Angiology: Open Access
Open Access
ISSN: 2329-9495
ISSN: 2329-9495
Research Article - (2018) Volume 6, Issue 3
Objective: To investigate the predictive value of preoperative urinary microalbumin to creatinine ratio (UACR) level for early diagnosis of contrast-induced nephropathy (CIN).
Methods: A total of 180 patients scheduled to undergo elective coronary angiography (CAG)/percutaneous coronary intervention (PCI) in our department from November 2016 to September 2017 were selected into this prospective study. Patients were allocated to high UACR group (UACR ≥ 30, n=35) and control group (UACR<30, n=145) according to the UACR level. The patients were also divided into CIN group (n=32) and no CIN group (n=148). Multivariable logistic regression model was used to investigate the risk factors of CIN. This trial was registered on the Chinese Clinical Trial Registry on 23 May 2017 (Registration No. ChiCTR-OOC-17011467).
Results: 32 patients developed CIN (17.78%). The incidence of CIN was significantly higher in high UACR group than in the control group (P0.001). The ratio of high UACR in CIN group was significantly higher than no CIN group (P0.001). Multivariable logistic regression analysis indicated that preoperative UACR level (P0.001, 95%CI: 3.81929.223, OR: 10.564) was an independent risk factor of CIN.
Conclusion: Preoperative UACR level appears to be an independent predictive factor for early diagnosis of CIN.
Keywords: Urinary microalbumin to creatinine ratio; Coronary angiography; Percutaneous coronary intervention; Contrast-induced nephropathy; Early diagnosis
With the rapid development and pervasive application of imaging diagnosis and treatment techniques such as contrast-enhanced CT, angiography and interventional therapy, the application of contrast medium is increasing in the clinic. Contrast-induced nephropathy (CIN), known as contrast-induced acute kidney injury (CI-AKI), is a common complication after using contrast medium during coronary angiography (CAG), percutaneous coronary intervention (PCI) or other diagnostic and interventional therapy [1]. With an everincreasing number of patients receiving intravascular injection of iodinated contrast medium worldwide, CIN has gradually become the third leading cause of iatrogenic acute kidney injury, right after renal hypoperfusion and nephrotoxic drugs, accounts for about 11% [2,3]. The pathogenesis of CIN may include direct toxicity of contrast medium, renal medulla ischemia and hypoxia, oxidative stress, renal tubular obstruction, etc. [4,5]. Nowadays we have discovered that some biomarkers can be used for accurate identification of high-risk patients and early diagnosis of CIN, like cystatin C (Cys C), neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), interleukin-18 (IL-18), liver-type fatty acid-binding protein (L-FABP), renalase and so on [6-9]. Urinary microalbumin to creatinine ratio (UACR) is one of the early predictors of renal impairment, widely used amang people with hypertension or diabetes mellitus to assess renal function. The purpose of this prospective study was to discover the relationship between UACR and the incidence of CIN, to investigate the predictive value of preoperative level of UACR for early diagnosis of CIN after CAG/PCI. The trial is registered on the Chinese Clinical Trial Registry on 23 May 2017(Registration No. ChiCTR-OOC-17011467).
Objects of study
From November 2016 to September 2017, a total of 180 patients underwent CAG/PCI in our department were selected into this study, including 121males and 59 females. Among them, the oldest aged 89 years, the youngest aged 34 years, aged 66.88 ± 10.42 years on average. 126 of them had hypertension history and 70 of them had diabetes mellitus. Inclusion criteria: (1) 18-90 years old; (2) scheduled to undergo CAG/PCI. Exclusion criteria: (1) history of allergy to contrast medium; (2) concomitant of severe heart failure, severe valvular heart disease, hemodynamic instability, and unable to lie for over 24 hours; (3) receiving contrast medium for examinations including contrastenhanced CT, MRI or CTA in the past 2 weeks; (4) acute kidney injury or using nephrotoxic medications within 2 weeks recently, including aminoglycosides, amphotericin B and Chinese medicine containing aristolochic acids ; (5) concomitant of severe liver dysfunction, renal dysfunction (CKD stage 4 to 5, eGFR30ml/(min 1.73 m2); (6) concomitant of cancer, fever, infectious diseases, thyroid dysfunction, and coagulation disorders; (7) pregnancy or lactation; (8) noncompliance of treatment or incoordination of examination. This study was approved by the Ethics Committee of Zhongda Hospital affiliated to Southeast University and all the patients gave informed consent.
