Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2014) Volume 4, Issue 3
Young of both sexes practicing basketball are becoming more frequent and this consequently increases the risk of sports injury. Therefore, the objective was to analyze the characteristics of injuries and associated personal and training characteristics in young basketball players of both sexes. Methods: One-year retrospective cross-sectional survey with 580 basketball players. Basketball players were interviewed using the Reported Condition Inquiry. This questionnaire contains items addressing anthropometric data and characteristics of injuries having occurred in the previous 12 months. Results: A total of 167 of the interviewees reported injuries. Significant differences were detected regarding all variables and both sexes (except age, body mass index and duration of practice in males) between athletes who had suffered injury and those who had not. A greater number of injuries occurred in females older than 14.44 years in comparison to younger females (OR: 3.66; 95% CI: 1.85–7.21). In younger and lighter female athletes, the injuries were predominantly in the knee and ankle/foot. Conclusions: The male gender exhibited a greater risk of injury than the female gender. Greater age, weight and height were risk factors in both sexes. The most affected anatomic sites were the ankle/foot and knee.
Keywords: Trauma in athletes; Risk factors; Basketball; Sports injuries
Basketball participation in childhood and adolescence offers a number of benefits, such as increased physical fitness and motor coordination, self-discipline, control of body composition and enhanced muscle strength. It is estimated that approximately 300 million individuals play this sport throughout the world [1,2], from young beginners to high-performance athletes [3-5]. However, the regular participation among young players, added to the specific risks of the sport factors can increase the chances of suffering an injury [4–6] due mainly to the immaturity of the musculoskeletal system during the period of structural and motor development [7,8]. Additionally, the effects of the referred causal factors, also identified in other modalities, are divided into intrinsic (age, gender and biotype) and extrinsic (climate, type of floor for the sportive participation or event practiced) [9].
Sports injuries constitute an untoward adverse effect that undermines the benefits of regular physical activity. From a sports medicine perspective, the prevention of sports injuries is important, as an injury occurring at a young age can have short and long-term effects on both physical and mental health. Thus, an early sports injury can hamper physical activity for the rest of one’s life and might also influence attitudes towards sports and physical activity [10].
As a result, it is necessary to conduct prevention research to protect children and adolescents against the potential negative consequences of sports. A precondition for the development of prevention strategies is sufficient understanding of the extent (i.e. incidence) and determinants (i.e. risk factors) of sports injuries [11]. Unfortunately, there are few international studies examining this issue, which is surprising and highlights an important gap in our knowledge.
The considerable increase in the number of young basketball players leads to a consequent increase in the risk of injury, which is a growing cause of concern. Thus, the control of intrinsic and extrinsic factors associated with sports injuries has been suggested [4,12,13]. In this respect, observational investigations can offer helpful information and a detailed description of such factors [14].
Thus, the aim of the present study was to analyze the characteristics associated with sports injuries and personal [age, weight, height and Body Mass Index (BMI)] and duration of practice] among young basketball players of both sexes.
Subjects
A total of 581 basketball players (350 males and 231 females) participating in the School Games and High School Olympics in the state of São Paulo, Brazil, were randomly selected through their accommodation and competition sites for participation in the present study. There was no denial of volunteers to participate.
The participants exhibited the following mean values for males and females respectively: age: 14.60 ± 1.75 and 14.13 ± 1.61 years; weight: 66.46 ± 16.20 and 56.40 ± 11.69 kg; height: 1.74 ± 0.12 and 1.64 ± 0.09 m; BMI: 21.55 ± 16.20 and 20.64 ± 2.95 kgm-2; and duration of training: 3.38 ± 2.06 and 3.13 ± 1.79 years. After receiving verbal and written explanations regarding the procedures, all subjects signed a term of informed consent agreeing to participate in the study. This study received approval from the Human Research Ethics Committee of the UNESP – Universidade Estadual Paulista (Brazil) under process number 221/2007.
