Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2013) Volume 3, Issue 6
Background: Use of lower tidal volumes during mechanical ventilation is associated with reduced morbidity and mortality of Intensive Care Unit (ICU) patients with the Acute Respiratory Distress Syndrome (ARDS). Use of lower tidal volumes could also protect ICU patients without ARDS. While use of higher tidal volumes is strongly discouraged in ARDS patients, guidelines do not yet recommend on tidal volume size in patients not suffering from this complication, resulting in unwanted variable mechanical ventilation settings amongst ICU patients.
Purpose: The present study aims to determine ventilation characteristics, including tidal volume size in intubated and mechanically ventilated patients in ICUs in Europe, Australia and the Americas. Ventilation characteristics and outcomes are compared among patients without ARDS, patients at risk for ARDS and patients with mild, moderate or severe ARDS.
Methods: The ‘PRatice of VENTilation in critically ill patients without ARDS’ study (PRoVENT) is an international multicenter observational study in critically ill intubated and ventilated ICU patients by the PROVENet (PROtective VENtilation Network) investigators (http://www.provenet.eu/). At least 1,000 patients under invasive mechanical ventilation are included in a time window of 7 days, and followed up to the end of stay in ICU. The primary endpoint is the variability of tidal volume size in ventilated patients in ICUs in Europe, Australia and the Americas.
Conclusion: PRoVENT is designed to investigate and compare tidal volume settings in patients without ARDS, patients at risk for ARDS, and patients with mild, moderate or severe ARDS, and to determine the impact of tidal volume size on important clinical endpoints, in particular patients without ARDS. PRoVENT shall provide information on ventilator settings that could be used in future trials of ventilation, especially in ICU patients without or at risk for ARDS (Trial Registration: NCT01868321).
Mechanical ventilation is a frequently applied and often life–saving strategy in critically ill patients [1]. Paradoxically, ventilation itself has the potential to worsen preexisting lung injury or even cause lung injury [2]. Ventilation–associated lung injury is suggested to result, at least in part through overstretching of aerated lung tissue and tidal recruitment of collapsed lung parts [2]. So-called ‘protective ventilation’ with lower tidal volumes (i.e., tidal volumes of 6 ml/kg Predicted Body Weight (PBW)) aiming at prevention of overstretching of lung tissue is strongly associated with reduced morbidity and mortality of Intensive Care Unit (ICU) patients with the Acute Respiratory Distress Syndrome (ARDS) [3-6], and consequently recommended in international guidelines [7].
Results from one multi–center randomized controlled trial suggest that ICU patients without ARDS could also benefit from protective ventilation with lower tidal volumes [8]. A recent meta–analysis confirmed such claim, showing an increased incidence of pulmonary complications and even increased mortality in patients who receive ‘higher’ or ‘traditionally-sized tidal volumes’ (i.e., tidal volumes of >10 ml/kg PBW) [9]. Whether we should use lower tidal volumes in ICU patients without ARDS remains debatable, since such measure can increase the need for sedation and prolonged use of muscle paralysis, possibly increasing the incidence of delirium, critical illness-associated muscle weakness, and even diaphragm dysfunction [10]. In view of the lack of evidence, guidelines inconsistently advise on tidal volume size in ICU patients without ARDS.
In view of those facts, a large well-powered randomized controlled trial comparing ventilation with lower tidal volumes with ‘conventional ventilation’ using traditionally-sized tidal volumes is needed to answer the question whether ICU physicians should use lower tidal volumes in all ventilated patients, including those without ARDS. Such a trial should not only use relevant clinical endpoints and pay attention to safety of use of lower tidal volumes, but also compare a lower tidal volume strategy to relevant tidal volumes in the control arm. Indeed, lower tidal volumes are increasingly used [3-6], possibly even in patients without ARDS in whom the benefits of lower tidal volumes are less certain. If studies of current practice would show that tidal volumes of >10 ml/kg PBW by now are uncommon, a conventional ventilation arm using tidal volumes of that size may impose a significant health risk of patients in that group, and also may hamper valorization of the trial results.