Diagnostic criteria
The diagnosis of CIN refers to the criteria defined by the European Society of Urogenital Radiology (ESUR) in 2011: an impairment of renal function (usually defined as either an increment of at least 0.5 mg/dl (44.2 mol/L) in serum creatinine concentrations or an increase of 25% or more in serum creatinine concentrations from the baseline) occurred within 48 to 72 hours after intravascular administration of contrast medium, with the exclusion of other causes [10,11]. The division of chronic renal insufficiency (CKD) is based on the estimated glomerular filtration rate (eGFR), calculated by the formula of Modification of Diet in Renal Disease (MDRD) [12], as eGFR =175 × serum creatinine -1.234 × age -0.179, and women multiplied by 0.79.
Methods of study
The clinical baseline data of the selected patients were recorded. All patients were divided into 3 groups due to body mass index (BMI), including BMI24.00 kg/m2, 24.00 kg/m2 ≤ BMI28.00 kg/m2, and BMI ≥ 28.00 kg/m2. Blood samples were tested routinely to measure preoperative baseline serum creatinine, urea nitrogen, leukocyte count, hemoglobin, total cholesterol, triglycerides, and LDL-Cholesterol and other clinical parameters. The urine was collected to test UACR before operation at the same time. Renal function was measured within 48 to 72 hours after operation. Antiplatelet drugs, beta blockers, angiotensin converting enzyme inhibitors (ACEI) or angiotensin II receptor blockers (ARB), calcium channel blockers (CCB), spironolactone and statins were administrated appropriately according to the condition of patients by clinician. The function of heart and kidney was considered to decide whether to conduct hydration therapy. A load amount of aspirin 300 mg and clopidogrel 300mg was given before operation. Seldinger puncture method was used for the operation. The puncture position was radial artery or femoral artery. The decision of whether further treatment was needed was made according to the results of coronary angiography, and the time of operation was not limited. Nonionic low-osmotic or isosmotic contrast medium was administrated, including iopromide (Bayer, Germany), iodixanol (General Electric, America).The volume of contrast medium was recorded during the procedure.
Statistical analysis
SPSS software (version 18.0) was used for analysis. Continuous variables were presented as mean±standard deviation, if normally distributed and as median (interquartile range) if not normally distributed. Student’s t-test or Wilcoxon W test, where appropriate, was used for comparison between groups. Categorical variables were expressed by percentages, and chi-square test or Fisher exact test where appropriate, was used for comparison between groups. Logistic regression model was used to analyze the risk factors of CIN. Variables included in multivariate analysis were determined according to clinical experience and professional knowledge. Receiver operator characteristic curve (ROC curve) was used to calculate the cut-off point of UACR for predicting CIN and the sensitivity and specificity of this point. Double-sided test was applied, and a P value less than 0.05 were considered statistically significant.
Comparison of clinical data between high UACR group and control group
Patients were divided into 2 groups according to the UACR level: high UACR group (UACR≥ 30, n=35) and control group (UACR30, n=145). Factors like level of preoperative serum creatinine, urea nitrogen, leukocyte count, amount of lesions and implanted stents were significantly higher in UACR group than control group, and preoperative eGFR was significantly lower than control group (P0.05). The proportion of male, hypertension, diabetes, cardiac dysfunction, the use of spironolactone, multi-vessel coronary disease, multi-stent implantation and hydration therapy were significantly higher than that in control group (P0.05). The incidence of CIN in high UACR group was significantly higher than control group (45.71% (16/35) to 11.03% (16/145), P0.001). There was no statistically significant difference between two groups in aspects including age, BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), erythrocyte count, hemoglobin, platelet count, total cholesterol, triglycerides, LDLCholesterol and volume of contrast medium (P0.05) (Table 1).
