Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2016) Volume 6, Issue 5
Background: Trauma is a leading cause of death worldwide and massive bleeding is the main cause of death in the first 24 hours after injury. Patients with large blood volume loss should undergo the massive transfusion protocol to quickly restore the blood volume and the clotting factors that were lost during bleeding. There are two common strategies regarding transfusion therapy for multiple trauma patients with severe bleeding. The fixed ratio strategy is based on the proportional transfusion of packed red blood cells, fresh frozen plasma and platelets (fixed ratio 1:1:1). The thromboelastometry guide approach is based on the physiopathology of the trauma coagulopathy is a phenomenon that occurs in the early stages of trauma, with hyperfibrinolysis and fibrinogen consumption. Blood products are given based on viscoelastic tests. Methods/design: This study is a prospective, single-center, open-label, randomized trial. Males and females between 18 and 80 years old, with severe trauma and a high Injury Severity Score (ISS- greater or equal than 15) admitted to trauma emergency room are included. To be included, patients require is bleeding actively, with inclusion criteria’s to massive transfusion protocol. Patients are randomly allocated to one of the two strategies for massive transfusion (Group A- fixed ratio 1:1:1 or group B- thromboelastometry guided). The primary outcome is the incidence of organ dysfunction on the first, 5th, and 7th day until 28 days post. The secondary outcome are the consumption of blood products within 48 hours, the length of stay in the hospital, days without mechanical ventilation and the financial costs in both groups. Discussion: This trial was proposed to answer questions about the outcomes related to these two strategies of transfusion. This study is important because there is a lack of prospective studies with the subject proposed. Trial registration: Clinical Trial NCT02416817
Keywords: Bleeding; Massive transfusion; Trauma; ÃÂromboelastometry Coagulopathy
TEG®: Thromboelastography; ISS: Injury Severity Score; ICU: Intensive Care Unit; TIC: Trauma Induced Coagulopathy; ROTEM®: Rotational Thromboelastometry; SAPS: Simplified Acute Physiology Score; SOFA: Sequential Organ Failure Assessment; HCFMUSP: Hospital das Clínicas da Faculdade de Medicina de São Paulo; ml: millilitre; Kg: Kilogram; Min: Minute; ABC: Assessment of Blood Consumption; PT: Prothrombin Time; APTT: Activate Partial Thromboplastin time; PCC: Prothrombin Complex; FFP: Fresh Frozen Plasma; G: Gram; DL: Decilitre; TBI: Traumatic Brain Injury.
Massive transfusion protocol
Trauma is a leading cause of death worldwide and massive bleeding is observed as the main cause of death of the victims in the first 24 hours after injury [1]. There is an agreement in the current medical literature that severe multiple trauma patients with active bleeding, should have their blood losses initially treated with the minimum necessary quantities of crystalloid solutions [1-5]. If the signs of hemodynamic instability persist, blood components should be transfused. Transfusion of blood products is performed to achieve an optimal supply of oxygen to the tissues and correct the incipient coagulopathy. Coagulopathy is recognized as an important participant in the lethal triad of trauma.
Patients with large blood losses [2] (at least 50% of their blood volume in 3 hours or 1.5 ml/kg/min for 20 minutes) should undergo transfusion to quickly the blood volume and the clotting factors that were lost during the bleeding [2]. There are two strategies regarding transfusion therapy for trauma patients with severe bleeding in the literature (fixed ratio and thromboelastometry guided approach).
Transfusion strategies
The fixed ratio treatment is based on the proportional transfusion of red blood cells, fresh frozen plasma and platelets in trauma patients with severe bleeding [2]. Damage control hematology or damage control resuscitation has as a target the rapid control of the bleeding and an early supplementation of blood products. According to the literature, fixed ratio treatment decreases mortality. These ratios are 1: 1: 1 in an attempt to provide a composition that is similar to the whole blood.