The PRatice of VENTilation in critically ill patients without ARDS (PRoVENT) study aims to determine ventilation practice and outcomes of intubated and ventilated ICU patients. PRoVENT shall provide information on ventilator settings that can be used in future trials of mechanical ventilation, in particular in patients without or at risk for ARDS.
Design
The PRoVENT study is an international multicenter observational study. The Institutional Review Board of the Academic Medical Center at the University of Amsterdam, Amsterdam, The Netherlands, approved the study and analysis plan. PRoVENT is conducted in accordance with the declaration of Helsinki and is registered at www.clinicaltrials.gov (trial identification number NCT01868321). Due to the strict observational design and anonymous collection of data, informed consent is not needed in most countries-however; in certain countries individual patient informed consent is required according to local IRB regulations. Figure 1 and 2 shows the CONSORT diagram of PRoVENT.
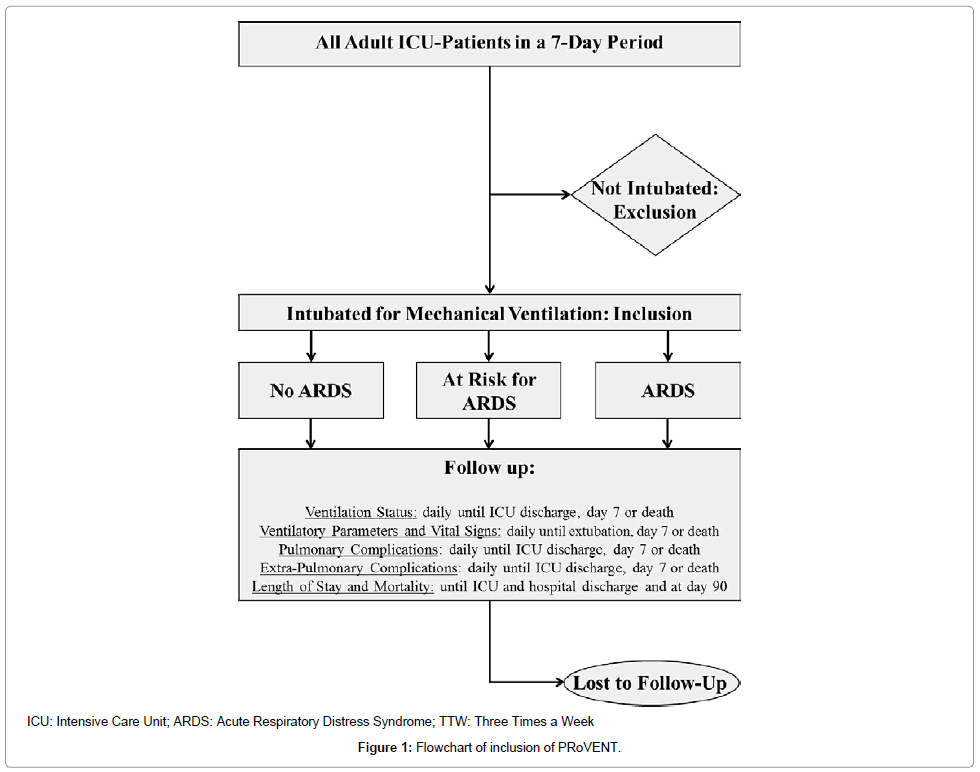
Figure 1: Flowchart of inclusion of PRoVENT.
