in 22 countries conducted from November 2003 to March 2008. Trial design, patient characteristics, and outcome measures have been published previously [19].
The following ARDS Network LPV protocol items were emphasized in the protocol for the VALID study:
- Ventilation with low VT of 6 mL/kg PBW, plateau pressure goal ≤ 30 cm H2O
- Arterial oxygenation goal of PaO2 55 to 80 mmHg (equal to 7.3 to 10.7 kPa) or oxygen saturation 88% to 95%
- FiO2 and PEEP combinations as described in ARDS Network ventilation protocol [6]
Training measures
Initial training measures: The VALID study protocol required that use of the ARDS Network ventilation protocol be emphasized at initial site visits and investigator’s meetings before patients were enrolled at each center. Adherence to the ARDS recommendations in terms of VT and arterial oxygenation goals were strongly recommended as part of the initial training measures. However, patient-specific details of the volume or pressure-controlled ventilation were at the discretion of the treating physician.
Intensified training measures: To encourage improved adherence to the ARDS Network ventilation protocol, four intensified training methods were used as part of the VALID study, subsequent to observations that demonstrated an opportunity for improved adherence to the LPV protocol during the study of the first 200 patients.
1. Teleconferences were organized with investigators at the initiation of the intensive training measures. Updates on the progress of lowering VT were emailed to all investigators every 6 months and on occasion of national and international investigators’ meetings as they occurred.
2. Data regarding the magnitude and distribution of VTs used at specific study sites were disclosed to the investigators at those sites during visits by the clinical research associate (which occurred when study patient data were collected) and/or during the sponsor’s study site visits. These data, as well as those aggregated by country, were presented and discussed with the investigators, with the request to more closely adhere to the VT goals, if necessary.
3. Just prior to patient enrollment, site investigators were required to discuss patient suitability for the study with a physician member of the trial Scientific Enrollment Coordination Board (SECB). The function and operation of this Board has been described previously [20]. Discrepancies between the recommended patient-specific VT and the VT actually being delivered to the patient were discussed with the study site investigator as part of the intensified training measures.
4. Case report form data, including ventilation parameters from 26 time points during the first 5 days of the study, were entered into the sponsor’s database. Data on ventilation parameters that deviated from the recommended LPV protocol values were used to provide feedback to the study sites and maintain awareness. For 576 patients (68.3% of the study population) a median of five (1 to 11 [25% to 75% quartile]) time points with a VT >8 mL/kg PBW was identified. One summary query for each of these patients was then issued to the relevant site.
Observational assessments
To assess achievement of LPV protocol goals, VT and peak inspiratory pressure (PIP) were measured at the beginning and end of the 2-hour baseline period before randomization. Values were averaged for individual patients. Although measurement of plateau pressures would have been preferable, standardized methodology across the 161 participating centers was not achieved. Investigators were requested to avoid, if possible, changes in ventilator settings during the baseline period. Achievement of the ARDS Network LPV protocol goals was assessed in consecutively enrolled patients before (patients 1 to 200) and after (patients 201 to 843) intensified training measures were implemented. Median VT during the study was calculated for each country that had enrolled at least 12 randomized patients. Comparison of median baseline VT per kg PBW and per kg ABW was undertaken. Each study patient contributed one pair of values. For display, the patients were sorted by VT/kg ABW and the corresponding value for VT/kg PBW was plotted above or below it.
Statistical analyses
Descriptive statistical analysis was performed, including mean ± standard deviation and 90%, 75%, 50%, 25%, and 10% percentiles. The Cochran-Armitage Trend Test was used to compare the frequency distribution of VT at baseline. The regression coefficient for trend of VT in cohorts of 200 consecutively enrolled patients (243 for the last cohort) was tested using a t-test. All other comparisons between ‘prior to intensified training measures’ (patients 1 to 200) and ‘with intensified training measures’ (patients 201 to 843) were performed using the two-sided Wilcoxon test.
The demographic characteristics for the 843 patients randomized in the VALID study have been published previously [19]. For all enrolled patients, the mean PaO2/FiO2 ratio was 123.9 ± 0.93 mmHg, and 58.6% of these patients had ARDS at baseline as previously defined by the American European Consensus Conference criteria [21]. Patients with unilateral opacities on the chest radiograph were not categorized as having ARDS. Pneumonia was the most common cause of acute lung failure, occurring in 728 (86.4%) of patients.