The thromboelastometry guided approach to transfusion therapy is based on the current understanding of the pathophysiology of trauma coagulopathy and the selective replacement of blood products. Induced trauma coagulopathy is a phenomenon that occurs in the early stages of trauma and is triggered by hypotension and/or hypoperfusion, pharmacological agents (antifibrinolytic drugs, use of concentrates of coagulation factors such as fibrinogen and prothrombin complex, factor XIII) [6,7]. Part of the hypothesis of trauma induced coagulopathy (TIC) is explained by the "clot breakdown", wherein occurs an exacerbated fibrinolysis. The hyperfibrinolysis leads to the consumption of coagulation factors and lysis of fibrin. Currently, many studies have been performed to develop strategies to detect and treat this exacerbated response of the coagulation system. This knowledge helps direct the goal-directed therapy for the replacement of coagulation factors specifically required [8-10]. The use of rotational thromboelastometry (ROTEM®) or thromboelastography (TEG®) has become a fundamental part of this type of treatment [2,5,6]. Fibrinogen, clotting factor I, plays an important role in coagulation. The concentration of fibrinogen in the plasma is the highest of all the coagulation factors. Because this protein is present during the acute phase, its level in the plasma increases during inflammation. In the final phase of coagulation, the majority of the fibrinogen is captured by activated platelets that in turn are triggered by the glycoprotein IIb/IIIa receptors [11-14]. Coagulopathy induced by trauma or by hemodilution, fibrinogen is the first clotting factor that undergoes reduction to a critical level [14].The prothrombin complex concentrate has been used for many years in clinical practice for the correction of coagulation disorders related to the use of Vitamin-K antagonists. It contains factors II, VII, IX and X. Due to the great loss of coagulation factors during bleeding; this complex has been designed for rapid replacement of the factors in trauma patients when guided by thromboelastography [15]. Studies [11] suggest that thromboelastrometry would be a more appropriate approach to monitor hemostasis, as it would be able to quickly provide information about the polymerization of fibrin in the presence of platelet activity, fibrinogen deficiency assessment and factor XIII deficiency.
Non-pharmacological treatment (active heating, pH and calcium correction) is observed as the key components in coagulopathy therapy.
Based on the need to answer questions regarding the short-term and long-term outcomes related to these two strategies of transfusion therapy, we developed this randomized study using adult patients with severe trauma, massive bleeding and the need for a massive transfusion. This study is important because it is an original trial and there is a lack in the literature of studies with the same number of patients as this analysis. Because this is a study undertaken in a major trauma center in Brazil and the results can be used worldwide.
Aims of the study
The primary objective of this study is to compare the two transfusion strategies (fixed ratio versus thromboelastometry guided approach) in adult trauma patients, undergoing massive transfusion to assess the following:
.1-The incidence of organ dysfunction in both groups of patients treated by the different strategies through the use of the Simplified Acute Physiology Score (SAPS) at admission and the Sequential Organ Failure Assessment (SOFA) on the first, 5th, and 7th day until 28 days post-admission.
Secondary aims are as follows
1-Estimated financial cost (inputs, blood products and drugs) of transfusion therapy for group A (fixed ratio) and group B- (thromboelastometry guided)
2- Determine days free of mechanical ventilation
3- Establish the length-of-stay hospital (LOS)
4--Determine readmission to the intensive care unit (ICU) due to bleeding
Study design
This study is a prospective, single-center, open-label, randomized trial, utilizing adult trauma patients admitted to the emergency room of the Surgery Department (Central Institute in Hospital das Clinics, São Paulo University, Brazil). The patients are followed from their admission, to emergency room, to the operating room and the followup in the intensive care unit and regular hospital bed, of the Central Institute of the HC- FMUSP until 28 days after discharge.
Included patients are admitted to the emergency room, and require a massive transfusion. Patients with an estimated blood loss of at least 50% of their blood volume in 3 hours, or 1.5 ml/kg/min for 20 minutes [2], and/or patients without an estimated blood loss that have the “scores” necessary to require a massive transfusion protocol in an emergency (Shock Index Score and Assessment Blood Consumption Score) are included.
Inclusion criteria
1-Trauma patients (both genders) with an Injury Severity Score (ISS) greater than or equal to15 (Table 1). The Injury Severity Score (ISS) is an anatomical scoring system that provides an overall score for patients with multiple injuries.
| Region | InjuryDescription | AIS | SquareTop Three |
|---|---|---|---|
| Head & Neck | Cerebral Contusion | 3 | 9 |
| Face | No Injury | 0 | |
| Chest | Flail Chest | 4 | 16 |
| Abdomen | Minor Contusion of Liver Complex Rupture Spleen |
2 5 |
25 |
| Extremity | Fractured femur | 3 | |
| External | No Injury | 0 | |
| Injury Severity Score: | 50 | ||
Table 1: Injury Severity Score.
Each injury is assigned an Abbreviated Injury Scale (AIS) score and is allocated to one of six body regions (Head, Face, Chest, Abdomen, Extremities (including Pelvis), External). Only the highest AIS score in each body region is used. The 3 most severely injured body regions have their score squared and added together to produce the ISS score. An example of the ISS calculation is shown in Table 1.
2- Aged between 18 and 80 years old.
3- Patients with an estimated loss of at least 50% of their blood volume in 3 hours, or 1.5 ml/kg/min for 20 minutes [2].
4- For patients in which we are unable to quantify the volume loss in the hospital due to an exsanguination documented at the scene of trauma, the transfusion protocol will be based on scores.
