Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2015) Volume 4, Issue 2
Background: Aeroallergen skin testing for assessing allergic disease has been in use for well over 100 years. Initially, trepidation to the use of skin puncture testing (SPT) occurred because of reported morbidity and mortality. SPT has most frequently been utilized in the specialist office due to fear of adverse reactions.
Methods: Analysis of 156,335 SPT tests (morbidity and mortality) allowed equivalency testing versus superiority testing to show 95% confidence level. The ninety-five percent confidence interval around the 11.5/100,000 SPT is (11.3-11.7/100,000).
Results: The literature documents 1 death from SPT from 1990 to 2001 and 1 death from 1945 to 1987. These 2 reported deaths have been contrasted with 0 deaths in 125,295 SPT patients reviewed in a primary care setting utilizing United Allergy Service protocols (UAS). Systemic reactions (SR) occurred in only 18 patients. The SR rate amongst subspecialists has been reported as a 0.015-0.023% SR per 100,000 SPT. Statistically, this result is not significantly different from the UAS SR rate of 0.0115% without associated anaphylaxis or deaths.
Conclusion: Based on the findings evident in this study, SPT is safely performed in the primary care (PC) office and allows for a larger percentage of the symptomatic population to be assessed. The observed SR rate of 11.5/100,000 SPT was statistically similar to the lowest published rate of 15/100,000 SPT (p=0.45) and statistically lower than the highest published rate of 23/100,000 SPT (p=0.02). These data suggest that SPT is as safe in the (PC) office as it is in the specialist office.
<Keywords: Systemic reaction; Aero allergen; Skin puncture testing; Primary care
Skin puncture testing (SPT) is the gold standard for the assessment of IgE mediated disease [1]. Utilizing skin testing in the Family Practice (FP) office will provide diagnostic versatility and greater patient access to assessing allergic diatheses. Aeroallergen skin testing has been in use for well over 100 years [2]. Initial trepidation to the use of SPT may have occurred because of purported morbidity and mortality reported in the American Academy of Allergy, Asthma and Immunology Immunotherapy Diagnostic Parameters whether factual or not [3,4]. SPT has often been considered dangerous in the literature [5,6]. Lockey et al. reported a number of deaths (6 from intradermal and 1 from SPT testing) from 1895 to 1968 [5]. Closer examination of the deaths revealed numerous occurrences where antiquated allergens were used. Intradermal skin tests were performed without doing SPT first, and in one instance where the application of 90 food tests were applied in one setting [5]. As a result of these poorly articulated findings, many FP are still reticent to conduct in office SPT. (Discussions with Family Practice Physicians).
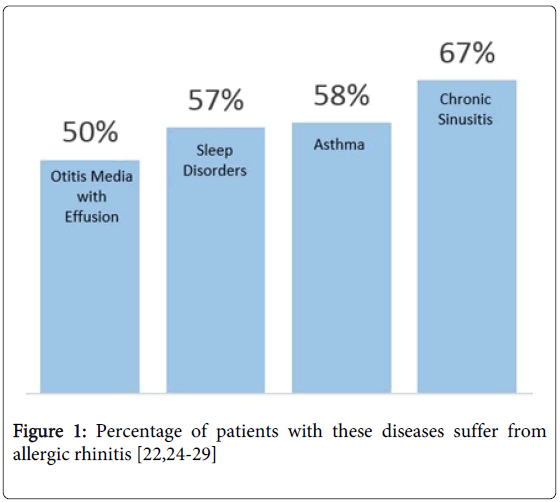
Greater than 50 million people in the United States suffer from an allergic disorder [6]. Approximately 60 percent of these patients have or will develop allergic asthma [7]. Since the majority of these individuals with allergic diatheses initially present to the FP office, SPT should be utilized in the primary care (PC) setting. The utilization of SPT by allergy specialists alone limits the number of patients who may have their allergic disorders identified and effectively treated. Allergic rhinitis (AR) is the third most common cause of pediatric office visits and the fifth most common disorder amongst those under 46 years of age [8,9]. These prominent factors are reflected in significant associated medical expenses [6]. 25.3 million patients (18.5 million adults and 6.8 million children) have been diagnosed with allergic rhinitis in recent years [5]. Over 13.4 million visits to hospital outpatient departments, emergency departments and physicians’ offices were attributed to allergic rhinitis. The total direct and indirect cost of allergic rhinitis was recently estimated to be $5.3 billion per year. A 2011 analysis determined patients with allergic rhinitis averaged 3 additional office visits, 9 more prescriptions filled, and $1500 in incremental health care costs in one year compared to similar patients without allergic rhinitis [10-13]. These numbers are staggering and the estimated economic health care costs are in the billions of dollars. A method to accurately diagnose allergic disease is desperately needed at the non-specialty level. Allergic rhinitis often has other accompanying disease etiologies further adding to the financial health care costs. (Figure 1) The FP often is the entrance to the health care system for these patients. A correct diagnosis becomes tantamount to lowering these costs and deciding if specialty referrals are warranted. Skin testing for IgE mediated disease can be done safely in the Family Practice office, providing needed diagnostic capabilities for atopic disease in the primary care setting. A definitive allergic rhinitis diagnosis is dependent upon the combination of SPT, structured allergy history and physical exam. Relying on history or SPT alone, patients may be misdiagnosed [14].SPT is the defining tool for assessing allergic disease and should be made available to a larger patient population through PC. We report the safety of SPT in the PC office setting utilizing the specific UAS protocol. We believe SPT can be both safely and efficiently utilized in the FP center.