Study design and field procedures
The data were collected using the Reported Condition Inquiry questionnaire (Appendix) described by Pastre et al. and modified for basketball [15], addressing the frequency, anatomic site, mechanism and time of occurrence of sports injuries in the previous 12 months. The volunteers were approached at times not corresponding to upcoming competitive events in an attempt to avoid interrupting training for such events.
A pilot study was first carried out to adjust the methodological procedures and test the data acquisition tool on a population involved in basketball with performance level and age range similar to those of the main sample. This procedure allowed perfecting the assessment tool and training the interviewer in its administration to avoid possible errors during the data acquisition process. A single interviewer performed data collection.
After informing the volunteers regarding the objectives and legal terms for participation in the study, the interviewer read the questions to each participant and recorded the responses on numbered, individualized charts [15]. The data were then entered on a computational spreadsheet of the Excel program (Windows XP Professional) for organization and subsequent analysis.
Description of reported condition inquiry
The Reported Condition Inquiry is an effective questionnaire for gathering information on health status. This assessment tool is objective and both easy to understand and administer, which are important aspects when studying a large number of volunteers. The questionnaire addresses personal data (age, weight, height and Body Mass Index – BMI), duration of practice (in years), injury mechanism, affected anatomic site and moment at which the injury occurred.
Injury mechanism was defined as the causal factor (direct contact, non-contact and overuse) and characterized by the player’s perception of the exact moment at which signs and symptoms of an acute episode emerged and/or the type of activity during which such manifestations were accentuated. Anatomic site was defined as the location of pain or musculoskeletal discomfort marked by the volunteer on a drawing of the human body (Figure 1). Moment of occurrence regarded the specific practice or competition phase in which the injury occurred. Sports injury was defined as any musculoskeletal impairment the signs and symptoms of which resulted from the participation of the sport in either the practice or competition phases that compromised normal training in terms of form, duration, intensity or frequency, as described in previous studies [9,14,16–18].
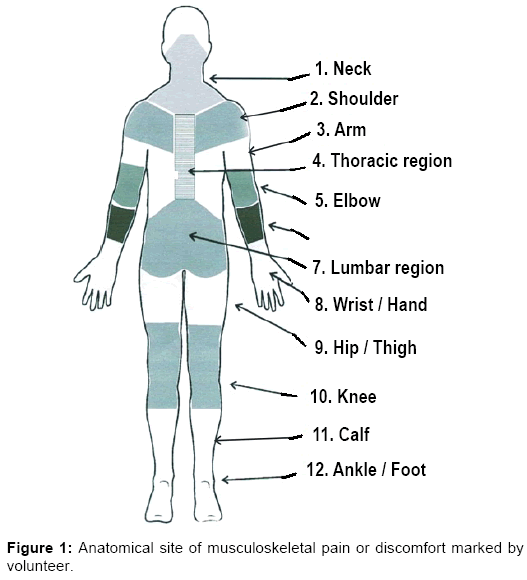
Figure 1: Anatomical site of musculoskeletal pain or discomfort marked by volunteer.
Organization and description of categories of variables
To facilitate the analysis of the results, the categories and subdivisions of the variables were grouped into more expressive blocks of results without affecting the essence of their origin or the conclusions of the study. The three main injury mechanisms were i) injury by direct contact caused by a single trauma involving contact with an opponent or the ball or a fall, ii) non-contact injury caused by movements inherent to the sport, such as short-distance running, sudden change in direction and jumping [12], and iii) injury caused by overuse, such as repetitive micro-trauma stemming from vigorous training [19]. The anatomic sites chosen for analysis were the trunk, shoulder, hand/wrist, thigh/leg, knee and ankle/foot. This information was obtained by questioning the players.
Statistical analysis
Descriptive statistics involved the determination of central tendency and variability (mean and standard deviation values). The odds ratio with a 95% confidence interval (CI) was initially calculated to determine statistically significant differences between sexes and subsequent analyses were performed separately for males and females. The Kolmogorov-Smirnov was used to determine the normality of the data. The Student’s t-test was used when normal distribution was determined and the Mann-Whitney test was used when distribution was nonparametric. Goodman’s test for contrasts between and within multinomial populations was used to determine significant associations between qualitative variables. The SPSS version 17.0 was used for the statistical analysis, with the level of significance set to 5% (p<0.05).