| Control Group (n=145) | High UACR Group (n=35) |
P | |
|---|---|---|---|
| Age (years) | 66.60 ± 9.74 | 68.03 ± 12.99 | 0.468 |
| Male (%) | 93 (64.14) | 28 (80.00) | 0.073 |
| BMI (kg/m²) | 25.41 ± 3.52 | 24.90 ± 4.03 | 0.775 |
| BMI groups (%) | 0.191 | ||
| Group 1 (BMI<24.00) | 46 (31.72) | 14 (40.00) | |
| Group 2 (24.00 ≤ BMI<28.00) | 74 (51.04) | 12 (34.29) | |
| Group 3 (BMI ≥ 28.00) | 25 (17.24) | 9 (25.71) | |
| SBP (mmHg) | 135.28 ± 17.34 | 136.43 ± 18.12 | 0.598 |
| DBP (mmHg) | 78.17 ± 11.93 | 77.20 ± 11.13 | 0.650 |
| Hypertension (%) | 96 (66.21) | 30 (85.71) | 0.024 |
| Diabetes (%) | 51 (35.17) | 19 (45.71) | 0.037 |
| Previous myocardial infarction (%) | 13 (8.97) | 2 (5.71) | 0.776 |
| Atrial fibrillation (%) | 7 (4.83) | 2 (5.71) | 1.000 |
| Cardiac insufficiency (%) | 0 (0.00) | 3 (8.57) | 0.007 |
| Preoperative serum creatinine (mmol/L) | 76.68 ± 17.44 | 92.26 ± 25.87 | 0.002 |
| Preoperative eGFR(ml/(min 1.73 m2)) | 73.79 ± 17.70 | 61.56 ± 20.32 | 0.001 |
| Preoperative urea nitrogen (mmol/L) | 5.75 ± 1.46 | 6.51 ± 2.00 | 0.045 |
| Leukocyte count (×109/L) | 6.51 ± 1.86 | 7.58 ± 2.37 | 0.014 |
| Erythrocyte count (×1012/L) | 4.51 ± 0.47 | 4.55 ± 0.70 | 0.861 |
| Hemoglobin (g/L) | 137.50 ± 14.05 | 136.83 ± 20.87 | 0.858 |
| Platelet count (×109/L) | 195.74±60.28 | 210.34 ± 85.21 | 0.393 |
| Total cholesterol (mmol/L) | 4.29 ± 1.18 | 4.10 ± 1.06 | 0.371 |
| Triglycerides (mmol/L) | 1.66 ± 1.69 | 1.87 ± 1.81 | 0.688 |
| LDL-Cholesterol (mmol/L) | 2.57 ± 0.99 | 2.28 ± 0.79 | 0.175 |
| UACR | 7.73 ± 5.36 | 415.59 ± 774.41 | <0.001 |
| Perioperative medication (%) | |||
| Aspirin | 129 (88.97) | 32 (91.43) | 0.905 |
| Beta blockers | 115 (79.31) | 28 (80.00) | 0.928 |
| ACEI or ARB | 72 (49.66) | 23 (65.71) | 0.088 |
| CCB | 50 (34.48) | 16 (45.71) | 0.216 |
| Statins | 141 (97.24) | 35 (100.00) | 1.000 |
| Spironolactone | 12 (8.28) | 9 (25.71) | 0.010 |
| Digoxin | 1 (0.69) | 1 (2.86) | 0.352 |
| Volume of contrast medium (ml) | 95.42 ± 58.20 | 100.16 ± 56.33 | 0.312 |
| Number of coronary artery lesions | 1.42 ± 1.10 | 1.86 ± 1.11 | 0.037 |
| Multi-vessel coronary disease (%) | 65 (44.83) | 23 (65.71) | 0.027 |
| Amount of lesions and implanted stents | 0.63 ± 0.81 | 1.06 ± 1.14 | 0.045 |
| Multi-stent implantation (%) | 23 (15.86) | 12 (34.29) | 0.013 |
| Hydration (%) | 108 (74.48) | 32 (91.43) | 0.03 |
| CIN (%) | 16 (11.03) | 16 (45.71) | <0.001 |
Table 1: Comparison of clinical data between high UACR group and control group.
Comparison of clinical data between CIN group and no CIN group
32 of the 180 patients developed CIN, accounting for 17.78%. The patients were divided into CIN group (n=32) and no CIN group (n=148). The preoperative UACR level, the proportion of the use of spironolactone and digoxin, multi-vessel coronary disease in CIN group were significantly higher than that in no CIN group (P0.05). There was no significant difference between two groups in other factors (P0.05). The proportion of high UACR level in CIN group was significantly higher than the other (50.00% (16/32) to 12.84% (19/148), P0.001) (Table 2).