United Allergy Services (UAS) is a health care services company which provides diagnostic skin testing and immunotherapy solutions to physicians throughout in the United States. SPT is currently being utilized in FP offices in approximately 30 states utilizing the UAS methodology. The protocols, patient screening guidelines, decisions, and choices of therapy are under the auspices of the Family Practitioner and are in accordance with current recommendations [3]. All patients were tested previously suspected of seasonal and/or perennial allergic rhinitis by their FP based on their symptomology, medical history, and physical exam results. These individuals underwent skin testing with one of two multiple headed test devices: 1. ComforTen (Jubilient Hollister-Stier Laboratories, Spokane, WA) or 2. Greer Omni Test (Greer Laboratories, Lenoir, NC). Forty Eight pertinent allergens (chosen by floristic zones, pollen counts and cross reactivity models), negative and positive controls, and standard cutoffs for interpretation were utilized. Standardized allergen extract concentrates were used if available and if not available the strongest allergen extract concentrate dilution was incorporated per the allergen diagnostic practice parameters [3].
Salus IRB (Austin, Texas), an independent review board approved the mining of patient data the UAS database, (SalesForce.com, Inc., San Francisco, CA), utilizing computer search algorithms. Patient records from June 2009 through November 2013 were examined. Patient records were reviewed for skin tests and associated adverse reactions. This collection and storage process is HIPAA compliant and access is both individual and computer restricted and also password protected. Statistical analyses and summaries were performed using SAS v 9.3 (SAS Institute, Inc., Cary, NC). Data were analyzed using Student’s T-test to test for differences in means. Chi-square analyses were used to test for differences between groups, using Fisher’s exact test when appropriate to account for small sample sizes. Equivalency testing versus superiority testing was also used to show a 95% confidence level. 95% confidence interval around the 11.5/100,000 SPT is (11.3-11.7/100,000).
In the 4.5 years studied, 156,335 SPTs were performed on 125,295 patients. The demographics of the patients who experienced SPT related SR is presented in (Table 1). In this population, SR reactions occurred in only 18 patients (Table 1). The rate is 0.0115% SR per 100,000 patients compared to the previously reported 0.015-0.023% SR per 100,000 patients SPT [3].Patients tested with the UAS protocol are similar to the lower reaction rate (p=0.45) and significantly safer than the highest reaction rate (p=0.02).
| Characteristic | Male | Female |
|---|---|---|
| Population, n (%) | 2 (11) | 16 (89) |
| Age, mean y | 17 | 48 |
| Race, n | ||
| White | 1 | 9 |
| Black | 1 | 3 |
| Hispanic | 0 | 1 |
| Unknown | 0 | 3 |
| Asthmatics, n | 0 | 4 |
Table 1: Demographics of Patients with Adverse Events.
SPT for aeroallergens has been the standard diagnostic tool to diagnose IgE disease for well over 100 years. The World Allergy Organization refers to skin testing as the gold standard for diagnosing allergic disease [1]. Numerous studies have verified the sensitivity and specificity of prick/puncture tests for both inhalant and food allergens when correlated with nasal and oral challenges [3].Thus, a diagnostic test to identify IgE mediated disorders’ which is quick, safe, accurate and inexpensive should be welcomed by the FP.
FP’s see the majority of patients with symptoms of AR and often provide care based solely on symptoms and physical exam. An allergy history alone is not sufficient to diagnosis allergic disease and patient’s self- assessments are flawed [15]. Usual treatment prescribed is antihistamines, and at times systemic steroids. If symptoms persist, antihistamines may be rotated or if relief is not achieved, then patients may be referred to Allergy Specialists. This referral can take weeks or months to accomplish. This time delay is largely due to the small number of Allergy Specialists versus patient population needing care (Figure 2). Dr. Richard Weber, president (2012-2013) of the American College of Allergy, Asthma, and Immunology (ACAAI) in the ACAAI newsletter addressed the fact skin testing and immunotherapy were going to become more and more apparent in the non-specialist office [16].