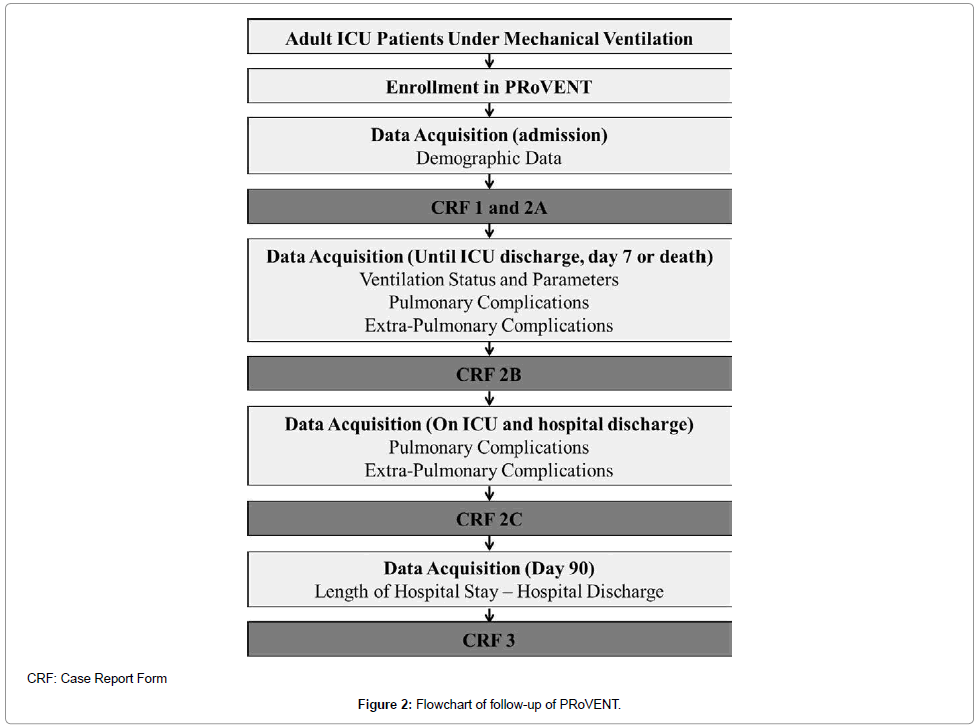
Figure 2: Flowchart of follow-up of PRoVENT.
Study population
Inclusion is not restricted to patients who are intubated for mechanical ventilation in the ICU; Patients who started mechanical ventilation in the emergency room, ward, community or operating room before the present ICU admission are also eligible for participation and should be included. Age <18 years, use of only non-invasive ventilation not followed by invasive ventilation, patients under invasive mechanical ventilation previous to the 7-day period of inclusion, and patients transferred from another hospital under invasive mechanical ventilation represent the main exclusion criteria (Table 1).
| INCLUSION CRITERIA |
| 1. Admitted to a participant ICU |
| 2. Intubated in the participating ICU, ER, ward, community or before the present ICU admission |
| EXCLUSION CRITERIA |
| 1. Age < 18 year |
| 2. Receiving only NIV |
| 3. Under invasive mechanical ventilation previous to the 7-day period of inclusion |
| 4. Transferred from another hospital under invasive mechanical ventilation |
| ICU: Intensive Care Unit; ER: Emergency Room; OR: Operating Room; NIV: Non-Invasive Ventilation |
Table 1: Inclusion and exclusion criteria.
Patients are stratified in three groups for comparison of the primary and secondary endpoints: patients without ARDS, patients without, but at risk for development of ARDS (defined as a LIPS ≥ 4 points), and patients with ARDS. Also, patients with ARDS will be stratified according to severity of ARDS (mild, moderate and severe).
Study conduct
Local investigators will screen all patients admitted to participating ICUs during a 7-day period. This period of inclusion of patients lasts from Monday at 8:00 AM to the next Monday at 7:59 AM (in time zones of the participating centers), the starting date will be flexible for participating centers and shall be determined at a later stage together with the study coordinator.
Baseline and demographic data on all screened patients, regardless of meeting enrolment criteria are recorded (see below).