Among the 581 young athletes interviewed, 167 athletes reported a total of 200 injuries. Most injuries occurred during practice (74%), whereas 26% occurred during competitions. A statistically significant difference between sexes was found regarding the frequency distribution of injuries (OR: 1.55; 95% CI: 1.08 to 2.22). Table 1 displays the rates of injuries in both sexes.
| Variable | Gender | Total (n=581) | |
|---|---|---|---|
| Female (n=231) | Male (n=350) | ||
| Injured athlete | 55 (32.90%) | 112 (67.10%) | 167 (100%) |
| Injury reported | 66 (33.00%) | 134 (67.00%) | 200 (100%) |
| Rate of injury per athlete | 0.28 | 0.38 | 0.34 |
| Injury rate per athlete injured | 1.20 | 1.19 | 1.19 |
Table 1: Distribution of injured athletes, injury reported, rate of injury per athlete and injury rate per athlete injured according to gender.
Significant differences were detected in all variables and both sexes (except age, BMI and duration of practice in males) between athletes who had suffered injury and those who had not (p<0.05). Odds ratios were calculated with 95% CI to analyse risk factors of injury for those variables with significant differences detected between injured and no injured athletes (Table 2).
| Variable | Gender | Injury | p value | |
|---|---|---|---|---|
| Presence (n=167) | Absence (n=333) | |||
| Age (years) | Female | 14.81 ± 1.52 * [14.44 – 15.19] |
13.86 ± 1.57 [13.62 – 14.10] |
0.0001 |
| Male | 15.01 ± 1.79 # [14.71 – 15.31] |
14.34 ± 1.68 [14.12 – 14.57] |
0.0008 | |
| Body mass (Kg) | Female | 60.10 ± 10.79 # [57.45 – 62.76] |
54.92 ± 11.73 [53.13 – 56.71] |
0.0021 |
| Male | 69.91 ± 16.99 * [67.04 – 72.79] |
64.32 ± 15.34 [62.27 – 66.36] |
0.0020 | |
| Height (m) | Female | 1.67 ± 0.08 # [1.65 – 1.69] |
1.63 ± 0.09 [1.62 – 1.65] |
0.012 |
| Male | 1.77 ± 0.12 # [1.75 – 1.80] |
1.72 ± 0.12 [1.70 – 1.74] |
0.0001 | |
| Body mass índex (kg·m-2) | Female | 21.39 ± 2.49 * [20.77 – 22.00] |
20.35 ± 3.07 [19.88 – 20.82] |
0.008 |
| Male | 21.81 ± 3.44 [21.22 – 22.39] |
21.39 ± 3.48 [20.93 – 21.86] |
0.216 | |
| Duration of practice (years) | Female | 3.84 ± 1.94 # [3.37 – 4.32] |
2.85 ± 1.64 (3.00) [2.60 – 3.10] |
0.0004 |
| Male | 3.57 ± 1.96 [3.24 – 3.91] |
3.26 ± 2.12 (3.00) [2.98 – 3.54] |
0.058 | |
Table 2: Mean, standard deviation and confidence interval values for age, body mass, height, body mass index (BMI) and duration of practice according to gender and occurrence of injury.
Females older than 14.44 years were at greater risk of injury than younger females (OR: 3.66; 95% CI: 1.85 to 7.21). Heavier males (greater than 67.04 Kg) had a greater chance of having suffered injury than lighter males (OR: 1.72; 95% CI: 1.11 to 2.67). Females with body mass greater than 57.45 Kg had a greater chance of having suffered injury (OR: 1.72; 95% CI: 1.10 to 3.53). Male athletes taller than 1.75 m had a higher chance of having suffered injury than shorter males (OR: 2.69; 95% CI: 1.71 to 4.23). Female athletes taller than 1.65 m had a greater chance of having suffered injury than shorter females (OR: 1.89; 95% CI: 1.06 to 3.38). Females with a greater BMI (OR: 1.94; 95% CI: 1.09 to 3.45) and longer duration of practice (OR: 2.83; 95% CI: 1.48 to 5.44) had a greater chance of having suffered injury, whereas no difference was detected among males with regard to these variables.