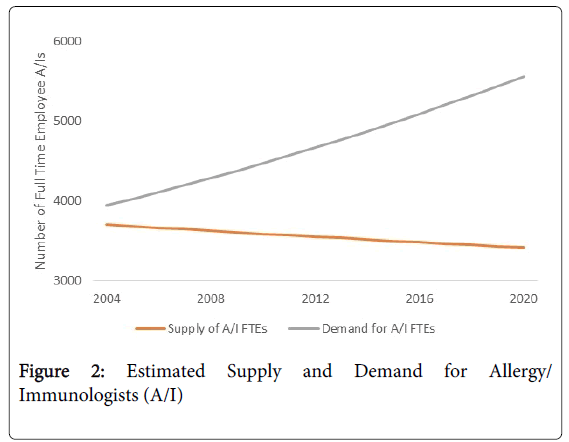
Figure 2: Estimated Supply and Demand for Allergy/ Immunologists (A/I)
Skin testing for IgE mediated disease is a necessary diagnostic tool for the PC physician if they are going to be treating allergic diseases. Settipane et al, clearly state in the American Journal of Rhinology that the only definitive way to differentiate non-allergic rhinitis from allergic rhinitis is with a skin test or in vitro test to seasonal and perennial aeroallergens. Thus, SPT should be utilized to assess and formulate appropriate therapy [17]. The presumptive diagnosis of allergic rhinitis without confirmation of SPT can lead to as many as 65% of these patients being treated with antihistamines or leukotriene receptor antagonists when there is no evident IgE mediated allergic disorder [7].Sibbald et al. demonstrated the need for SPT to properly assess avoidance measures in patients with known or suspected asthma [18]. The 2013 Atopic Dermatitis Practice Parameter indicates SPT to aeroallergens is appropriate in patients who may have an aeroallergen exposure contributing to their atopic dermatitis [19].
In all of these instances, SPT is necessary for accurate diagnosis and treatment. SPT is a safe, proven method for determining allergic disease in the Specialist office and now the same diagnostic tool has been shown, as is evident by our study results, to be safe and effective in the PC physician’s office [20]. Furthermore, our results demonstrate safety results equivalent to that reported by Allergists. Offering SPT's in the primary care setting will provide access to a large number of patients who may otherwise be mistreated, or have a significant wait period for an allergy referral work up. SPT assessment in the primary care setting would promote beneficial economic and health care outcomes. These beneficial outcomes include: diminishing the thousands of dollars spent on over prescribed medication; improving quality of life; and decreasing the number of absent days from school or work due to allergic diatheses. These beneficial consequences would arise from the accurate diagnosis and treatment of AR by utilizing SPT in the FP office. SPT is faster, less expensive, more sensitive, and more easily accomplished than allergen specific IgE serology tests [8,21,22]. Results of allergen specific IgE serology may take up to two weeks to acquire and serologic results may be more difficult to interpret than SPT [1,21,22]. SPT should be utilized to correctly diagnose allergic disease in light of the evidence that two thirds of patients suffering from upper respiratory allergy- like symptoms may be misdiagnosed without utilization of IgE diagnostic tools [7]. SPT is a valuable, reliable diagnostic tool for use in the FP office. Recent FDA approval of two prescription sublingual tablets for Grass allergy and Ragweed allergy will drive the need for SPT in primary care as a confirmed diagnosis by either SPT or RAST is necessary before the sublingual tablets can be prescribed.
One death associated with SPT occurred between 1990 and 2001 and an additional death occurred between 1945 and 1987 [3,4]. These 2 reported deaths have been contrasted with 0 deaths in 125,295 SPT patients reviewed in a primary care setting utilizing the UAS SPT protocols. SPT in the FP arena is a safe means of examining allergic sensitivities to aero allergens. This diagnostic tool has the potential to change prescribing methods for antihistamine usage in presumed but unproven AR; provide vital information in the care of allergic asthmatics and differentiate the diagnosis of AR from non allergic rhinitis [17,18]. Removal of the fear of severe adverse reactions or death from SPT in the primary care setting should allow the FP to feel more comfortable in recommending this service to his or her patients.
“Our nation is facing a critical shortage of certified allergist/ immunologists. Unless action is taken, there will not be enough allergists to treat the growing number of patients who desperately need their care.” The American College of Allergy, Asthma & Immunology [23]. The number of patients is increasing by 35% (by 2020) and few new allergy fellowship training programs are planned currently. The overall outlook for treatment by an allergy specialist is problematic in the future (Figure 2). The sheer future volume of patients needing care for their allergy symptoms, versus specialists available to provide such care, will create a major health care dilemma in future years without some type of intervention in the present. Allowing the FP to evaluate and treat some of these patients should help lessen the burden on the system, provide access to the specialists when deemed medically necessary, and possibly assist in the reduction of asthma in children. The safety of SPT in the FP office is substantiated by the results of this study. Allowing FP physicians to do SPT testing is cost effective and will lessen the burden on the specialists, decrease costs, improve the overall health care of allergic suffers and contribute to better diagnosing millions of patients suffering from sinusitis like symptoms.
This study was reviewed and approved by Salus Independent Review Board (Austin, TX).