Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2014) Volume 4, Issue 6
Study background: Cellulitis and erysipelas are common skin and soft tissue infections. Antibiotics are the mainstay of therapy, but to date there is no consensus on whether intravenous or oral therapy are optimal choices, and the suggested duration of therapy.
Methods: In a randomized non-inferiority, parallel trial, consecutive eligible adult patients will be randomized by random block allocation to the intervention arm of 24 hours IV therapy versus ≥ 72 hours IV therapy (both followed by oral therapy to total duration of 10 days). Antibiotics used are anti-staphylococcal penicillins and first generation cephalosporins.
Resolution of cellulitis is defined by; resolution of fever, lack of progression of the involved area at 48-72 hours, and lack of requirement for antibiotics beyond the study period of 10 days.
Secondary outcome measures include; pain in the affected limb, return to normal mobility, blinded photographic assessment, adverse events, and recurrence of infection within 30 days. A cost effectiveness analysis will also be undertaken.
Results: Over a 12-month period from November 2012, 243 patients were screened for participation in the SWITCH pilot trial. Forty patients were recruited (16%) and 203 patients (84%) fulfilled one or more exclusion criteria. Patients were excluded based on having received ≥48 hours IV antibiotics prior to presentation, an alternative diagnosis and an unwillingness to participate.
20 patients were randomized to ≥72 hours IV therapy; 19 successfully responded to therapy and 1 case withdrew prematurely. 20 cases were randomized to 24 hours IV therapy; 17 responded successfully and 3 withdrew prematurely.
Conclusions: This pilot randomized trial of short course therapy for cellulitis has determined that such a trial is safe and feasible. Recruitment may be affected by many conditions that are mislabeled as cellulitis or represent non-acute pre-treated cellulitis. This non-inferiority trial will now expand to multiple sites in 2014.
Keywords: Cellulitis, Erysipelas, Skin infections, Antibiotics, Randomized controlled trial
IV: Intravenous; HITH: Hospital in the Home; ICU: Intensive Care Unit; ED: Emergency Department; SSTIs: Skin and Soft Tissue Infections
Cellulitis and erysipelas are common skin and soft tissue infections seen in both primary care and acute hospital settings locally and internationally with an estimated incidence of 16.4-24.6/1000 personyears [1,2]. Cellulitis is generally considered synonymous with the term ‘erysipelas’, although they can be differentiated according to the tissues affected. While erysipelas affects the upper dermis, including the superficial lymphatics, cellulitis involves the deeper dermis, and subcutaneous fat [3]. The most common causative organism is Streptococcus sp., and the leg is the most commonly affected site [2,4,5]. The infections that result are considered paucibacillary, and carry an excellent prognosis [6]. However, despite a very low mortality, these skin and soft tissue infections are painful and disabling during the acute phase, can be associated with significant systemic symptoms and necessitate time away from usual daily activities.
The local clinical features of both erysipelas and cellulitis are rapidly spreading areas of edema, redness, and heat, sometimes with lymphangitis and lymphadenopathy. The diagnosis of erysipelas and cellulitis is almost always clinical, with blood cultures being positive in only 5% of cases, [7] and needle aspiration and other cultures of the affected area being of low diagnostic yield [7-9]. The lack of a gold standard diagnostic test results in the diagnosis sometimes being complex as there are many conditions which may be confused with cellulitis, such as; dermatitis, acute gout, venous eczema, and acute lipodermatosclerosis [10].
