Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2016) Volume 5, Issue 1
Endometriosis is a common benign gynecological disease in women of reproductive age with a variety of clinical presentations ranging from asymptomatic to intractable and intolerance. Intestinal involvement occurs in 3% to 37% of patients with pelvic endometriosis, and rectosigmoid colon is the most frequently involved site [1]. Involvement of the gastrointestinal tract may mimic primary gastrointestinal carcinoma. Bowel obstruction is rare because it usually involves the serous layer, sparing the mucosa. We report a case of a 43-year-old woman presented with gastrointestinal symptoms of bowel obstruction as the first manifestation of disease and highlight the diagnostic difficulty.
<Keywords: Intestinal endometriosis, Endometriosis, Colon cancer, Bowel obstruction
A previously healthy 43-year-old woman suffered from bowel habit change for months. Initially, she was diagnosed as irritable bowel syndrome and treated at a local medical clinic. The physical examination found normal vital signs, and examination of the abdomen was normal. Colonoscopy indentified a sigmoid ulcerative mass lesion (Figure 1) and tubular adenoma was diagnosed by the histological examination of the endoscopic biopsy specimen. Abdominal computed tomography (CT) showed annular mural thickening of the wall of the rectosigmoid colon, about 4.1 cm in length (Figures 2 and 3). Sigmoid colon cancer was suspected and a laparoscopic assisted low anterior resection of the rectum was planned. At surgery, upper rectal tumor with partial obstruction and right ureter partial obstruction were noted. Frozen section biopsy results showed atypical glands, favored benign, much to the surprise of the treating team. The surgical procedure started with a low anterior resection of the rectum, ending with an end to end colorectal anastomosis and cystoscopy assisted double-J catheter insertion. The final pathologic results showed endometriosis with rectum involvement in mucosa, submucosal, muscular wall and culde- sac. The one regional lymph node also revealed endometriosis. She was discharged without discomfort 8 days later.
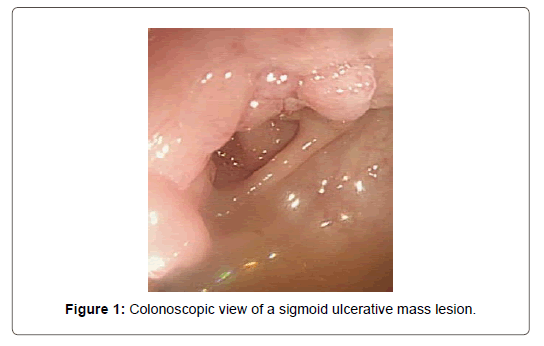
Figure 1: Colonoscopic view of a sigmoid ulcerative mass lesion.
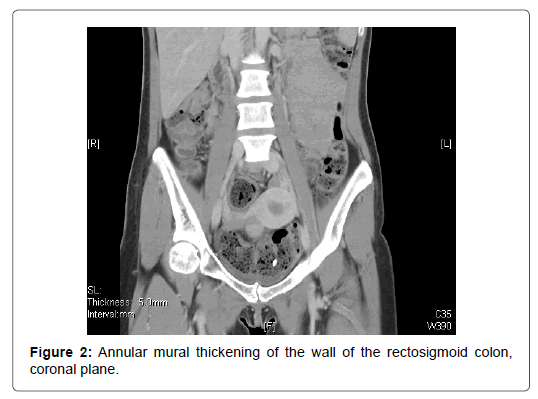
Figure 2: Annular mural thickening of the wall of the rectosigmoid colon, coronal plane.
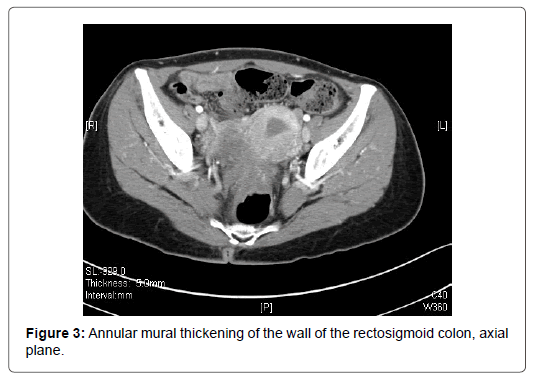
Figure 3: Annular mural thickening of the wall of the rectosigmoid colon, axial plane.
Endometriosis is defined as the presence of endometrial tissue and glands outside the uterine cavity. The most widely accepted theory about the pathogenesis of endometriosis is the retrograde menstruation, which explains the presence of endometrial cells on the peritoneal surfaces [2]. The ovaries are the most affected organs, followed by the uterosacral ligaments, the fallopian tubes, and the bowel [3]. Rectosigmoid colon is the most frequently involved site of intestinal endometriosis (73%), followed by the small bowel and the cecal appendix [4]. Patients with bowel involvement can be asymptomatic or they can present with abdominal pain, constipation, diarrhea, change in the form and caliber of stool, tenesmus and rarely hematochezia. A cyclic pattern of abdominal symptoms that correlates with menstruation supports a diagnosis of endometriosis, but these symptoms are easily mistaken for bowel obstruction caused by adhesions, malignancy, or inflammatory bowel disease. Differentiation of the clinical symptom between intestinal endometriosis and primary gastrointestinal carcinoma is difficult and it is a challenge for physicians to make diagnosis.
Endometriosis most often involves the anterior wall of the rectosigmoid colon, and typically produces extrinsic mass effect on the serosa, with the overlying mucosa left intact. The incidence of mucosal involvement by intestinal endometriosis has been estimated by examination of involved resection specimens to be only 30% [1]. A definitive preoperative diagnosis is sometimes difficult because an endoscopic biopsy has limited efficacy as a diagnostic tool. Recognition of the radiologic appearance of gastrointestinal involvement may be the clue for diagnosis. Endometriosis may manifest as a polypoid mass extending into the lumen of the colon, a stricture or a short annular lesion [5,6] . In these cases, it may be impossible to distinguish endometriosis from carcinoma at radiography. Many cases of intestinal endometriosis are still diagnosed during operation. Because pelvic endometriosis sometimes involves the intestinal tract and mimics a malignant tumor in a female case, an intraoperative histological examination should therefore be considered for conclusive diagnosis during surgery for colorectal cancer.
Treatment options consist of medical and surgical treatment. Most patients are treated medically with hormone therapy to control the cyclic tissue proliferation and bleeding that cause the symptoms. The medications used to treat endometriosis are danazol, highdose progestins, and GnRH agonists, all of which have equivalent efficiency [7]. Laparoscopic or open surgical bowel resection may be necessary in selected patients in whom endometriosis has involved the gastrointestinal tract and caused obstruction or severe bleeding [8]. When it is impossible to differentiate between endometriosis and a neoplasm of the bowel, surgical intervention is also necessary.
In our patient, the atypical presentation included clinical symptoms of bowel obstruction and annular mural thickening lesion at abdominal computed tomography (CT), led to be mistaken as primary gastrointestinal carcinoma. Surgical intervention was necessary in this case because bowel obstruction developed and differentiation between endometriosis and a neoplasm of the bowel was difficult.
Diagnosis of intestinal endometriosis is difficult. Based on clinical symptoms, endoscopic procedure and radiological findings, it can be easily mistaken for malignancy. Familiarity with the pattern of gastrointestinal tract involvement is important for accurate diagnosis. Most patients can be treated medically with hormone therapy, and laparoscopic or open surgery is usually successful if medical management fails.