The results are used to classify these patients for a massive transfusion, and the results should be positive when two scores are combined: ABC Score [15] over 03 points and a Shock Index [16] greater than 1.2 (Table 2).
| Penetrating trauma (0=no, 1=yes) |
| Systolic blood pressure lower than 90 mmHg at emergency admission (0=no, 1=yes) |
| Heart rate greater than 120 bpm at emergency admission (0=no, 1=yes) |
| FAST positive (0=no, 1=yes) |
Table 2: ABC Score12 (Assessment of Blood Consumption). A score equal to or greater than 2 can be used as a predictor of massive transfusion. A score of 0 or 1 is not a massive transfusion predictor, Shock Index: Cardiac rate/ Systolic blood pressure.
5-For victims with a traumatic amputation of limbs with exsanguination documented at the trauma scene, the transfusion protocol will be based on the degree of hemorrhagic shock IV, according to the American College of Surgeons [17] (Table 3) because these patients are unable to have a combined high score (ABC>3 and SI> 1.2) due the trauma mechanism.
| Degree of hemorrhagic Shock | ||||
|---|---|---|---|---|
| I | II | III | IV | |
| Blood loss (mL) | ≤ 750 | 750-1500 | 1500-2000 | ≥ 2000 |
| Blood loss (volume %) | ≤ 15 | 15-30 | 30-40 | ≥ 40 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Cardiac rate (bpm) | <100 | >100 | >120 | >140 |
| Respiratory rate | 14-20 | 20-30 | 30-40 | >35 |
| Diuresis | ≥ 30 | 20-30 | 5-15 | Absent |
| Mental state | Anxious | Very anxious | Anxious and confused | Confused, lethargic |
Table 3: Degree of hemorrhagic shock, according to the American College of Surgeons.
Exclusion criteria
Exclusion criteria will are as follow: 1) patients not meeting the inclusion criteria; 2) legal guardians or patients who to refuse to sign the Term of Consent, or a request to withdraw from the study at any time; 3) pregnant patients and patients younger than 18 years old; 4) patients with previously diagnosed coagulation disorders; 5) patient's death within the first 06 hours; 6) history of cardio-respiratory arrest at the trauma scene; 7) isolated brain traumatic injury; 8) admission to the emergency room more than 6 hours after the trauma; 9) previously use of anticoagulant and/or antiplatelet drugs and 10) patients with a history of thromboembolic events (deep vein thrombosis, myocardial infarction, pulmonary embolism, stroke or heparin-induced thrombocytopenia type 2 in the last 12 months).
Randomization
Ethical considerations: This trial was approved by the Ethics Committee for Project Analysis Research (CAPPesq) from the Hospital das Clinics Medical School, São Paulo University- HC-FMUSP (Brazil Approval Pl 202,002 online in 9771). The Term of Consent will be displayed (read) to the patient or their legal guardian. In cases where there is no responsible person present and/or able to sign, an independent physician not involved in the research of the emergency services, will be responsible for signing the free informed consent form .As soon as the responsible person is found (until 24 hours after the patient's admission to the hospital), a new inform consent is presented to him/her by the main researcher. If the person responsible for the patient refuses to sign it, the patients are excluded from the study immediately.
Work plan: A researcher member is present in emergency department 24 hours for 7 days per week (nurse team and a physician). After the patient's admission to the emergency room, the researcher will be responsible for the observation of all the inclusion and exclusion criteria, and to make the appropriate allocations in the trial. After the patient's allocation to the study, the patient will be recruited as a selected patient, and the patient, legal guardian or independent physician will sign an informed Consent. Patients who meet the inclusion criteria are undergo massive transfusion protocol in one of the groups. Patients are randomly allocated according to a predetermined order by sealed envelopes containing the two strategies of transfusion treatments (group A or group B). On admission will collect a complete coagulation profile (PT, APTT), serum fibrinogen, platelet count, and blood count and blood gas analysis with arterial lactate from all patients. Patients receive 1 g of tranexamic acid as a "bolus" for 10 minutes followed by a continuous infusion of 1 g up to 8 hours [18] on admission (first 3 hours). We also measure calcium replacement, pH and temperature in all patients.
Group A (fixed ratio strategy) will be exclusively treated with blood components (initial treatment proposed: 4 red blood cells, 4 fresh frozen plasmas and 1 platelet apheresis or 1 unit of platelets for each 10 Kg). More blood components may be given according to the clinical judgment of the attending physician provided the ratio 1:1:1 is maintained. After the end of the first "package" of transfusion (1:1:1), a new sample with a coagulation profile (PT, APTT), serum fibrinogen, platelet count, blood count and arterial blood gas analysis with arterial lactate should be taken from the patient by a staff member involved in the research.