Box plots of distribution of VT at baseline in 18 countries are shown in Figure 1 and demonstrate wide differences in VT among countries. Patients in Estonia (median of 6.1 mL/kg PBW), New Zealand, Russia, and Denmark received the lowest VT, followed by Austria, Germany, Argentina, and Spain (median< 7.0 mL/kg PBW). VT goal achievement in other countries was less favorable, with seven countries having a median baseline VT of > 7.5 mL/kg PBW. The countries with the highest median VT were Canada and Switzerland (8.1 mL/kg PBW). Intensified training measures improved VT goal achievement in several countries. In the USA, mean VT was significantly lower following the implementation of intensified training than prior to training (7.3 mL/ kg PBW vs 8.5 mL/kg PBW; p=0.0003). Other countries for which statistically significant improvement in VT goal achievement were observed included Australia (p=0.0113), Belgium (p=0.0087), Germany (p=0.0345), and Hungary (p=0.0031).
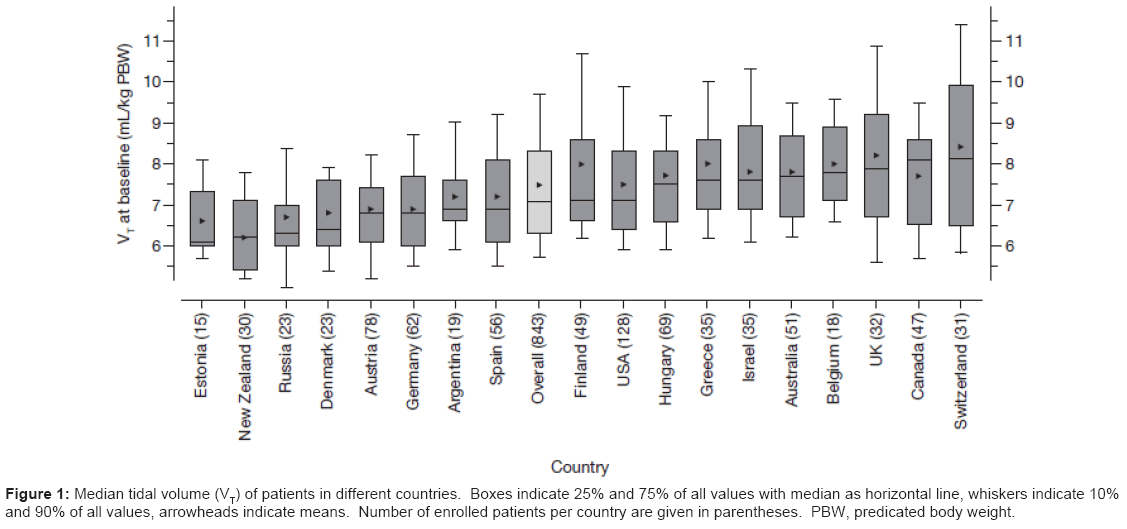
Figure 1: Median tidal volume (VT) of patients in different countries. Boxes indicate 25% and 75% of all values with median as horizontal line, whiskers indicate 10% and 90% of all values, arrowheads indicate means. Number of enrolled patients per country are given in parentheses. PBW, predicated body weight.
Overall, achievement of the ARDS Network LPV protocol VT goal was significantly improved after intensified training compared with pretraining adherence (Figure 2). For the first 200 patients treated before intensified training, median (25th to 75th percentile) VT at baseline was 7.8 (6.6 to 9.0) mL/kg PBW compared with 7.0 (6.2 to 8.0) mL/kg PBW in the 643 patients treated after initiation of intensified training (p<0.0001). Immediately after implementation of the intensified training measures, median VT decreased to 7.4 mL/kg PBW (patients 201 to 400). With continuation of training efforts, median VT continued to decrease to 7.1 mL/kg PBW in the next 200 patients (up to patient 600), and to 6.7 mL/kg in the following 243 patients (up to patient 843; p<0.0001 (Figure 2)), indicating ongoing decline over time. Furthermore, patients were more likely to be ventilated with a VT consistent with the ARDS Network LPV protocol after intensified training measures had been applied (patients 201 to 843; p<0.001 (Figure 3)).