Table 3 shows that injuries were predominantly in the knee and ankle/foot in younger and lighter female athletes, with statistically significant differences (p<0.05) in relation to the trunk, shoulder and thigh/leg. In older female athletes, the wrist/hand was significantly more affected in comparison to the trunk and shoulder (p<0.05). The knee and ankle/foot had significantly greater frequencies of injury among heavier female athletes in comparison with the shoulder (p<0.05).
| Variable | Gender | Characteristics | Anatomic site | |||||
|---|---|---|---|---|---|---|---|---|
| Trunk | Shoulder | Wrist/hand | Thigh/leg | Knee | Ankle/foot | |||
| Age (years) | Female | Younger1 | 0 (0.0) | 0 (0.0) | 6 (46.1)a,b | 1 (7.7) | 2 (15.4) | 4 (30.8) |
| Older2 | 2 (3.8) | 2 (3.8) | 6 (11.3) | 3 (5.6) | 21 (39.6)a,b,d | 19 (35.9)a,b,d | ||
| Body mass (kg) | Female | Lighter3 | 1 (4.0) | 0 (0.0) | 5 (20.0) | 2 (8.0) | 8 (32.0)b | 9 (36.0)b |
| Heavier4 | 1 (2.4) | 2 (4.9) | 7 (17.1) | 2 (4.9) | 15 (36.6)a,b,d | 14 (34.1)a,b,d | ||
| Male | Lighter5 | 3 (5.1) | 2 (3.4) | 25 (42.4)# a,b,d | 5 (8.5) | 8 (13.5) | 16 (27.1b | |
| Heavier6 | 4 (5.3) | 1 (1.4) | 10 (13.3) | 5 (6.7) | 10 (13.3) | 45 (60.0)* a,b,c,d | ||
| Height (m) | Female | Short7 | 2 (7.7) | 0 (0.0) | 4 (15.4) | 1 (3.8) | 11 (42.3)b,d | 8 (30.8)b |
| Tall8 | 0 (0.0) | 2 (5.0) | 8 (20.0) | 3 (7.5) | 12 (30.0)a | 15 (37.5)a,b | ||
| Male | Short9 | 1 (2.4) | 1 (2.4) | 18 (42.8)a,b,d | 3 (7.1) | 7 (16.7) | 12 (28.6)a,b | |
| Tall10 | 6 (6.5) | 2 (2.2) | 17 (18.5)b | 7 (7.6) | 11 (11.9) | 49 (53.3)a,b,c,d,e | ||
| Body mass index (kg·m-2) | Female | Smaller BMI11 | 0 (0.0) | 1 (3.6) | 8 (28.6)a | 3 (10.7) | 6 (21.4) | 10 (35.7)a,b |
| More BMI12 | 2 (5.3) | 1 (2.6) | 4 (10.5)e | 1 (2.6) | 17 (44.7)a,b,d | 13 (34.3)a,b,d | ||
| Duration of practice (years) | Female | Shorter duration13 | 0 (0.0) | 0 (0.0) | 4 (26.6) | 1 (6.6) | 5 (33.4) | 5 (33.4) |
| Longer duration14 | 2 (3.9) | 2 (3.9) | 8 (15.7) | 3 (5.9) | 18 (35.3)a,b,d | 18 (35.3)a,b,d | ||
Table 3: Distribution of absolute and relative (%) frequency of injuries according to anthropometric and training variables, gender and respective characteristics and anatomic site.
Heavier male athletes reported more injuries in the wrist/hand in comparison to lighter athletes (p<0.05), whereas lighter male athletes reported more injuries in the ankle/foot in comparison to heavier athletes (p<0.05). Injuries among taller females were predominantly in the knee and ankle/foot. The wrist/hand and ankle/foot were the most affected sites among male athletes. Female athletes with a higher BMI had significantly greater frequencies of wrist/hand and ankle/foot injuries in comparison to the trunk (p<0.05). Moreover, female athletes with a lower BMI had significantly greater frequencies of wrist/hand and ankle/foot injuries in comparison to the knee.