Data collection
Baseline and demographic variables are collected on the day of admission, including gender, age, height, weight, ethnicity, smoker (never, former or current), functional status (non-dependent, partially dependent, totally dependent), presence of ARDS according to Berlin definition (Table 2) [11], Lung Injury Prediction Score (LIPS) (Table 3) [12], Acute Physiology And Chronic Health Evaluation (APACHE II) score, Simplified Acute Physiology (SAPS III) score, reason for ICU admission, and reason for intubation and ventilation. In addition, it is determined whether patients have Chronic Obstructive Pulmonary Disease (COPD) with use of inhalation therapy and/or steroids, active cancer, heart failure, according to the New York Heart Association (NYHA), diabetes mellitus, chronic kidney failure with or without hemodialysis, liver cirrhosis, immunosuppression, and arterial hypertension. On the day of start of invasive ventilation the reason for mechanical ventilation is collected, as well as whether the patient received non-invasive ventilation before intubation.
| Time | Within one week of a known clinical insult, or new/worsening respiratory symptoms | ||
| Chest imaging* | Bilateral opacities not fully explained by effusions, lobar/lung collapse or nodules | ||
| Origin of edema | Respiratory failure not fully explained by cardiac failure or fluid overload; need objective assessment to exclude hydrostatic edema if no risk factor present (e.g., echocardiography) | ||
| Oxygenation** | Mild 200 < PaO2 / FiO2 < 300 PEEP or CPAP ≥ 5 cm H2O*** |
Moderate 100 < PaO2 / FiO2 < 200 PEEP ≥ 5 cm H2O |
Severe PaO2 / FiO2 ≤ 100 PEEP ≥ 5 cm H2O |
Table 2: The Berlin definition of ARDS [12].
| LIPS points | LIPS points | ||
|---|---|---|---|
| Predisposing Conditions Shock Aspiration Sepsis Pneumonia High-risk surgery* Orthopedic spine Acute abdomen Cardiac Aortic vascular High-risk trauma Traumatic brain injury Smoke inhalation Near drowning Lung contusion Multiple fractures |
2 2 1 1.5 1 2 2.5 3.5 2 2 2 1.5 1.5 |
Risk Modifiers Alcohol abuse Obesity (BMI > 30 kg/m2) Hypoalbuminemia Chemotherapy FiO2 > 0.35 (> 4 l/min) Tachypnea (RR > 30 bpm) SpO2 < 95% Acidosis (pH < 7.35) Diabetes mellitus** |
1 1 1 1 2 1.5 1 1.5 -1 |
Table 3: Lung Injury Prediction Score (LIPS) calculation worksheet [13].
Every day, until ICU discharge, death or day 7 (whichever comes first), patients are evaluated according to ventilation status (extubation or not), continuation of ventilation by non-invasive ventilation, tracheostomy, and mortality. Ventilation parameters (ventilation mode, tidal volume size, respiratory rate, peak and plateau [with volume-controlled modes] or maximum airway pressure [with pressure-controlled modes], Positive End-Expiratory Pressure (PEEP), inspired oxygen fraction, inspiration to expiration ratio, minute volume), oxygenation parameters (PaO2, PaCO2, arterial bicarbonate, arterial pH, arterial base excess, end-tidal fraction of CO2), vital signs (heart rate, cardiac rhythm, blood pressure, central venous pressure), transfusion requirements (red blood cell, fresh frozen plasma and platelets), daily fluid balance, sedation scores (RASS, SAS or Ramsay), and Sequential Organ Failure Assessment (SOFA) subgroups (cardiac, hepatic, respiratory, coagulation, kidney and neurologic) are recorded every day close to 08:00 AM until ICU discharge, death or day 7 (whichever comes first).
Pulmonary complications (new requirement of invasive ventilation, pulmonary infection, atelectasis, barotrauma, pleural effusion, new pulmonary infiltrates, and development or worsening of ARDS), and extrapulmonary complications (sepsis, extra-pulmonary infection, acute kidney injury and renal replacement therapy) are recorded daily until ICU discharge, death or day 7 (whichever comes first) and on ICU and hospital discharge.