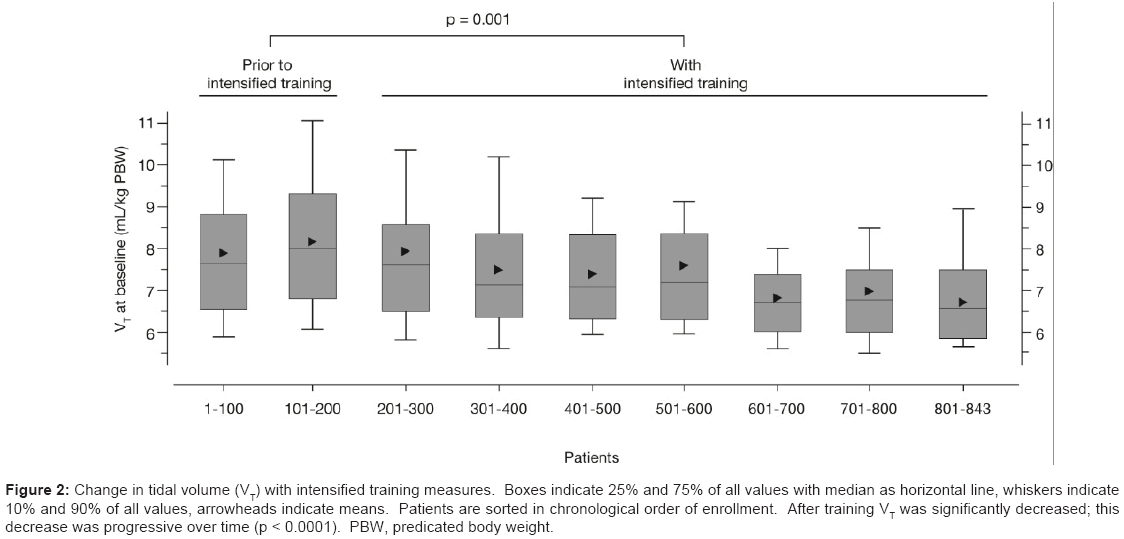
Figure 2: Change in tidal volume (VT) with intensified training measures. Boxes indicate 25% and 75% of all values with median as horizontal line, whiskers indicate 10% and 90% of all values, arrowheads indicate means. Patients are sorted in chronological order of enrollment. After training VT was significantly decreased; this decrease was progressive over time (p < 0.0001). PBW, predicated body weight.
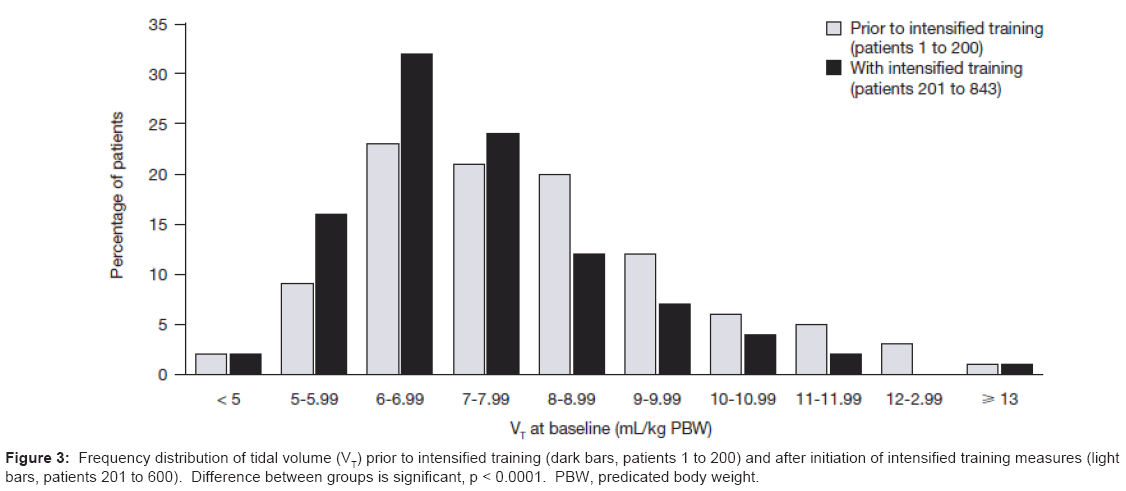
Figure 3: Frequency distribution of tidal volume (VT) prior to intensified training (dark bars, patients 1 to 200) and after initiation of intensified training measures (light bars, patients 201 to 600). Difference between groups is significant, p < 0.0001. PBW, predicated body weight.