| no CIN group (n=148) | CIN group (n=32) | P value | |
|---|---|---|---|
| Age (years) | 66.94 ± 9.73 | 66.59 ± 13.35 | 0.890 |
| Male (%) | 99 (66.89) | 22 (68.75) | 0.839 |
| BMI (kg/m²) | 25.43 ± 3.51 | 24.75 ± 4.07 | 0.320 |
| BMI groups (%) | 0.615 | ||
| Group 1 (BMI<24.00) | 47 (31.75) | 13 (40.63) | |
| Group 2 (24.00 ≤ BMI<28.00) | 72 (48.65) | 14 (43.75) | |
| Group 3 (BMI ≥ 28.00) | 29 (19.60) | 5 (15.62) | |
| SBP (mmHg) | 134.79 ± 17.30 | 138.81 ± 18.02 | 0.357 |
| DBP (mmHg) | 77.34 ± 11.59 | 80.63 ± 12.37 | 0.204 |
| Hypertension (%) | 100 (67.57) | 26 (81.25) | 0.155 |
| Diabetes (%) | 55 (37.16) | 15 (46.88) | 0.307 |
| Previous myocardial infarction (%) | 13 (8.78) | 2 (6.25) | 0.906 |
| Atrial fibrillation (%) | 6 (4.05) | 3 (9.38) | 0.421 |
| Cardiac insufficiency (%) | 2 (1.35) | 1 (3.13) | 0.446 |
| Preoperative serum creatinine (mmol/L) | 79.43 ± 17.36 | 80.97 ± 30.62 | 0.382 |
| Preoperative eGFR(ml/(min 1.73 m2)) | 71.30 ± 17.73 | 71.93 ± 23.53 | 0.725 |
| Preoperative urea nitrogen (mmol/L) | 5.86 ± 1.61 | 6.08 ± 1.59 | 0.422 |
| Leukocyte count (×109/L) | 6.66 ± 1.96 | 7.00 ± 2.23 | 0.334 |
| Erythrocyte count (×1012/L) | 4.52 ± 0.46 | 4.51 ± 0.74 | 0.521 |
| Hemoglobin (g/L) | 137.70 ± 14.24 | 135.81 ± 20.75 | 0.626 |
| Platelet count (×109/L) | 197.29 ± 61.44 | 204.56 ± 84.23 | 0.999 |
| Total cholesterol (mmol/L) | 4.21 ± 1.19 | 4.46 ± 1.01 | 0.264 |
| Triglycerides (mmol/L) | 1.58 ± 0.97 | 2.26 ± 3.46 | 0.732 |
| LDL-Cholesterol (mmol/L) | 2.51 ± 0.99 | 2.57 ± 0.84 | 0.505 |
| UACR | 27.58 ± 97.75 | 362.00 ± 817.89 | <0.001 |
| High UACR (%) | 19 (12.84) | 16 (50.00) | <0.001 |
| Perioperative medication (%) | |||
| Aspirin | 131 (88.51) | 30 (93.75) | 0.578 |
| Beta blockers | 113 (76.35) | 28 (87.50) | 0.165 |
| ACEI or ARB | 75 (50.68) | 20 (62.50) | 0.297 |
| CCB | 55 (37.16) | 11 (34.38) | 0.767 |
| Statins | 144 (97.30) | 32 (100.00) | 1.000 |
| Spironolactone | 13 (8.78) | 8 (25.00) | 0.022 |
| Digoxin | 0 (0.00) | 2 (6.25) | 0.031 |
| Volume of contrast medium (ml) | 96.20 ± 56.32 | 98.31 ± 57.14 | 0.231 |
| Number of coronary artery lesions | 1.46 ± 1.11 | 1.71 ± 1.13 | 0.169 |
| Multi-vessel coronary disease (%) | 67 (45.27) | 21 (65.63) | 0.037 |
| Amount of lesions and implanted stents | 0.69 ± 0.85 | 0.81 ± 1.08 | 0.590 |
| Multi-stent implantation (%) | 28 (18.92) | 7 (21.88) | 0.702 |
| Hydration (%) | 113 (76.35) | 27 (84.38) | 0.322 |
Table 2: Comparison of clinical data between CIN group and no CIN group.
