Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2015) Volume 5, Issue 4
Objective: To demonstrate the efficacy of a 12-week, professionally-facilitated, Internet-based support group for women who are sexually distressed due to gynaecologic cancer and its treatment.
Methods: The participants are women who received treatment for gynaecologic cancer, were diagnosed within the previous five years and who currently have no evidence of disease. They must meet a minimum cut-off score on the Revised Female Sexual Distress Scale (FSDS-R). Enrolled participants are randomized to the immediate treatment condition or to the waitlist control condition. The intervention is delivered in an asynchronous format (i.e., bulletin board), and also includes two scheduled synchronous (i.e., live chat) sessions. Each week, a new topic relating to sexuality and gynaecologic cancer is introduced, and group members are given access to psych educational materials on that topic. Assessments are completed at baseline, month 5, and month 9. The primary outcome is sexual distress, and the secondary outcomes include sexual function, body image, depression and anxiety, relationship satisfaction, and perceived social support.
Results: To date, 234 of the planned 520 participants have been enrolled and 7 groups (4 immediate treatments and 3 waitlist) have been conducted.
Conclusion: Women treated for gynaecologic cancer often experience psychosexual distress. Demonstrating the efficacy of an online intervention that targets those concerns is an important step towards meeting the needs of survivors of gynaecologic cancer.
Keywords: Gynaecologic cancer; Sexual distress; Randomized controlled trial; Online support group
Gynaecologic cancer is associated with a wide variety of psychosexual problems [1-11], with approximately half of all diagnosed women being sexually distressed [7,12]. Sexual difficulties following treatment are the biggest source of distress and the most common sources of sexual distress due to cancer-related treatment are reduced frequency of orgasm and pain [13]. Sexual distress is frequently associated with depression [14-18] as well as problems with body image [19]. These difficulties can disrupt sexual intimacy at a time when the buffering effects of intimate relationships are most needed [19,20]. A decreased sense of intimacy and closeness can also have adverse consequences for a relationship, and for an individual’s self-esteem [21,22].
A need for greater social support and supportive services has been documented among gynecologic cancer survivors [23]. Along with the need for support, there is evidence that a larger social support system is associated with less depression among cancer survivors [24,25] and higher quality of life in gynecologic cancer survivors [26].
It appears that many survivors who are faced with these challenges turn to the Internet for support and information. Distressed cancer survivors may be more likely to participate in Internet support groups than in face-to-face groups [27], possibly due to the convenience of being able to access them at any time, and their anonymity, which may make it easier to discuss highly personal issues. While online groups for cancer survivors are widely available and commonly used, there are few groups that focus specifically on gynecologic cancer or on concerns pertaining to sexuality [28].
Empirical evaluations of Internet cancer support groups have emerged [29,30], including a randomized controlled trial, which found that a professionally-led, online support group reduced distress in breast cancer survivors [30]. Results from our feasibility/pilot study suggest that an online support group may benefit gynecologic cancer survivors who are sexually distressed [31,32]. However, two recent studies of online peer support (i.e., with no professional facilitators) found that cancer survivors receiving online peer (only) support became more psychologically distressed compared to a control condition [33,34]. This research suggests that online support groups should be professionally facilitated in order to be beneficial, and that un-facilitated programs may, in fact, be detrimental.
Overall study design
The primary aim of this mixed methods study is to demonstrate that a professionally facilitated, information-rich, online support group (GyneGals) is beneficial for women who are sexually distressed subsequent to gynecologic cancer and the side effects of treatment. We will also investigate mediators and moderators of treatment outcome (Figure 1).