On day 90, hospital-free days, ICU-free days, ventilation-free days, need of tracheostomy and mortality are recorded; if the patient is still admitted to the hospital on day 90, this day will be recorded as last day of follow-up.
Study endpoints
The primary endpoint is the variability of size of tidal volumes used amongst diverse ICU patient categories. Secondary clinical endpoints include: 1) other ventilation parameters (including plateau pressure levels, PEEP levels, and driving pressure levels); 2) development of ARDS in patients without ARDS at the onset of mechanical ventilation; 3) worsening of ARDS in patients with ARDS at the onset of mechanical ventilation; 4) pulmonary infection; 5) other pulmonary complications (barotrauma, pleural effusion and atelectasis); 5) need for tracheostomy; 6) extra-pulmonary complications (acute kidney injury, renal replacement therapy, sepsis, extra-pulmonary infection); 7) number of ventilator-free days at day 28 and 90; 8) length of stay in ICU and in hospital at day 90; 9) all-cause ICU and hospital-mortality; 10) all-cause mortality at day 90.
All-cause mortality is defined as any death during follow-up and length of stay as the time between admission and discharge or death. Days of ventilation is defined as time between orotracheal intubation and successful extubation (in case of intermittent mechanical ventilation via a tracheostomy, every day a patient needs ventilation counts as one extra day of ventilation, irrespective of duration of ventilation that specific day) In case of non-invasive ventilation, the duration will be assessed separated from the assessment of invasive mechanical ventilation.
Pulmonary infection is defined as need of new antibiotics in the presence of new or changed lung opacities on chest X-ray and/or new or changed sputum plus at least one of the following criteria: 1) temperature >38.3ºC; or 2) WBC count >12,000. Atelectasis is suggested by lung opacification with shift of the mediastinum, hilum, or hemidiaphragm towards the affected area, and compensatory overinflation in the adjacent nonatelectatic lung, while pleural effusion is suggest by lung opacification with shift of the mediastinum, hilum, or hemidiaphragm towards the non-affected area. Barotrauma is defined as the air in mediastinum or in the pleural space with no vascular bed surrounding the visceral pleura. ARDS is defined according to the Berlin definition and worsening of ARDS is defined as any change in the prior classification (i.e., mild to moderate or severe, or moderate to severe). Systemic Inflammatory Response Syndrome (SIRS), sepsis, severe sepsis, and septic shock is defined according to consensus criteria [13], and acute kidney injury according to the RIFLE classification system [14].
Sample size calculation
The sample size is calculated for the largest and most relevant subgroup of the primary endpoint, the tidal volume size amongst patients without ARDS and also, expresses the number of patients needed to ensure that the margin of error is small enough to remain relevant for our objective. Experience a mean ± standard deviation tidal volume in patients without ARDS of 10 ± 2 ml/kg PBW, considering the incidence of 30% of ARDS in the population of interest [15], with 95% confidence interval and a margin of error of 0.16, and corrected for 10% of drop-out, the net total sample size needed is 952 patients. To correct for drop-outs (incomplete follow–up, etc), we will include at least 1,000 patients.
Analysis
Normally distributed variables will be expressed by their mean and standard deviation; not normally distributed variables will be expressed by their medians and interquartile ranges; categorical variables will be expressed as n (%). In test groups of continuous normally distributed variables, Student’s t-test will be used. Likewise if continuous data are not normally distributed the Mann-Whitney U test will be used. Categorical variables will be compared with the Chi-square test or Fisher’s exact tests or when appropriate as relative risks. Statistical uncertainty will be expressed by 95% confidence levels.
Primary outcome is the tidal volume size in each group within mechanical ventilation, presented as milliliters per kilogram of predicted body weight (ml/kg PBW). The ml/kg PBW will be analyzed as continuous variables. If the data is normally distributed, one-way Analysis Of Variance (ANOVA) or two-way ANOVA assessing the time-interaction between groups and days of observation will be used. When not normally distributed the Kruskal-Wallis test or Friedman test assessing the time-interaction between groups and days of observation will be used.