For each individual patient, VT was calculated on the basis of ABW and the values were sorted by VT/kg ABW. These values were plotted in ascending order, starting with the patient with the lowest VT/kg ABW. This resulted in a sigmoid distribution curve. We then calculated the VT of each patient based on PBW and added these values to the graph. The resultant scatter plot indicates that using ABW is misleading because it frequently results in VT values considerably lower or higher than the appropriately calculated VT using PBW (Figure 4).
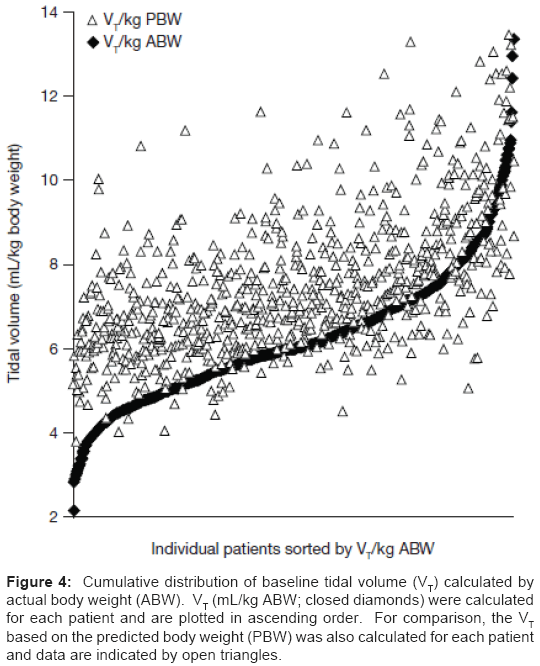
Figure 4: Cumulative distribution of baseline tidal volume (VT) calculated by actual body weight (ABW). VT (mL/kg ABW; closed diamonds) were calculated for each patient and are plotted in ascending order. For comparison, the VT based on the predicted body weight (PBW) was also calculated for each patient and data are indicated by open triangles.
Median (25th to 75th percentile) PIP at baseline was reduced from 29.5 (25.0 to 34.5) cm H2O before intensified training to 28.5 (23.5 to 32.5) cm H2O (p=0.002) after intensified training (Figure 5).
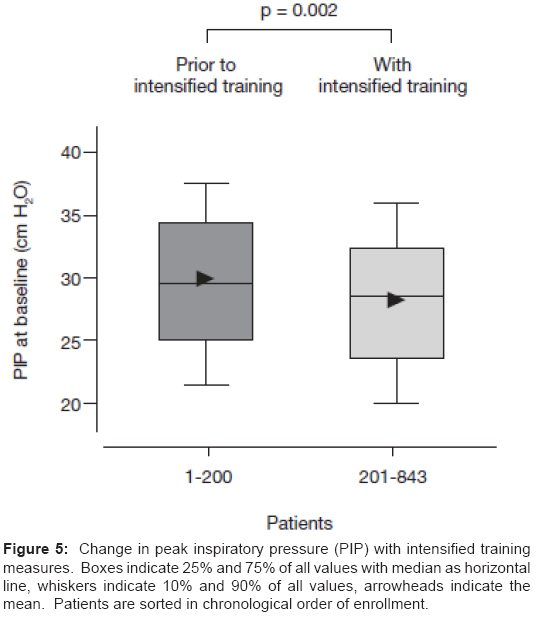
Figure 5: Change in peak inspiratory pressure (PIP) with intensified training measures. Boxes indicate 25% and 75% of all values with median as horizontal line, whiskers indicate 10% and 90% of all values, arrowheads indicate the mean. Patients are sorted in chronological order of enrollment.
Site investigators in this multinational study were advised to comply with the ARDS Network LPV protocol. After the first 200 patients had been enrolled into the study, it became apparent that compliance with this protocol, particularly with use of VT of 6 mL/ kg PBW, could be improved. While no specific measures have been shown prospectively to be effective [18] evidence supports the use of multifaceted interventions that include education, reminders, and feedback [22]. For this reason, four specific training interventions were implemented. These provided: real-time reminders to the site investigator at the time of patient enrollment to use the appropriate VT; feedback that reported the VTs actually used by that investigator as well as by investigators in different countries; feedback focusing on use of excessive VTs; and regular teleconferences and mailings designed to provide ongoing education. In a small, retrospective study, Wolthuis et al. [23] suggested that such measures may promote adherence to an LPV protocol.