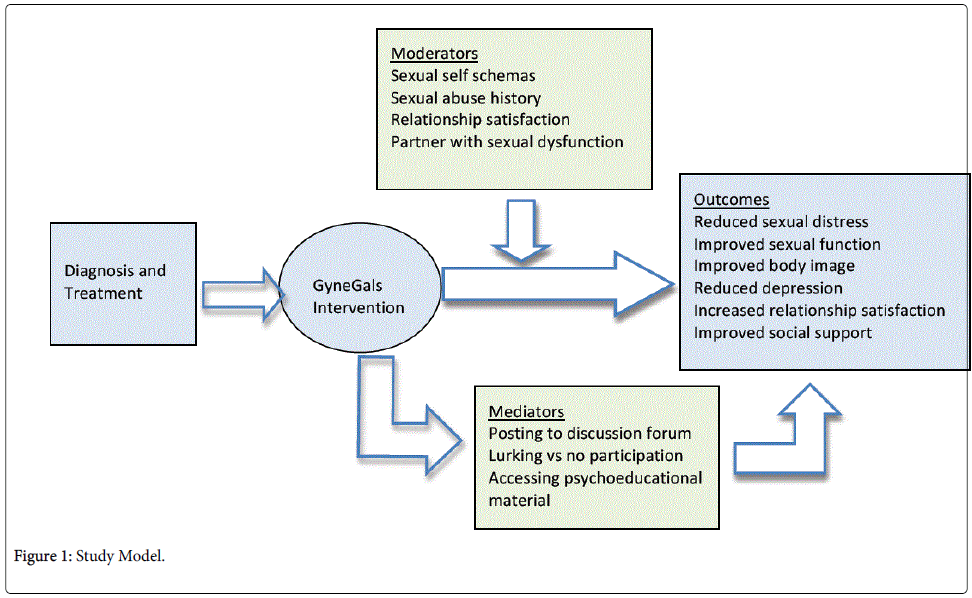
Figure 1: Study Model.
We will recruit 520 participants through oncology centres in the Canadian provinces of Ontario, British Columbia, and Alberta and in the state of New York, USA. Quantitative assessments and the intervention are provided online in secure online environments. All quantitative data are collected using Fluid Surveys. Qualitative data are gathered via telephone interviews (Figure 2).
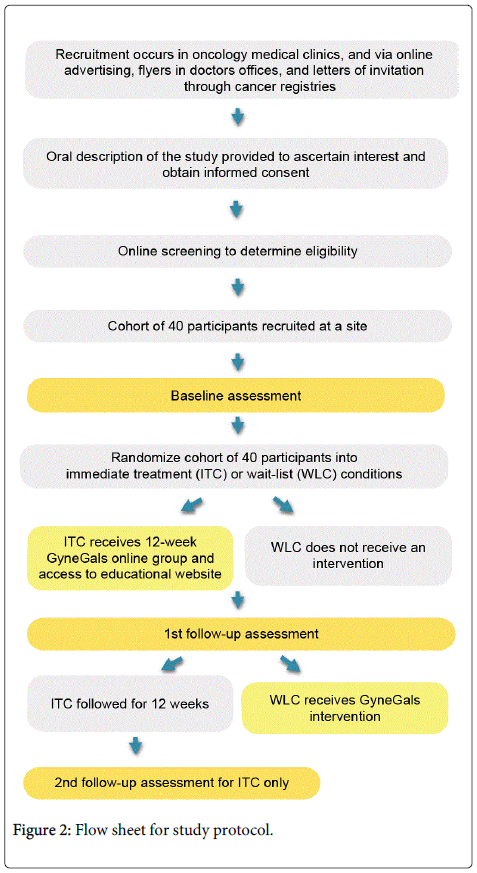
Figure 2: Flow sheet for study protocol.
Inclusion criteria
Participants must be 18 years of age or older and able to speak, read and write in English. Women are considered eligible if they have received surgical, radiation or chemotherapy treatments for any gynecologic cancer, have had no evidence of disease for a minimum of 3 months, are not receiving active treatment and are no more than 5 years post-diagnosis. They must also meet the established cut-off for psychosexual distress, as measured by the Female Sexual Distress Scale-Revised (FSDS-R), and indicate that they are willing to write about their sexual concerns in a private, online discussion forum. Participants must have access to a computer (or tablet) and the Internet.
Exclusion criteria
Individuals experiencing acute suicidality and/or current major psychiatric illness are excluded, as are those who are already receiving another form of treatment or intervention to address their psychosexual concerns at the time of enrolment.
Hypotheses and exploratory questions
We hypothesize that, compared to women assigned to the waitlist control condition, women randomized to the immediate treatment condition will: (1) show a greater reduction in sexual distress (primary outcome); (2) show greater improvement in sexual function, body image, symptoms of depression, relationship satisfaction, and social support (secondary outcomes); and (3) that these benefits will be sustained through to a second follow-up assessment at 4 months post-intervention.
