Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2014) Volume 4, Issue 2
Background: Retinal vascular occlusion disorders: vein occlusion, central and branch, central arterial occlusion, or branch arterial occlusion as well as anterior ischemic (non arteritic) papillopathy are not rare. They are followed by abrupt decrease of vision acuity, and are complication of different systemic metabolic disorders.
Aim: The aim of this study is to explain possible relationship between inflammatory biomarkers of metabolic syndrome and appearance of retinal vascular net occlusion.
Patients and methods: Prospective case control study was carried on 90 individuals with central retinal vein occlusion, 20 with central arterial retinal occlusion, and 30 with anterior ischemic papillopathy.
The standard ophthalmic examination was obtain, photophundus and fluorescein angiography. Hematological parameters (ESR, WBC, and RBC) and biochemical analysis were done (levels of uric acid, creatinin and urea, plasma fibrinogen level, C reactive protein, glycemia, glycated hemoglobin A1C, total cholesterol, and its fractions, triglycerides). We used National Cholesterol Education Program criteria for metabolic syndrome.
Results: Among examined patients 62(69%) were with CRVO, and 28(31%) with BRVO. Fifty four (60%) patients with vein occlusion meet all criteria for metabolic syndrome. The mean level of glycemia was 8,9 mmol /L, CRP 21mmol/L, total cholesterol 6,7mmol/L, LDL 4,2 mmol/L, triglycerides 1,7 mmol/L and ESR 18 mm/h. Among patients with diagnose of CRAO 12 (60%) and 24 (80%) patients with AION meet the criteria for metabolic syndrome. The mean level of ESR in patients with CRAO was 24/h, glycemia 7,2 mmol /L, CRP 34 mmol/L, cholesterol 7,2 mmol/L, LDL 5,2 mmol/L, and triglycerides 2,7 mmol/L. In patients with AION, the average value of ESR was 20/h, glycaemia 6,9 mmol /L, CRP 54 mmol/L, total cholesterol 8,2 mmol/L, LDL 5,4 mmol/L, and triglycerides 3,0 mmol/L.
Conclusion: Retinal vascular occlusions are not so rare in metabolic syndrome. The CRP is an important parameter in following these conditions, as well as lipid levels, ESR and glycemia and HDL.
Keywords: Retinal vessels; Occlusion; Metabolic syndrome; Inflammation
The entities of Retinal Vascular Occlusion Disorders Obtain: central (CRVO) and Branch (BRVO) Vein Occlusion, Central Arterial Occlusion (CRAO), or branch arterial occlusion as well as Anterior Ischemic (non arteritic) papillopathy (AION) [1,2].
CRVO occurs as a result of thrombosis of the central retinal vein at the level of or posterior to, the lamina cribrosa [1]. BRVO is a term that defines occlusion of one branch of vein [2]. CRAO is occlusion of the central retinal artery at the level of the lamina cribrosa due to thrombus formation in atherosclerosis, emboli, or inflammatory changes in the artery [1,3].
AION is caused by reduced circulation in the short ciliary arteries. These changes of circulation of ciliary arteries may be caused by atherosclerotic changes and in one third of all patients by inflammation [1,3].
The aim of our study was to explain possible relationship between metabolic syndrome and appearance of vascular retinal occlusion disorders.
The prospective study, conducted on Eye Clinic, Clinic Centre in Niš, Serbia, has followed entities of different retinal vascular occlusion disorders. The study obtains 90 patients with CRVO, 20 with retinal CRAO, and 30 with AION. All patients were informed about the methods and the aim of the study and gave their written consent for the participation.
In all patients the standard ophthalmic examination was obtain: best corrected visual acuity, anterior segment examination, and tonometry, posterior segment examination by indirect ophthalmoscopy, photophundus and fluorescein angiography.
Multislice Computed Tomography (MSCT) and Magnet Resonance (MR) of brain were done and excluded space occupying lesions.