No significant differences were detected among female athletes with short duration of training (p>0.05). However, the female having practiced for a greater number of years reported injuries predominantly in the knee and ankle/foot, with statistically significant differences in relation to the trunk, shoulder and thigh/leg (p<0.05) (Table 3).
Table 4 shows that direct contact and non-contact were reported as the main mechanisms of injury rather than overuse (p<0.05), except for shorter females with a lower BMI and short duration of practice. No significant difference was found between non-contact and overuse among younger, lighter, taller females with long duration of practice (p>0.05). Regarding age, a greater frequency of injury was found in older females in comparison to younger females in relation to the overuse mechanism (p<0.05).
| Variable | Gender | Characteristics | Mechanism of injury | ||
|---|---|---|---|---|---|
| Direct contact | Non-contact | Overuse | |||
| Age (years) | Female | Younger1 | 6 (46.2) * | 7 (53.8) * | 0 (0.0) † |
| Older2 | 26 (49.0) * | 19 (35.9) | 8 (15.1) | ||
| Body mass (kg) | Female | Lighter3 | 12 (48.0) * | 11 (44.0) * | 2 (8.0) |
| Heavier4 | 20 (48.8) * | 15 (36.6) | 6 (14.6) | ||
| Male | Lighter5 | 23 (39.0) * | 32 (54.2) * | 4 (6.8) | |
| Heavier6 | 34 (45.3) * | 36 (48.0) * | 5 (6.7) | ||
| Height (m) | Female | Short7 | 11 (42.3) | 12 (46.2) | 3 (11.5) |
| Tall8 | 21 (52.5) * | 14 (35.0) | 5 (12.5) | ||
| Male | Short9 | 16 (38.1) * | 24 (57.1) * | 2 (4.8) | |
| Tall10 | 41 (44.6) * | 44 (47.8) * | 7 (7.6) | ||
| Body mass index (kg·m-2) | Female | Smaller BMI11 | 15 (53.6) * | 12 (42.8) * | 1 (3.6) |
| More BMI12 | 17 (44.8) | 14 (36.8) | 7 (18.4) | ||
| Duration of practice (years) | Female | Shorter duration13 | 5 (33.3) | 8 (53.3) | 2 (13.4) |
| Longer duration14 | 27 (52.9) * | 18 (35.3) | 6 (11.8) | ||
Table 4: Distribution of absolute and relative (%) frequency of injuries according to anthropometric and training variables, gender and respective characteristics, and mechanism of injury.
Table 5 shows that injuries were predominantly reported during practice rather than during competition. Significant differences were found between heavier and lighter males as well as between shorter and taller males (p<0.05). Regarding the training variable, significant differences were detected between heavier (higher frequency of injury) and lighter male athletes (p<0.05). Regarding the competition variable, significant differences were found between lighter (higher frequency of injury) and heavier athletes (p<0.05).
| Variable | Gender | Characteristics | Period of injury | |
|---|---|---|---|---|
| Training | Competition | |||
| Age (years) | Female | Younger1 | 6 (46.2) | 7 (53.8) |
| Older2 | 32 (60.4) | 21 (39.6) | ||
| Body mass (kg) | Female | Lighter3 | 15 (60.0) | 10 (40.0) |
| Heavier4 | 23 (56.1) | 18 (43.9) | ||
| Male | Lighter5 | 55 (93.2)*# | 4 (6.8) | |
| Heavier6 | 55 (73.3)* | 20 (26.7)† | ||
| Height (m) | Female | Short7 | 17 (65.4) | 9 (34.6) |
| Tall8 | 21 (52.5) | 19 (47.5) | ||
| Male | Short9 | 38 (90.5)* | 4 (9.5) | |
| Tall10 | 72 (78.3)* | 20 (21.7) | ||
| Body mass index (kg·m-2) | Female | Smaller BMI11 | 18 (64.3) | 10 (35.7) |
| More BMI12 | 20 (52.6) | 18 (47.4) | ||
| Duration of practice (years) | Female | Shorter duration13 | 9 (60.0) | 6 (40.0) |
| Longer duration14 | 29 (56.9) | 22 (43.1) | ||
Table 5: Distribution of absolute and relative (%) frequency of injuries according to anthropometric and training variables, gender and respective characteristics, and period of injury.