Propensity score is calculated by a multivariate logistic regression model with outcome as the dependent variable, while all other covariates related to mortality is included as independent variable. Tidal volume size related to outcomes is investigated using conditional logistic regression. Also, a Cox proportional hazards model with outcomes as dependent variables and tidal volume and propensity score as covariates is used. Time-course variables (e.g., repeated measures of ventilatory parameters, vital signs, oxygenation parameters and others) are also analyzed by a linear mixed model. The linear mixed models procedure expands the Generalized Linear Model (GLM) so that the data are permitted to exhibit correlated and non-constant variability. The model includes two factors: 1) study group (fixed factor), each level of the study group factor can have a different linear effect on the value of the dependent variable; 2) time as covariate, time is considered to be a random sample from a larger population of values, the effect is not limited to the chosen times. Pre-specified subgroup analyses will be performed in the following subgroups: 1) ARDS vs. Non-ARDS; 2) severity of ARDS; 3) reason for ICU admission; 4) reason for intubation and mechanical ventilation; and 5) at risk or not for ARDS (according to LIPS).
Statistical significance is considered to be at a p-value of <0.05. Statistical analyses are conducted using SPSS version 20.0 (SPSS, Inc., Chicago, IL).
The study coordinator, the principal investigator and two additional investigators of PROVENet (http://www.provenet.eu/) form the Core Steering Committee. The Steering Committee is composed of these investigators plus the investigators involved in the design of the study and writing of the study protocol. National Coordinators are responsible for administrative management and communication with local Coordinators (in participating hospitals) and provide assistance to the participating clinical sites in study management, record keeping and data management. National Coordinators and local Coordinators are expected to guarantee the quality and security of the data collected.
PRoVENT is an international multi-center prospective observational study that aims to determine ventilation practice and outcomes of consecutive intubated and ventilated ICU patients in a 7-day period in ICUs in Europe, Australia and the Americas. PRoVENT will help to understand current mechanical ventilation practice, in particular variability in tidal volume size, amongst patients without, at risk for or with ARDS. Results of this study can and should be used to plan future studies of mechanical ventilation in ICU patients. The sample size of PRoVENT will have power to determine the current practice of ventilation and the tidal volume size in several subgroups of mechanically ventilated patients, like those without ARDS, those at risk for ARDS and those in each severity group of ARDS.
Several observational studies in ICU patients under mechanical ventilation have been published in recent years (Table 4) [1,4,15-23]. Differences in reported tidal volume sizes between studies are large, but there is a suggestion that lower tidal volumes are increasingly used over the last years. Previous studies lack important information, first, patient populations studied are heterogeneous, and most of the published analyses do not allow conclusions regarding ventilation practices in specific patient groups (i.e. patients without ARDS, patients at risk for ARDS, and patients with mild, moderate or severe ARDS). Furthermore, common to all previous studies, the publications do not report analyses of effects of tidal volume size on important clinical outcome measures. This information is crucial for future trials of mechanical ventilation in ICU patients. Indeed, we need to know which patients other than those with ARDS would benefit from the use of lower tidal volumes. Second, for power calculations information is needed with regard to the primary endpoint (e.g., incidence of development of ARDS, duration of mechanical ventilation, or death) of patient groups of interest in planning any trial. Third, we need to know what tidal volumes are used in groups of interest, to choose the appropriate tidal volume size in the control groups of future trials. PRoVENT is the first observational study that can provide this information.