Blood laboratory examination obtain hematological parameters Erythrocytes Sedimentation Rate (ESR), White Blood Cells Count (WBC), Red Blood Cells Count (RBC), levels of uric acid, creatinin and urea, plasma fibrinogen level (PF), C reactive protein-(CRP), proteins, glycemia, glycated Hemoglobin A1C (HbA1C), total cholesterol, Low Density Cholesterol (LDLC), High Density Cholesterol HDL-C, and triglycerides. Laboratory examination was performed at Center for Medical Biochemistry, Clinical center Niš, Serbia, on Olympus AU680. The blood samples were taken in early morning hours, before therapy or meal (Figure 1).
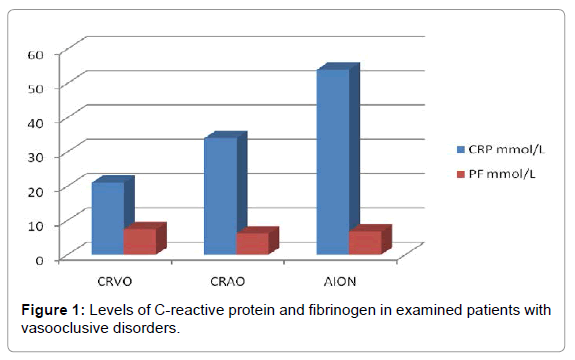
Figure 1: Levels of C-reactive protein and fibrinogen in examined patients with vasooclusive disorders.
Systolic and diastolic blood pressure was measured in morning hours, and expressed in mm/Hg. Body Mass Index (BMI) was calculated, by formula BMI=mass (kg)/(height(m))2 in all examined patients [4]. The Atherogenic Index of Plasma has been calculated by formula Chol- HDL-C/HDL-C [5], and the value of this parameter 2,3 mmol/L was taken as the average value. We used National Cholesterol Education Program (NCEP) criteria metabolic syndrome for diagnose of MetS [6]. According to the NCEP criteria, an individual may be diagnosed to have the MetS if three or more of the following findings are present: abdominal type of obesity, triglycerides more than 1,7 mmol/l, HDL -C < 1.0 mmol/l, blood pressure > 130/85 mmHg, and fasting glucose > 6,1 mmol/l [6-8]. SPSS 16.0 has been used for statistical method, at the level of statistical significance p<0.05. The results are presented in tables and graphics.
Among examined patients 62 (69%) were with CRVO, and 28 (31%) with BRVO. Fifty four (60%) patients with vein occlusion meet all criteria for MetS according to NCEP criteria [6]. The average serum mean level of glycemia in this group of patents was 8, 9 ± 1,26 mmol/L, CRP 21 ± 0.75 mmol/L, total cholesterol 6.7 ± 0.02 mmol/L, LDL-C 4.2 ± 0.04 mmol/L, HDL-C 0.96 ± 0.69 mmol/L, triglycerides 1.7 ± 0.01 mmol/L, PF 7.4 ±1.2 mmol/L and ESR 18 ± 0.2 mm/h (Table 1). The average systolic blood pressure was 140 mm ± 0.2/Hg, and diastolic 90 ± 0.2 mm/Hg.
| Parameter | CRVO (n=45) | CRAO (n=20) | AION (n=30) |
|---|---|---|---|
| Cholesterol (mmol/L) | 6.7 ± 0.2 | 7.2 ± 1.2 | 8.2 ± 1.2 |
| HDL-C (mmol/L) | 0.96 ± 0.69 | 1.0 ± 0.6 | 1.2 ± 0.2 |
| LDL-C (mmol/L) | 4.2 ± 0.4 | 5.2 ± 0.4 | 5.4 ± 0.4 |
| Triglycerides (mmol/L) | 1.7 ± 0.1 | 2.7 ± 0.2 | 3.0 ± 0.4 |
| Glucose (mmol/L) | 8.9 ± 1.26 | 7.2 ± 0.86 | 6.9 ± 1.2 |
| CRP (mmol/L) | 21 ± 0.75 | 34 ± 0.6 | 54 ± 0.7 |
| ESR (mm/h) | 18 ± 0.2 | 24 ± 0.4 | 20 ± 0.1 |
| PF (mmol/L) | 7.4 ± 1.2 | 6.2 ± 0.4 | 6.8 ± 0.4 |
| BMI (kg /m2) | 31.07 ± 4.82 | 30 ± 0.4 | 31.8 ± 0.6 |
| Atherogenic Index | 5.7 ± 1.2 | 5.8 ± 0.4 | 5.7 ± 0.7 |
Table 1: Biochemical parameters in patients with different retinal vascular occlusive disorders.