Multivariable logistic regression analysis of risk factors related to CIN
Combined with single factor of statistical results, clinical and professional knowledge, Possible risk factors, such as age, gender, groups of BMI, complications (hypertension, diabetes, pre-existing myocardial infarction, atrial fibrillation, cardiac insufficiency), laboratory examination indicators (including preoperative eGFR, urea nitrogen, divisions of UACR level, etc.), multiple lesions, perioperative medication (aspirin, beta blockers, ACEI/ARB, CCB, spironolactone, digoxin), hydration therapy were all included in logistic regression. The logistic regression revealed that preoperative eGFR (P=0.01, 95%CI: 1.008˜1.063, OR: 0.935) and UACR (P0.001, 95%CI: 3.819˜29.223, OR: 10.564) were independent risk factors of CIN (Table 3).
| Variable | β | SE | Wals | P | Odds Ratio | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| Upper Limit | Lower Limit | ||||||
| Preoperative eGFR | -0.035 | 0.014 | 6.567 | 0.010 | 0.935 | 1.008 | 1.063 |
| High UACR | 2.357 | 0.519 | 20.621 | <0.001 | 10.564 | 3.819 | 29.223 |
| Beta blockers | 1.250 | 0.666 | 3.525 | 0.060 | 3.489 | 0.947 | 12.864 |
| Spironolactone | 1.085 | 0.794 | 1.867 | 0.072 | 2.959 | 0.624 | 14.022 |
Table 3: Multivariable logistic regression analysis of risk factors related to CIN
Analysis of ROC curve
UACR was used in ROC curve to determine the cut-off for the prediction of CIN. The area under the ROC curve of UACR was 0.718 (95%CI: 0.605~0.831, P<0.001), with statistically significant difference. When UACR was 47.08, the sensitivity was 50.0% and the specificity was 93.9% (Figure 1).
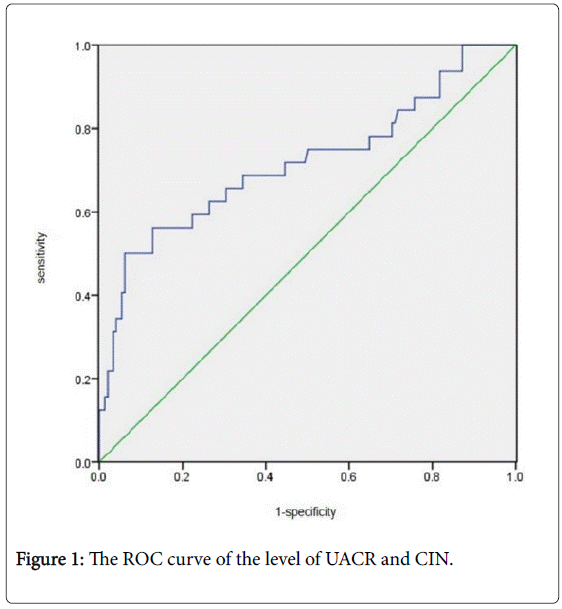
Figure 1: The ROC curve of the level of UACR and CIN.
CIN is one of the serious complications after receiving intravascular injection of contrast medium. Emerging evidence has shown a significant increase in short-term and long-term mortality in patients developed CIN, compared with those without CIN. In addition, the history of CIN may also be related to the development of chronic renal disease and the long-term development of end-stage renal disease [13]. Previous studies have discovered that CAG and PCI are most closely related to the occurrence of CIN. The prevention and early intervention of CIN are partly limited because of the lack of early prediction of biological markers to identify high-risk patients [2,14].
A large number of studies have shown that the incidence of CIN in general population is lower than 1%, while in high-risk groups (preexisting chronic kidney disease, diabetes, hemodynamic instability, acute myocardial infarction, excessive application of contrast medium, renal toxicity drugs, advanced age, etc.), the risk of developing advanced cardiovascular events, dialysis and death at the end of chronic kidney disease increases significantly. Similar to the results of other epidemiological studies, the incidence of CIN in our study is 17.78% [15].
Nowadays, the most accepted definition of CIN is formulated according to the level of serum creatinine. However, the level of serum creatinine is not a reliable indicator during the period of acute kidney injury, and the variation of serum creatinine is not sensitive and specific enough for small changes in glomerular filtration rate. In addition, serum creatinine could be influenced by many factors, such as age, gender, race, intravascular volume and so on [16]. Urinary microalbumin is a sensitive index reflecting the permeability of glomerular capillaries, used for early evaluation of diabetic nephropathy and hypertensive nephropathy. In the past, people detected urinary microalbumin through the urine of 24 hours or night time (8 hours) to calculate the excretion rate of urinary microalbumin, but the subsistence of sample was troublesome and time consuming. The output of urinary microalbumin is basically constant in normal condition or when the kidney was mildly damaged. Creatinine is mainly filtered through glomerulus, which is excreted in the renal tubule with rarely reabsorbed, and the output also remains constant when the kidney is normal or mildly damaged.