The secondary aim is to examine potential moderators (positive sexual self-schemas, history of sexual abuse, degree of relationship satisfaction, and partner’s sexual difficulties) and mediators (level of active involvement in the support group) of treatment.
Qualitative and exploratory analyses will also be conducted. The qualitative component examines women’s subjective experience of participating in an online support group intervention. Exploratory analyses will address the following questions: a) What characterizes women who join the study but do not log on to the intervention? b) What characterizes women who log on but do not post? c) Is there a benefit to simply observing? d) What baseline variables are potential moderators of treatment outcome? e) Are their other potential mediators of treatment outcome?
Measures
Primary outcome: The Revised Female Sexual Distress Scale (FSDS-R) [35] is a 13-item self-report scale that measures sexually-related distress in women.
Secondary outcomes: The Sexual Function Questionnaire (SFQ) [36] is a 25-item measure developed for cancer patients and can be completed by women regardless of sexual orientation or whether they have a partner. The Sexual Adjustment and Body Image Scale – Gynecologic Cancer (SABIS-G) [37] consists of two independent scales designed to assess changes in sexuality and body image before and after diagnosis. The Hospital Anxiety and Depression Scale (HADS) [38] is a 14-item self-report questionnaire for detecting depression and anxiety in a hospital outpatient setting. The Relationship Assessment Scale (RAS) [39] is a 7-item measure assessing satisfaction with an individual’s romantic relationship. The Medical Outcomes Study (MOS) Social Support Survey [40] consists of 19 items and assesses emotional/informational support, tangible support, affectionate support, and positive social interaction, as well as providing an overall functional support index.
Moderators: Possible moderators of the treatment effect include sexual self-schema, as assessed by the Sexual Self Schema Scale for Women [41], history of prior sexual trauma, as measured by the trauma history screen [42], relationship satisfaction, assessed using the RAS [39], and partner sexual difficulties, measured with a single item adapted from Schover’s sex history form [43].
Mediators: We will examine whether active participation mediates the effects of the intervention. Active participation will be based on 1) the number and regularity of messages that women post, 2) the frequency of lurking on the discussion board (i.e., accessing the discussion forum but not posting), and 3) the number of times women view the educational material (which is separate from the discussion forum).
Qualitative and exploratory: Data from additional measures are collected for descriptive and exploratory analyses.
Randomization
Participants are recruited in cohorts of 40 at each site, and once a full cohort has been enrolled at a given site and participants for that cohort have completed baseline assessments, they are randomly assigned to either the immediate treatment condition (ITC) or the wait-list control condition (WLC).
Immediate treatment and wait-list control conditions
The ITC receives GyneGals, the online intervention, immediately following their cohort’s completion of the baseline assessments. Details of the intervention are provided below. The ITC participants are assessed immediately following completion of the intervention and again 4 months later. The WLC does not receive the online intervention until after completion of the 1st follow-up assessment. Technically, the WLC participants are considered to be out of the study after the follow-up assessment. They are provided the intervention as a courtesy for their participation in the study.
Intervention
The intervention is an asynchronous online group (i.e., bulletin board format) with two scheduled synchronous (i.e. live chat) sessions. The intervention also provides participants with access to psycho-educational material related to sexuality and gynecologic cancer that is housed on a separate website. The advantage of an asynchronous group is that women can participate at any time of the day or night, during the 12 weeks of the intervention. The intervention is informed by the supportive-expressive group therapy model [46], which encourages open and honest expression of thoughts and emotions, receiving and offering support, and learning new ways to cope. The two 90-minute synchronous sessions, offered in weeks 4 and 8, allow participants to “chat” with one another in real time. The first chat session takes place with the two facilitators. The second session involves the two facilitators and two experts in gynecologic cancer-a gynecologic oncology surgeon (SF) and a radiation oncologist (LB).
The intervention is semi-structured and facilitated by two mental health professionals who, between them, have expertise in leading psycho-oncology groups and in issues related to sexuality. A new topic is introduced each week, covering themes adapted from supportive-expressive groups for cancer patients [44] and Schover’s book “Sexuality and Fertility After Cancer” [45]. The material addresses concerns of heterosexual and queer women, as well as partnered and non-partnered women.
Each week, the facilitators post a message on the forum to introduce the theme and to ask questions related to the topic in order to stimulate conversation. A link is also provided to the psycho-educational material covering that week’s topic.