Despite the frequency with which clinician’s treats cellulitis and erysipelas, there is no consensus on whether intravenous (IV) or oral therapy is the optimal choice, nor the most appropriate duration of therapy. Furthermore, there are no validated objective measures of severity or improvement in the case of cellulitis that can assist clinicians in making the decision to switch from IV to oral therapy [11]. The Infectious Diseases Society of America recommends that while many patients with cellulitis or erysipelas may be treated orally from the start; patients who are systemically unwell should be treated with intravenous antibiotics and then transitioned to oral therapy once they are able to tolerate oral medication [6]. One non-randomized study showed no benefit to intravenous over oral therapy even in patients who were febrile on enrolment [12]. It has however been shown that in practice the duration of IV therapy varies widely. Previous research on cellulitis has demonstrated a mean duration of IV treatment of 6 days, mean hospital stays of approximately 5 days, and therapy duration of 10 days or more in 10-42% of cases, with no significant difference in outcome [12-16]. Such management regimens are inherently inefficient and result in possible unnecessarily long hospital stays [11].
Geelong Hospital is a 450 bed tertiary teaching hospital in Geelong, Victoria servicing a large catchment area of Southwestern Victoria, Australia. Cases of lower limb cellulitis requiring parenteral antibiotics at our hospital are managed either via inpatient admission or home administration of IV antibiotics via the Hospital in the Home (HITH) service. In order to determine the safety and efficacy of short-course IV therapy, we designed a prospective, randomizedcontrolled, non-inferiority trial comparing a control arm of 72 hours or more intravenous antibiotics to the intervention arm of 24 hours of intravenous antibiotics, both followed by oral antibiotics for total treatment duration of 7-10 days. We present here both our trial protocol and the results of the pilot trial.
Primary objective
To determine the safety and efficacy of 24 hours of IV therapy followed by oral therapy compared to 72 hours or more of IV therapy followed by oral therapy to a total of 7-10 days antibiotic treatment duration.
Study design
The SWITCH trial is an investigator-initiated, prospective, randomized open label, non-inferiority multicenter trial comparing 24 hours of IV therapy with 72 hours or more of IV therapy followed by oral therapy to 7-10 days duration. All treatments used in this study are current approved and recommended therapies for the treatment of cellulitis [17]. IV antibiotics used are anti-staphylococcal penicillins, and first generation cephalosporins. Oral antibiotics include; di/ flucloxacillin, cephalexin, and clindamycin.
The 24 hour IV trial arm was chosen as from our experience it is common for patients presenting with cellulitis to have associated nausea and vomiting and to be unable to tolerate oral therapy initially. Trial antibiotics were chosen to cover the usual streptococcal and staphylococcal pathogens in the Geelong area. Geelong has a rate of community-acquired Methicillin resistant Staphylococcus aureus (MRSA) of approximately 5%.
Inclusion criteria
Participants are eligible for inclusion in the trial if they meet all of the following criteria:
1. Acute cellulitis or erysipelas of lower limb with consistent clinical features, including erythema, pain, swelling of lower extremity of acute onset with presence of or recent history of fevers and/or chills, rigors, and nausea.
2. Age > 18 years.
3. Patient is planned for IV therapy for cellulitis/erysipelas of the lower limb as inpatient or via HITH.
Exclusion criteria
Potential participants are excluded from the study if they meet any of the following criteria:
1. Age <18 years
2. Pregnancy
3. Immunosuppression including any one of: active chemotherapy in the last 6 weeks, receipt of prednisolone >20 mg/ day, neutropenia with neutrophil count <0.5 × 109/L, or alternative conditions significantly affecting the immune system.
4. Alternative diagnosis, including but not limited to: venous eczema, diabetic foot infection, surgical site (wound) infection or other open wound.
5. Penetrating injury or bite.
6. Suspected complication such as an abscess or necrotizing infection.
7. Septic shock or other reasons for intensive care unit (ICU) admission.
8. *Antibiotics effective against cellulitis for >24 hours IV (including receipt of di/flucloxacillin, cephalexin, cephazolin, clindamycin and vancomycin).
9. Patients unwilling to participate or who in the opinion of investigators would not be able to comply with the requirements of the study.
*Exclusion criteria 8 for the pilot trial also included the receipt of >24 hours oral antibiotics, which was altered 5 months after recruitment commenced to >48 hours oral antibiotics.