Achievement of LPV protocol VT goal improved after implementing training measures, as reflected by a fall in median VT from 7.8 mL/kg PBW (patients 1 to 200) to 7.0 mL/kg PBW (patients 201 to 843), and to 6.7 mL/kg PBW in the final cohort reported (patients 601 to 843). One can question whether this modest change is of clinical relevance; however, the point of this observational study was to identify strategies that improved achievement of the LPV protocol goals. The training measures that were implemented here were accompanied by a 44% reduction in median VT delivered in excess of the goal of 6.0 mL/kg PBW. In addition, these training measures also were accompanied by a small but significant decrement in PIP.
Our observations have several limitations that deserve comment. First, they are uncontrolled and indeed it is ethically impossible to purposefully under-train study site investigators on an intervention thought to improve patient survival. However, our observations are based on a large number of patients and on the care delivered at 161 sites in 22 countries. While it is possible that achievement of the VT goal of the ARDS Network LPV protocol may have improved internationally and independently of our intensified training measures, we believe that such an abrupt improvement, coincident with the implementation of these measures, would be unlikely.
A second limitation is absence of measurements of inspiratory plateau pressure. The LPV protocol that was recommended in the VALID trial called for achieving a plateau pressure less than 30 cm H2O. Unfortunately, methods for measuring plateau pressure were not standardized across the 22 countries participating in the study, and the only reliable measurements of pressure that are available for analysis are those of PIP. PIP is reported to exceed plateau pressure by approximately 5-7 cm H2O in patients with ALI [24]. It is likely that the reduction in PIP noted after the implementation of intensified training measures reflects a true decrement in plateau pressure.
A third limitation is the absence of information on the ventilatory mode used, and specifically if more patients were managed with volume control ventilation after the interventions.
We observed considerable variation in baseline VT among the participating countries. A retrospective study analyzing 149 patients in two hospitals in the USA reported a mean VT of 7.6 (standard deviation 2.1) mL/kg PBW on the first day [11]. Interestingly, they reported a hospital mortality of 41%, which compares with a mortality of 32% reported in another observational study that adhered to the ARDS Network protocol in an equivalent patient population [25]. The authors suggested that these differences in mortality may be partly attributable to the less rigorous adherence to the ARDS Network goal of a VT of 6 mL/kg PBW [11].
In the conduct of a large multinational study of patients with severe lung injury, achieving adherence to an LPV protocol at multiple sites in multiple countries is challenging. As the study end point is often mortality, and mortality is significantly affected by the ventilation strategy, such adherence is critical. In the STRIVE study, investigators were successful in standardizing ventilator management across 105 institutions in six countries with enrollment of 429 patients with acute lung injury, achieving a median VT of 6.5 mL/kg PBW [14]. The VALID study, covering 161 centers in 22 countries, was significantly larger, with increased difficulty of assuring compliance to the LPV protocol. Achieving a median VT within target range after implementing intensified training measures may provide a temporary benchmark for studies of this magnitude.
Low-stretch ventilation is now considered the current standard of care in the treatment of patients with acute lung injury or ARDS [8,27], and a clearly stated LPV management strategy should be considered for inclusion in study protocols. This observational study describes methods that promote achievement of the goals of a LPV protocol. Given the direct impact of ventilation protocols on mortality, the most significant end point in studies of critically ill patients, continuing attention must be given to methods of optimizing achievement of LPV protocol goals.
In a large multicenter international study, compliance with the ARDS Network LPV protocol was inconsistent, resulting in significant variation of delivered VTs among 161 sites in 22 countries. Implementation of specific training measures was accompanied by improved achievement of LPV protocol goals, with a lowering of the median VT and PIP and a narrowing of the variation of the VT values.
Clinical trials involving patients with acute respiratory failure require adherence to a LPV protocol. Intensive measures to improve achievement of protocol goals may be of value.
The VALID study was sponsored by Nycomed GmbH, Konstanz, Germany. Funding for the analysis described in this manuscript consisted of salary support by Nycomed GmbH for authors affiliated with that company. The sponsor provided full information to the senior author (Dr. Spragg) who wrote the manuscript. The decision to submit the manuscript for publication was not determined by the sponsor.
All authors have reviewed and take full responsibility for the content of the manuscript. They gratefully acknowledge the statistical support of Markus Roters, PhD, Omnicare Clinical Research, Cologne, Germany, and the editorial assistance of Lynda Chang, PhD, Complete HealthVizion, Glasgow, UK. Editorial assistance was funded by a grant from Nycomed GmbH.