Among patients with diagnose of CRAO 12 (60%) patients and 24 (80%) patients with AION meets the criteria for MetS. The average value of ESR in patients with CRAO was 24 ± 0.4 mm/h, serum level of glucose 7.2 ± 0.86 mmol /L, CRP 34 ± 0.6 mmol/L, cholesterol 7.2 ± 1.2 mmol/L, LDL-C 5.2 ± 0.4 mmol/L, HDL-C 1.0 ± 0.6 mmol/L, triglycerides 2.7 ± 0.2 mmol/L (Table 1), PF 6.2 ± 0.4 mmol/L. The average systolic blood pressure was 145 ± 0.5 mm/Hg, and diastolic 100 ± 0.2 mm/Hg.
In patients with AION, the average value of ESR in was 20 ± 0.01/h, serum level of glucose 6.9 ± 1.2 mmol/L, CRP 54 ± 0.7 mmol/L, cholesterol 8.2 ± 1.2 mmol/L, LDL-C 5.4 ± 0.4 mmol/L, HDL-C 1.2 ± 0.2 mmol/L, triglycerides 3.0 ± 0.4 mmol/L, PF 6.8 ± 0.4 mmol/L (Table 1). The average systolic blood pressure was 135 ± 0.7 mm/Hg, and diastolic 95 ± 0.2 mm/Hg.
Among examined group of patients with vascular retinal occlusion and Mets the statistical significance was present in comparation of levels of total cholesterol and LDL-C in patients with CRAO and AION according to the levels in patients with CRVO (p<0.05). The levels of this parameter were higher in patients with CRAO and AION. The levels of CRP were higher in group of patients with AION and CRAO than in patients with CRVO and in group of patients with AION than in group with CRAO (p<0.05 AION and CRAO vs. CRVO; p<0.05 AION vs. CRAO). The levels of ESR were higher in patients with CRAO than in patients with AION and CRVO (p<0.05 CRAO vs. CRVO and CRAO vs. AION). The levels of triglycerides were significantly higher in group of patients with CRAO and AION in cooperation to the group with CRVO (p<0.05 AION and CRAO vs. CRVO).
The Atherogenic Index of Plasma was elevated in all groups of examined patients and presented in Table 1 for all groups of patients. Among examined group of patients the statistical significance in comparation of levels of this parameter was not present (p>0.05) (Figure 2).
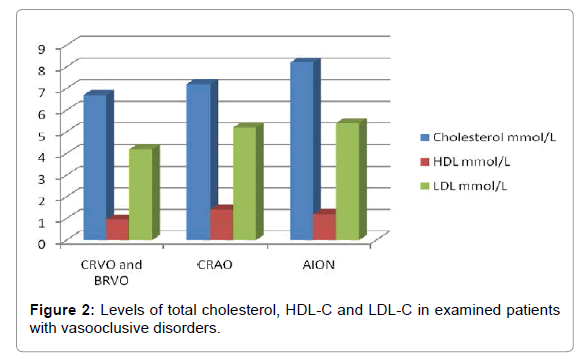
Figure 2: Levels of total cholesterol, HDL-C and LDL-C in examined patients with vasooclusive disorders.
Abrupt, in the most cases unilateral visual loss is a symptom of retinal vascular occlusive disorder. AION, CRAO and CRVO may be caused by complex metabolic changes [1].
According to the NCEP criteria, an individual may be diagnosed to have the MetS if she or he has three or more of the following findings: abdominal type of obesity, triglycerides more than 1.7 mmol/l, HDL -C <1.0 mmol/l, blood pressure >130/85 mmHg, and fasting glucose > 6.1 mmol/l [6-8].