Patient identification
Consecutive patients presenting with acute cellulitis or erysipelas are reviewed for participation in the SWITCH trial. These patients are identified either after referral to the HITH team or via a real-time electronic search for patients with a diagnosis of lower limb cellulitis in our Emergency Department. Participants are enrolled either from the Emergency department, the inpatient wards, or the HITH service. Following informed consent, patients are randomized to standard or short course IV therapy.
Randomization
Randomization for the trial is performed via random block allocation. Allocation of participants to either the short-course or longer-course treatment arms occurs in ascending numeric order and is completed on enrolment into the study. Participant allocation is via sealed opaque envelopes, prepared by a research assistant with no involvement in patient recruitment.
Study visits
Patients are reviewed on recruitment (visit 1), after 48-72 hours (visit 2), and after 7-10 days (visit 3). Researchers make a follow-up telephone call 30 days after recruitment to determine whether the patient has recovered or whether the patient has developed a recurrence of infection (Figure 1).
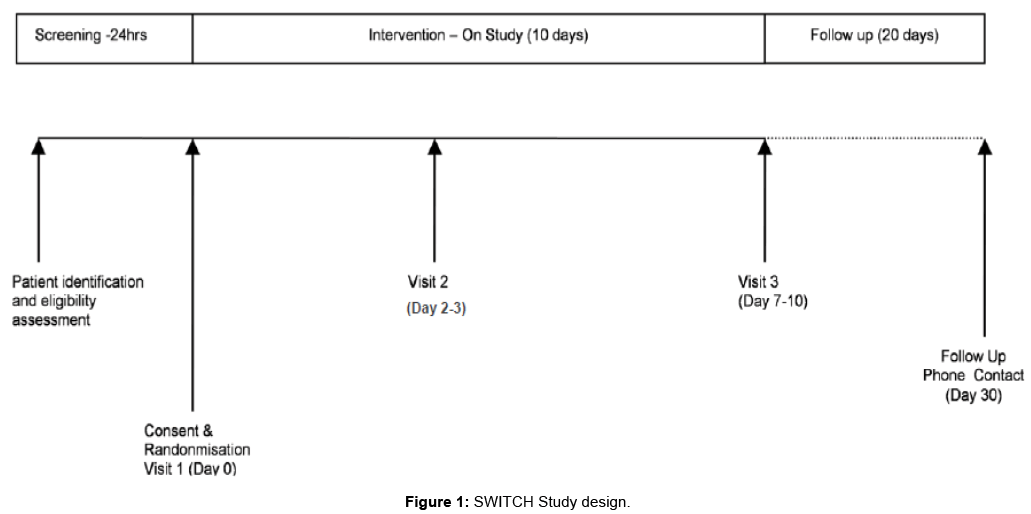
Figure 1: SWITCH Study design.
Primary outcome measures
Resolution of cellulitis, defined by all of the following 3 criteria:
1. Resolution of fever at visit 2.
2. Absence of progression of skin and subcutaneous abnormalities at visit 2.
3. Absence of ongoing requirement for antibiotic therapy beyond the study period of 10 days.
Secondary outcome measures
1. Self-reported pain using the Wong-Baker face scale [18]
2. Return to normal mobility
3. Blinded photographic assessment of the affected lower limb
4. Adverse events
5. Disease recurrence within 30 days
The above information is collected from study participants via a study diary (Figure 2), in-person visits and 30-day telephone follow-up.