In the present study, the risk of injury was greater among males than females. Moreover, greater age, weight and height values were associated with a greater frequency of injury in both sexes and greater BMI and duration of training were associated with a greater frequency of injury in the female gender. Ankle/foot and knee injuries and the direct contact and non-contact mechanisms were the most frequently reported characteristics in both sexes regardless of the cutoff points established, whereas body weight and height were associated with a greater frequency of injury during practice among males.
The male gender had a 1.55-fold greater chance of having suffered an injury in the previous 12 months in comparison to the female gender (95% CI: 1.03 to 2.20). This finding is in agreement with that reported by Messina et al. [20] in a study involving basketball players between 14 and 18 years of age, in which 543 injuries were reported among 973 male players (injury rate: 0.56) and 436 injuries were reported among 890 female players (injury rate: 0.46), representing a 1.14-fold greater risk of males suffering musculoskeletal injury. In contrast, Moreira [21] studied basketball players with a mean age of 18 years and found that female players had a 3.9-fold greater risk of injury in comparison to male players.
One hypothesis for the increased risk of injury in the male gender is greater body size and muscle strength, resulting in an increased likelihood of collisions of greater impact [20]. Moreover, males tend to exhibit more aggressive forms of training and playing when facing opponents, which is accompanied by a greater risk of injury [22]. However, it should be stressed that studies often differ with regard to the methodology employed and the definition of sports injury, which limits the comparison of findings from different investigations [4,13].
While male players were at greater risk of injury, the injury rate in both sexes was considered low, which may be explained by the age range analyzed in the present study (14.41 ± 1.71 years). A lower degree of physical performance is expected of younger players and such individuals participate in a lower number of competitions. Thus, the lesser physical contact and lower intensity during games likely limit the number and extent of sports injuries [4].
Age was a risk factor for the female gender. The lesser risk of injury among younger female players may be associated with the frailer physical condition and lower technical level, thereby generating a lower impact and consequently less tissue damage [23]. Moreover, older girls exhibit hormonal changes that have been associated with an increased risk of injury [24].
Regarding anthropometric characteristics, studies involving male and female children and adolescents [23,25] report that spurts in weight and height represent a risk for injury due to the production of forces of greater magnitude that are potentially absorbed by soft tissues and joints. Moreover, studies have demonstrated that the greater dynamism and force of collision on the part of taller, heavier players contribute toward the occurrence of injury [23,25].
BMI was a risk factor for injury in the female gender alone. During adolescence, body composition undergoes changes, especially with regard to the percentage of body fat. In boys, there is a relative loss of fat mass, whereas the opposite occurs in girls, with a relative gain in the concentration of body fat. This greater proportion of body fat generates greater impacts of the dynamic movements of basketball, such as landing on the ground, with a greater absorption of shock in body structures and consequent greater risk of injury [25].
Duration of practice was a risk factor for injury among the female gender alone. The increase in exposure to injury may be related to the increase in repetitive and cumulative micro-traumas stemming from prolonged training to ensure improvement in skills [4]. Another reason for the increased risk of injury with a longer duration of practice may be also as a result of older age groups being larger, heavier, stronger, more aggressive and more enthusiastic to compete in their selected sport, contributing to increased injuries [26].
The ankle/foot was the anatomic site with the greatest frequency of injury. According to Gomez et al. [27], 31% of injuries to the ankle complex affect basketball players between 14 and 18 years of age. According to Timothy et al. [28], nearly 72% of grade I ankle sprains affect both the female and male gender in a population made up of elementary and high school students. The occurrence of this type of injury may be explained by the impact with the floor of the basketball court, especially during jumping and landing on the side of the foot or on someone else’s foot [15,28].