In group B (thromboelastometry guided strategy), patients should be treated with red blood cells (04 units initially, or more red blood cells according to the clinical judgment of the treating physician) and the other blood products (coagulation factors) guided by thromboelastometry (Rotem® -Munich Germany). Based on the results, a PCC (prothrombin complex-Beriplex®) and fibrinogen (Haemocompletan®) or additional tranexamic acid can be performed An algorithm for treatment is available to guide all cases in group B (Figure 1). Platelets and fresh frozen plasma can be offered based on ROTEM® if the results suggest platelets dysfunction or specific missing factors that we cannot provide by any other method (factor V or factor XI). In these cases, platelets will be given as 1 unit for each 10 kg or 1 apheresis. The FFP will be given at rate of 15-20 ml/Kg of volume transfused if necessary.
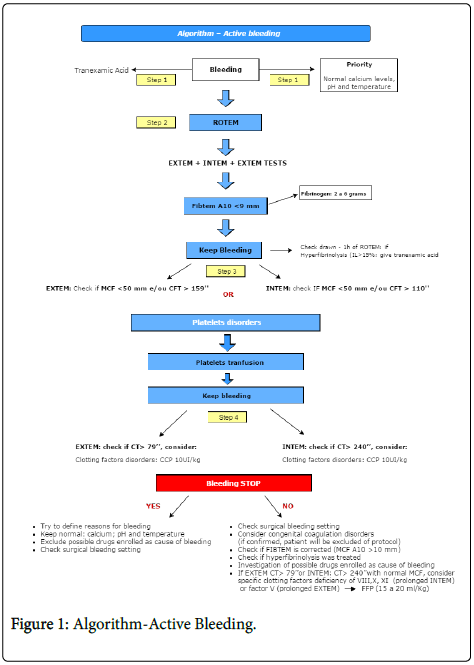
Figure 1: Algorithm-Active Bleeding.
In this group, a blood sample is analyzed by thromboelastometry (ROTEM®-Germany) by the member of the study with a mobile thomboelastographic device within first the fifteen minutes of admission. After analyzing the results of thromboelastometry, an intervention can be proposed by the study team, to correct the coagulopathy guided by the results of the thromboelastometry (algorithm treatment by ROTEM®). In this group, all transfusion aimed at coagulopathy correction should be guided by this method. The patients may receive other coagulation factors according to the results of thromboelastometry, including platelets and FFP based on the algorithm.
Concentrates of additional red blood cells in both groups are transfused according to the results of the hematocrit and hemoglobin (hemoglobin less than 7g/dL) and/or the clinical judgement of the medical team responsible for patient care.
Other data, such as the patient's temperature, blood pressure on admission, amount of fluid received on admission to the emergency room, pre-hospital time and operation room time, amount of blood products, coagulation profile (PT and APTT), platelet count and fibrinogen, time of arrival to the hospital, Injury Severity Score (ISS), presence or absence of TBI (traumatic brain injury), urine output, blood gas, doses of vasoactive drugs and laboratory data, will also be recorded. Patients are daily followed for data collection until the time of hospital discharge and followed for up to 28 days. SAPS [19] are collected at ICU admission and SOFA [20] on the first, 5th, and 7th day during the internal care unit stay. The length of stay (all in-hospital days) and days free of mechanical ventilation for recorded.
About one hundred and eighteen patients should be studied and the results will be submitted for statistical analysis.
Patients who have a clinical indication for the transfusion of packed red blood cells or platelets will not be deprived of their treatment regardless of to which group they are allocated. Patients from group B who receive transfusion therapy based on fresh plasma, cryoprecipitate or platelets according to the algorithm, will be excluded because it will be considered “break of protocol”
All patients are followed in the operating room (all procedure period) and until ICU admission, where the ICU team is instructed about the protocol. After that, all patients are visited at least twice per day (by the protocol-team), to take note of vasoactive drugs, the amount of additional fluids and transfusions, required reoperations, bleeding and thromboembolic events, oxygenation data, and other data to calculate SOFA score and other outcomes. The members that allocate and recruit patients are not the same that perform the followup. This was the way to try decrease observational bias about treatment proposed and outcomes founded.
Transfusion is part of the treatment of severe trauma patients. It improves tissue perfusion and promotes early correction of coagulopathy. There remain, however, many doubts about which strategy involves less risk to patients, less financial costs and more effectiveness for the correction of coagulopathy.
Recruitment for the study is completed. Patient recruitment began in June 2014 and finished in July 2016. We performed an interim analysis with 50% of the sample size. We did not find any difference regarding mortality between the groups, which showed that this trial did not cause any harm to patients.
The TEM Innovations Company is a donor of the reagents used in ROTEM® tests performed in this trial.
The first author gives lectures to CSL Berhing regarding coagulation and hemostatic drugs.
The other authors do not have conflicts of interests.
The ROTEM® machine and reagents used to ROTEM® analysis on the trial were donated by TEM Innovations from Germany.