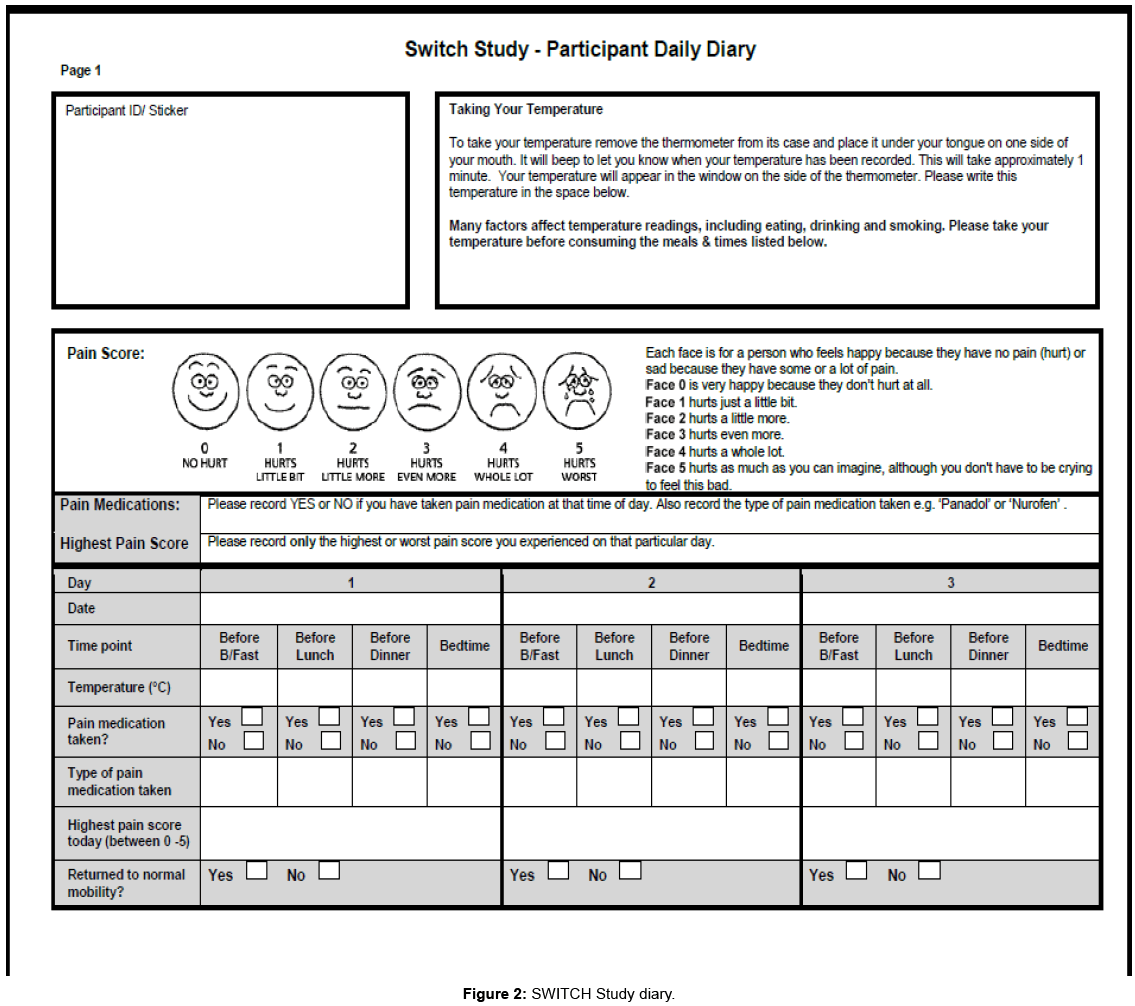
Figure 2: SWITCH Study diary.
Retrospective review
Five months after the pilot trial commenced, in the setting of slow prospective recruitment, a retrospective review of patients at our institution coded as having cellulitis in the 1 year prior (November 2011- November 2012) was undertaken to inform likely future recruitment patterns. Cases were analyzed against the inclusion and exclusion criteria for the SWITCH trial.
Statistical analysis
Demographic tables will be reported by treatment arm. Analysis will be based on the intention-to-treat sample, with the difference in the proportion of patients with resolution of cellulitis (as defined above) being presented. 95% confidence intervals for the difference in proportions will be calculated by inverting the score test. Secondary outcomes will be summarised by treatment arm, with medians (IQRs) and proportions where appropriate. Confidence intervals for medians will be calculated by bootstrapping. Further risk factors will be explored by regression models. All analyses will be performed using the open source statistical software R (http://www.r-project.org/ ).