In addition, the excretion of urinary microalbumin and creatinine is affected by the same factors, so the ratio of both is relatively constant, thus avoiding the one-side effect of single index [17]. And the method of collection is simple and fast. Jones and Viberti have found that UACR can predict the risk of cardiovascular events directly in diabetic patients. The HOPE study found that urinary microalbumin is closely associated with the incidence of cardiovascular events in patients with hypertension. Currently, UACR is widely recognized as an independent predictor of cardiovascular events [18,19]. Guo et al. found that age, SBP and eGFR were all risk factors for UACR [20]. Our study found that the level of preoperative serum creatinine, urea nitrogen, the proportion of hypertension, diabetes were significantly higher in UACR group than control group, and eGFR was lower than control group, consistent with the level of UACR. The multivariate logistic regression analysis showed that preoperative level of UACR was one of the independent risk factors of CIN. Our study revealed that patients with high UACR level developed a higher risk of CIN, compared to those with low UACR, and prevention should be strengthened at an early stage.
Pre-existing renal insufficiency with reduced nephron capacity is now recognized as the most important and independent risk factor for CIN [21], which is associated with oxidative stress, decline of kidney compensatory ability, extension of residence time of contrast medium in kidney, direct toxic effect of contrast medium on renal tubules and so on [4,5]. Our study found that preoperative eGFR was also an independent risk factor for CIN (P0.05, OR=0.935), which suggests that the risk of developing CIN is higher with lower eGFR. The level of creatinine can reflect renal function indirectly through eGFR. A study on pharmacokinetics of iomeprol in vivo showed that people with normal renal function discharge 50% given dose of contrast medium need 2 hours, while those with severe chronic kidney disease need 16 to 84 hours. Chronic kidney disease can make renal tubular damage worse, as the compensatory mechanism of kidney is limited, few renal units with normal function need to metabolize overload contrast medium, which will cause the extension of residence time of contrast medium in kidney and aggravate damage on renal tubules.
In addition, the widely recognized risk factors of CIN at present also include age, diabetes, congestive heart failure, severe hypovolemia, dehydration, long-term sustained hypotension, multiple myeloma, osmotic pressure, volume and using interval time of contrast medium, etc. [21,22]. Our study have ruled out the objects with obvious hemodynamic instability, but we still did not find any significant difference in factors like diabetes and age between groups of CIN and no CIN, which means further more studies are needed.
Studies have shown that intravenous hydration therapy is the most effective strategy to prevent CIN [11,13]. The ESC guidelines indicated that preoperative hydration is recommended to prevent CIN, in addition to limiting the amount of contrast medium and the use of isotonic or hypoisotonic contrast medium. Similarly, the KDIGO clinical guidelines recommend that patients with high risk of CIN should be treated with normal saline or sodium bicarbonate solution before operation to prevent CIN. In this study, there was no significant difference in hydration treatment between CIN group and no CIN group, and no significant protection of hydration was found in multivariate Logistic regression analysis. We speculated that this might be related to the situation that most of the patients were taken hydration in our study, which made the condition of hydration matched between two groups.
The limitations of our study mainly include: (1) This study is a single-center prospective observational study. In the process of inclusion, some patients were excluded due to incoordination with examination, which caused a selection bias. (2) Because of the small sample size, the dispersion of UACR level among patients was large, resulting in the instability of results. (3) Some uncertain confounding factors might not be adjusted while conducting multivariate logistic regression analysis. Our study showed that there is a correlation between UACR and CIN and UACR is an independent risk factor of CIN. However, due to the shortcomings of this study, more multicenter prospective randomized controlled trials on a larger scale are needed to further confirm the relationship between UACR and CIN.
In summary, our single-center prospective study reveals that preoperative UACR level could be an independent predictive factor for early identification of high-risk patients and diagnosis of CIN. The risk of incidence of CIN is higher in patients with high levels of UACR. Obviously, early intervention should be conducted to help reducing the occurrence of CIN, and lowering the mortality rate ultimately. Therefore, UACR may be a promising early biomarker to prevent CIN in the future.
The authors declare that there are no conflicts of interest regarding the publication of this article.
This study was supported by the National Natural Science Foundation of China (grant no. 81600227).