Facilitator training
Training of the facilitators occurred in the first year of this 5-year project. There were three components: 1) observation of an online 12-week GyneGals group; 2) weekly teleconference calls during this 12-week training period to discuss the group; and 3) assigned reading. Two of the investigators (CCC and MLC) co-facilitated the groups for the pilot study and were responsible for training the facilitators for this RCT. Acquisition of skills was assessed by having facilitator trainees compose interventions (i.e., written comments) that they would have made had they been facilitating the group.
Data analysis
The sample size is based on the pilot study’s observed effect size (Cohen’s d) of .3 for decrease in sexual distress, as measured by the FSDS-R [35]. A sample size of 520 gives an 80% chance to detect a .3 standard deviation difference on sexual distress between the immediate treatment (ITC) and wait-list control (WLC) conditions at the .05 significance level (two-tailed). This estimate takes into account 15% loss to follow-up (based on the pilot study) and the effect of clustering, which is due to treatment being delivered in a group format.
The efficacy of the intervention will be assessed using the primary outcome, sexual distress. The difference of the average sexual distress score at the end of month 4 between the treatment and waitlist groups will be calculated and adjusted for the effect of clustering within treatment groups (using a linear mixed effects model). The same analytic strategy will be used to test the effect of the intervention on the secondary outcomes. A Bonferroni correction will be used for testing the secondary hypotheses; the significance level will be set at 0.01 (0.05/5) in order to control for the probability of a Type 1 error.
In order to assess whether the benefits from participating in the intervention are sustained through to the second follow-up assessment, for each of the six outcome measures a difference score will be calculated between the score on the outcome variable at baseline and the score at the second follow-up for the ITC. The hypothesis will be tested by a t-test adjusted for clustering due to women being in the same support group (using a linear mixed effects model), with the null hypothesis being that the difference is zero.
A grounded theory analysis will be used for all qualitative analyses [46]. This involves analyzing as many interviews as necessary to achieve theoretical saturation. The aim of the qualitative analyses is to understand women’s experience of the intervention.
Since November 2012, 234 of the planned 520 participants have been enrolled in the study, and 7 groups (4 ITC and 3 WLC) have been completed. We anticipate that the study will be closed to accrual by August 2016 and that all data will be collected by May 2017.
We hypothesize that the immediate treatment group will show greater improvement in sexual distress, sexual function, body image, depression symptoms, relationship satisfaction, and social support compared to the waitlist control condition. Furthermore, we expect to find that benefits on these outcomes will be maintained four months post-intervention among ITC participants.
Regarding potential moderators of treatment effectiveness, we hypothesize that: a) women with positive sexual self-schemas will show a greater reduction in distress compared to other women; b) a history of sexual abuse will be associated with less benefit from the intervention; and, for partnered women, c) being high in relationship satisfaction, and d) having a partner who does not have sexual difficulties will each be associated with greater benefit.
We expect that active involvement in the support group will mediate treatment effectiveness, such that the more actively involved an individual is, the more benefit she will have.
The qualitative analyses will enable us to understand women’s subjective experience of participating in this intervention and the extent to which they may or may not have found it helpful. The exploratory analyses will examine other potential moderators and mediators and identify factors that may influence participation patterns. These qualitative and exploratory quantitative analyses may inform whether modifications to the intervention are needed in order to maximize participation and benefit.
Women who have been treated for gynecologic cancer experience significant psychosexual distress, which affects their relationships, body image and mental health. As there are limited resources available to address the concerns of gynecologic cancer survivors, demonstrating the efficacy of an online intervention designed for this population will be an important step towards meeting their needs.
This research was funded by the Canadian Institutes of Health Research (grant number MOP-123219) and Ovarian Cancer Canada. The authors would like to acknowledge the contributions of Yvonne Brandelli, Jocelyn Canty, Jessica Kalbfleisch, Adrienne Marsh, Joanne Park, Cara Stabil, Aubrie Vigna, Manon Labrecque, Ericka Wiebe, Yvonne O’Meara, Lisa Roeflsma. Jan Silverman, Lisa Skelding, Yvonne Erskine, Laurie Ching, Andrea Beck, Abby Gunn, and Erin Breckon, as well as the various community organizations and cancer centers involved in promoting the study. We are especially grateful to the women who agreed to participate in this research.