This trial has been registered with the Australia Clinical Trials Registry (ACTRN12613001366741) and approved by the Barwon Health Human Research and Ethics Committee.
The SWITCH pilot trial commenced enrolling patients in November 2012. Patients were screened according to the inclusion and exclusion criteria described above.
Over a 12-month period from November 2012, 243 patients were screened for possible participation in the SWITCH trial. Of these 243 patients, 40 (16%) were recruited to the SWITCH pilot trial and 203 patients (84%) fulfilled one or more exclusion criteria. The majority of patients (37%) were excluded based on having received oral antibiotics for ≥48 hours or due to an alternative diagnosis (26%). Other reasons for exclusion included; unwillingness to participate or considered unable to comply with the study (15%), planned for oral antibiotics only (6%), penetrating injury or bite (5%), immunosuppression (4%), suspected abscess or necrotizing infection (3%).
Twenty patients were randomized to ≥ 72 hours IV therapy; 19 successfully responded to therapy and 1 case withdrew prematurely.
Twenty patients were randomized to 24 hours IV therapy; 17 responded successfully to therapy, 2 patients withdrew prematurely after providing informed consent, and 1 patient was withdrawn by investigators because of ICU admission for hypotension after recruitment.
Participants who withdrew themselves from the trial did so before Visit 2, without any evidence of treatment failure. One patient developed self-limiting, non Clostridium difficile diarrhea after visit 3. There were no other adverse events.
Patients in the intervention arm of the pilot SWITCH trial had an average length of stay of 1.3 days, in comparison with patients in the conventional therapy duration arm, where the average inpatient length of stay was 3.7 days.
A 12-month retrospective review of cases coded as cellulitis of the lower limb revealed 265 cases. These cases of cellulitis were analyzed against the inclusion and exclusion criteria for the SWITCH trial. 59 cases (22%) would have met criteria for inclusion in the SWITCH trial, and 206 cases (78%) met one or more criteria for exclusion. The major reasons for exclusion in this retrospective review were; oral antibiotic therapy >48 hours (108,52%), alternative diagnosis (75,36%), suspected necrotising fasciitis or abscess (23,11%), and penetrating injury or bite (16,8%).
Cellulitis and erysipelas are seen in both primary-care settings and in hospital EDs. In ambulatory care, uncomplicated skin and soft tissue infections are among the most frequent indications for outpatient antibiotics, and in EDs patients with cellulitis comprise 1-14% of visits [19,20]. In the USA hospital visits for abscesses and cellulitis increased from 17.3 to 32.5 per 1000 person-years from 1997 to 2010, and in 2010 there were 600,000 hospital admissions for these conditions [21]. Research in the United Kingdom found that skin and soft tissue infections (SSTIs) accounted for 10% of hospitalizations, with mean stays of approximately 5 days, and were the second most common reason for hospital-based IV antibiotic therapy lasting more than 48 hours [14].
In 2011 and 2012 there were 265 and 243 cases respectively of Skin and Soft Tissue Infection (SSTI) presenting to Geelong hospital, respectively. Our institution cares for the Greater Geelong population estimated at 22,515 persons [22]. Extrapolating this to the current estimated Australian adult population of 23,355,000, suggests that country-wide there will be 26,779 cases of skin and soft tissue infection per year requiring treatment.
The optimal duration of intravenous antibiotics for cellulitis is not known. The duration of IV therapy has been shown previously to vary widely, with no outcome benefits and long hospital stays [11-16]. Furthermore, a recent cohort study of patients with uncomplicated skin infections revealed that 42% of patients received antibiotics for 10 or more days resulting in considerable unnecessary expense [16]. In our pilot trial participants in the intervention arm of 24 hours IV therapy had a length of stay reduced by two-thirds compared to the conventional therapy arm, with equivalent outcomes and no increased adverse events. Shortening the duration of intravenous antibiotics is likely to result in substantial cost savings and reduce the risk of treatment complications.