The knee was the second most affected anatomic site, regardless of the cutoff points used for individual and training characteristics. During the maximal ground reaction force, the structures of the knee are fully tensed by the impact load, which favors the occurrence of injury [3]. There is evidence that flexion of the knee during the landing phase can reduce the odds of injury due to lower ground reaction forces and lesser absorption of impact [29]. Thus, the high correlation between the flexion angle of the knee and ground reaction force may be an important factor to reduce the impact of landing after a jump and a consequent lesser possibility of injury [29]. Another explanation for knee injuries may be related to muscle fatigue, which impairs performance and alters proprioceptive function. Thus, fatigue may reduce the pre-activation of stabilizing muscles of the knee, causing a loss of balance and leading to excessive strain on the structures of the joint, particularly the ligaments, thereby favoring the occurrence of injury [3,5,29].
Regarding the mechanism, injuries caused by direct contact were the most frequent in both sexes based on the cutoff points of the anthropometric and training variables. These data corroborate findings described by Kofotolis and Kellis [30], who report direct contact to be the main mechanism of injury stemming mainly from the constant movements of the sport, such as collisions with the floor, backboard supports, teammates and opponents. According to Agel et al. [12], the high degree of physical contact between opponents, together with the lack of technique for practicing the sport on the part of young players, predispose individuals to musculoskeletal injuries.
Non-contact injuries were also frequent in the present study. Basketball is a sport that emphasizes explosive force and is practiced within a small physical space with movements that require abrupt changes in speed and direction as well as sudden rotations and numerous jumps. Thus, the dynamic conditions of the game favor the occurrence of non-contact injuries [2,15].
In the male gender, there was a predominance of injuries during practice rather than during competition considering the cutoff points for weight and height. This may be interpreted as an attempt to achieve the position of team captain, requiring the player to be ready for both the internal dispute within the team and the load to be developed, exposing the individual to more practice time. In contrast, Messina et al. [20] and Agel et al. [12] report that competition is the time in which more injuries occur. What could explain this result would actually know the amount of practice and games held weekly, unfortunately we do not have this data. In this sense, it could be considered a limitation of the study.
Moreover, physical exhaustion, especially at the end of practice, can lead to muscle fatigue and consequently compromise motor performance, thereby contributing to injury [12,31,32]. Previous studies report that the risk of injury is greater with the longer exposure of the player to practice and games [12,20]. However, this analysis was not performed in the present study.
The present study has limitations that should be addressed. The lack of the determination of the injury rate per 1000 hours of exposure to the sport does not allow the comparison of the results to findings described in other investigations of this nature. Another limitation to be pointed out is that the survey used to collect information about injuries in basketball is a strategically suitable model, however, not validated. Despite the simplicity of our questions, additional information on the respondents´ interpretation about the issues can provide greater certainty to the validity of the response and, thus, allow more precise inferences. It is also suggested an interviewer’s previous training and familiarization with the technical terms used in the sport. Moreover, although Pastre et al. [9] suggest a good correlation between the occurrence of injuries and their reports on a range of time, some information may be forgotten and, in this sense, the very design of the study limits the accurate reading on all the actual occurrences. However, the presentation of the data allowed a description of the cutoff points of the quantitative variables, which assists in the interpretation of the association between such variables and sport injuries. Thus, the information gathered can contribute to the establishment of preventive measures aimed at reducing the occurrence of injuries during the participation of basketball.
The findings of the present study revealed that the male gender (67.1%) was at greater risk of injury than the female gender (32.9%). Greater age, weight and height values were risk factors for both sexes, whereas greater BMI and duration of practice were risk factors for the female gender alone. The ankle/foot and knee were the most affected anatomic sites, independent of gender and the characteristics analyzed. For most of the individual and training characteristics, the injury mechanisms were predominantly direct contact and non-contact in both sexes. Among males, body weight and height were associated with a greater frequency of injuries during practice.
The authors declare that they have no competing interests.
The authors are grateful to the Brazilian fostering agency Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (process number 07/08038-6) and the Secretaria Municipal de Esportes de Presidente Prudente/SP (SEMEPP) for support to the present study.