The MetS seems to have 3 potential etiological categories: obesity and disorders of adipose tissue; insulin resistance; and a constellation of independent factors (eg, molecules of hepatic, vascular, and immunologic origin) that mediate specific components of the MetS [9-11]. Other factors—aging, proinflammatory state, and hormonal changes—have been implicated as contributors as well [12-14].
Abdominal obesity is the form of obesity most strongly associated with the MetS [8, 4]. BMI is often used for evaluation of obesity. Obesity contributes to hypertension, high serum cholesterol, low HDL cholesterol, and hyperglycemia. Excess adipose tissue releases several products that apparently exacerbate these risk factors. They include Nonesterified Fatty Acids (NEFA), cytokines, Plasminogen Activator Inhibitor (PAI)-1, and adiponectin [14,15]. High CRP levels accompanying obesity may signify cytokine excess and a proinflammatory state [14]. An elevated PAI-1 contributes to a prothrombotic state.
Insulin resistance is present in the majority of people with the MetS [16]. It strongly associates with other metabolic risk factors and correlates with Cardiovascular Disease (CVD) risk. These associations account for the term insulin resistance syndrome. Insulin resistance generally rises with increasing body fat content, yet a broad range of insulin sensitivities exists at any given level of body fat. Most people with categorical obesity (Body Mass Index [BMI] ≥ 30 kg/m2) have postprandial hyperinsulinemia and relatively low insulin sensitivity. However, weight gain seems to enhance insulin resistance and MetS [6,15]. Dissociation of obesity and primary insulin resistance in patients with MetS is difficult.
Dyslipidemia was very significant in our patients, and atherogenic index as a risk factor for atherosclerosis was increased (Table 1) [6,15]. Atherogenic dyslipidemia manifests in routine lipoprotein analysis by raised triglycerides and low concentrations of HDL-C. A more detailed analysis usually reveals other lipoprotein abnormalities, eg, increased remnant lipoproteins, elevated apolipoprotein B, small LDL-C particles, and small HDL-C particles. All of these abnormalities have been implicated as being independently atherogenic [17].
Atherogenic Index of Plasma (AIP) has been used by some practitioners as a significant predictor of atherosclerosis and indirect parameter of inflammation. The levels of this parameter were elevated in all patients with retinal vascular occlusions.
Blood pressure, systolic as well as diastolic was elevated in all groups of examined patients. Most of them had an anamnesis of previous hypertension. Elevated blood pressure strongly associates with obesity and commonly occurs in insulin-resistant persons. Hypertension is listed among metabolic risk factors. However, some investigators believe that hypertension is less “metabolic” than other metabolicsyndrome components. Certainly hypertension is multifactorial in origin.
A proinflammatory state, recognized clinically by elevations of CRP, is commonly present in persons with MetS. Multiple mechanisms seemingly underlie elevations of CRP. One cause is obesity, because excess adipose tissue releases inflammatory cytokines that may elicit higher CRP levels [18,19].
A prothrombotic state, characterized by increased plasma PAI-1 and PF, also associates with the MetS. PF, an acute-phase reactant like CRP, rises in response to a high-cytokine state. Thus, prothrombotic and proinflammatory states may be metabolically connected [16,18,19].
In all groups, of examined patients with retinal vascular occlusion disorders and MetS, PF, CRP and ERS were increased and suggest an inflammatory component of MetS. The levels of CRP were higher in group of patients with AION and CRAO than in patients with CRVO and in group of patients with AION than in comparation to group with CRAO. CRP levels are more sensitive biomarker for retinal occlusion of small retinal arteries than veins.
Retinal vascular occlusions are not so rare. The visual loss may be severe. Etiology of retinal vascular occlusions is various and often needs multidisciplinary approach. It is closely associated with MetS.
There are suggestions that inflammation might be important triggering mechanism for different vascular occlusion (retinal, CDV, stroke) and MetS. The CRP, PF and HDL are an important parameter in following these conditions.