Managing patients with this type of infection with 24 hours of intravenous therapy and then a course of oral antibiotics would mark a dramatic change in practice for many hospitals, preventing longer hospital stays, or longer courses of IV antibiotics at home and would save on direct healthcare related costs for the inpatient length of stay, hospital in the home program costs, intravenous equipment/ consumables, and nurses visits to patients at home. A British study estimated that if the hospital stay of patients with SSTIs was reduced by only 1 day, savings would amount to £0.5-1 million per year [14].
Administration of unnecessary antibiotics should be avoided to prevent side effects and to reduce overall antibiotic exposure. It has been demonstrated that avoidable antibiotic exposure occurs in nearly half of patient with skin infections [16]. Antibiotics given via the IV route carry a small but not insubstantial risk of phlebitis and IV cannula infection, the risk of which is related to the duration of cannulation [23,24]. Furthermore, a reduced length of stay in hospital can also benefit the patient in terms of spending less time out of their home environment and in reducing the possibility of contracting nosocomial infections during their admission [25].
The Australasian College for Emergency Medicine reported that if a hospital with 20,000 admissions each year saved half a bed day per patient by improving discharges, about 2000 extra patients a year could be admitted [20]. Data from this pilot study reveals that combined length of stay in the acute hospital and hospital-in-the home is reduced among patients in the intervention arm. A formal health economic evaluation in a larger trial is required to confirm the cost savings of reduced IV therapy duration for cellulitis and erysipelas.
Strict inclusion and exclusion criteria have undoubtedly influenced the speed of patient recruitment in this pilot randomized controlled trial, with less than one in five patients identified as suffering from lower limb cellulitis being recruited. This is partly due to the fact that many skin and soft tissue conditions such as venous eczema, abscess or penetrating injury are loosely referred to as cellulitis. In addition, in our institution it is very common for patients to present or be referred to hospital for treatment of presumed cellulitis or erysipelas after having received 48 hours or more of oral antibiotics. More than 48 hours of oral antibiotics was initially an exclusion criteria when the pilot trial commenced. This cut-off for pretreatment was indeed arbitrary, and another recent trial protocol used more than 4 days of therapy as a cut-off point [26]. Although it is unclear whether IV therapy is beneficial in systemically well patients with non-acute cellulitis of the lower limb the SWITCH protocol has been refined to include patients who have received 48 hours or more of oral antibiotic therapy with an intention to compare this sub-group with non-pre-treated patients in an exploratory data analysis phase.
Studying a condition, which has predominantly a clinical diagnosis, and relies on visual assessments of improvement, involves some methodological challenges. In order to attempt to standardize assessments and rely on objective measures of improvement, our participant trial diary focuses on the presence of fever and pain, the use of analgesia and the time to return to usual mobility. In addition, digital photographs taken on 3 occasions during the trial will be assessed by a blinded investigator in order to both objectively assess skin changes and to corroborate the primary investigator’s assessment of cellulitis resolution. Other trials of cellulitis are also employing photography as a measure of cellulitis severity [26].
Among the recruited trial patients to date, efficacy in both groups has been in keeping with expectations with regard to the non-inferiority design. Our pilot trial has demonstrated that while this trial is both feasible and safe to undertake, it will be unrealistic to complete this trial in a timely fashion in a single centre. This trial is now expanding to a multicentre trial in Australia and New Zealand.
This trial of short duration IV therapy for a common skin and soft tissue infection is an example of simple clinical research. Investment in such a simple clinical trial may lead to longer durations of therapy being made redundant with the development of protocols for shorter treatments that improve the treatment experience for patients, improve efficiency, and save on costs for healthcare providers.