| First Author | Year of Publication | Study Location | Patient Selection | Tidal Volume, ml/kg PBW |
|---|---|---|---|---|
| Luhr et al. [16] | 1999 | 132 ICUs in Scandinavia n = 1231 |
MV > 24 hours | 8.1 (all patients) 8.3 (patients with mild ARDS)* 8.3 (patients with M/S ARDS) |
| Valta et al. [17] | 1999 | 1 ICU in Finland n = 59 |
ARDS | 8.1 (all patients) |
| Esteban et al. [18] | 2002 | 361 ICUs in 20 countries worldwide n = 5183 |
MV > 12 hours | 8.4 (patients with COPD) 8.6 (patients with ARDS) |
| Bersten et al. [19] | 2002 | 21 ICUs in Australia n = 168 |
ARDS | 9.7 (patients with ARDS) |
| Brun-Buisson et al. [20] | 2004 | 78 ICUs in Europe n = 463 |
ARDS | 9.5 (patients with ARDS) |
| Tomicic et al. [21] | 2008 | 349 ICUs in 23 countries worldwide n =4968 |
MV > 12 hours | 9.3 (all patients) |
| Linko et al. [22] | 2008 | 19 ICUs in Chile n = 156 |
MV > 12 hours | 9.6 (all patients) 9.4 (patients with ARF) 10.2 (patients without ARDS) |
| Villar et al. [23] | 2009 | 25 ICUs in Finland n = 958 |
MV > 6 hours | 8.7 (all patients) |
| Esteban et al. [4] | 2011 | 17 ICUs in Spain n = 255 |
ARDS | 7.2 (all patients) |
| Azevedo et al. [15] | 2013 | 45 ICUs in Brazil n = 622 |
MV > 24 hours | 7.3 (patients without ARDS) 8.1 (patients with mild ARDS) 7.6 (patients with M/S ARDS) |
| Esteban et al. [1] | 2013 | 927 ICUs in 40 countries worldwide n = 8151 |
MV > 12 hours | 8.2 (all patients) |
Table 4: Systematic review of literature on studies about mechanical practice ventilation and tidal volume size in critically ill patients.
It can be difficult and sometimes even impossible to distinguish patients without ARDS from those with mild ARDS, since previously used criteria (i.e., the American-European Consensus Criteria [24]) and present definition (i.e., the Berlin definition [11]) lack sufficient power to discriminate between patients at risk for ARDS or with mild ARDS, and between patients with mild ARDS and patients with moderate or severe ARDS [12,25]. Notably, none of the published studies so far used the new definition for ARDS [11]. Since ventilation with lower tidal volumes is well established in patients with the syndrome, failure to identify patients with mild ARDS can lead to the use of higher tidal volumes in this group of patients, potentially worsening their outcomes. The use of lower tidal volumes for all patients can potentially avoid this situation. Also, recent studies show that median tidal volume size in all subgroup of patients (without and with ARDS) was well above 6 ml/kg PBW. The reasons for lack of adherence to a lower tidal volume strategy may include concerns about adverse effects of low tidal volumes, such as hypercapnia and increased need for sedatives, insufficient knowledge of the lung protective ventilation protocols and under recognition of ARDS [15,26].
Despite the benefits associated with use of lower tidal volumes, there are some possible side effects. Use of lower tidal volumes may increases the need for sedation and even neuromuscular blockade, increasing the risk of delirium and the rate of ICU-acquired paresis [10]. Also, the use of lower levels of assistance could exhaust the respiratory muscles, leading to increased duration of mechanical ventilation [10]. Previous studies did not confirm these effects, since the use of lower tidal volume did not increase the need of sedation [27] and could be associated with a shorter hospital length of stay [9]. Well-powered, probably large, studies are needed to definitively answer these questions.
Recently, much attention has been drawn to the role of driving pressure (plateau pressure or maximal airway pressure minus PEEP) in development of ventilator-associated lung injury. Some reports suggest that higher driving pressure levels are associated with worse outcome of patients with ARDS [28-30]. With data of PRoVENT, by building a predictive model, and with the use of multivariate analyses, it could be possible to discriminate the effects of tidal volume size versus driving pressure on patient’s outcomes.
In conclusion, PRoVENT is an international multicenter observational study powered to investigate the tidal volume size actually used and the outcomes of ICU-patients intubated and under mechanical ventilation without ARDS, without ARDS but at risk for, and with mild, moderate or severe ARDS.