Journal of Defense Management
Open Access
ISSN: 2167-0374
ISSN: 2167-0374
Research Article - (2013) Volume 0, Issue 0
The nasal deformities inherent in the cleft lip are challenging. Controversy exists regarding the best time to attempt surgical correction of this nasal problem. Opinion is now strengthening for the correction of these nasal deformities along with the repair of cleft lip either by a closed technique or by an open or external open tip rhinoplasty technique. Open tip rhinoplasty technique has the added advantage that it allows accurate repositioning and secure stabilization of the key anatomical structures such as the lower alar cartilages under direct vision, and the incisions of this procedure can be carried out through the hidden rim incisions of the nostrils without any residual scars. Following the introduction of open tip rhinoplasty at the time of lip repair in the cleft lip and palate patients by J.A. Trott and N. Mohan, it was decided to try this technique with minor modifications in our cleft lip and cleft palate management at the Department of Plastic & Reconstructive Surgery, Khoula Hospital, Muscat, Sultanate of Oman, since 1994, where over 75 new patients of cleft lip and palate are operated annually. Only unilateral and bilateral complete cleft lip with gross nasal deformities are selected for this study because nasal deformities are minimal in incomplete cleft lip. Conventionally, there is hesitation to do radical nose correction for the cleft lip patients because of the fear of possible growth retardation. The present technique, while it achieves excellent post operative results constantly, does not entail any more trauma to the cartilage complex than any of the conventional closed rhinoplasty techniques. Results obtained by this method appear to be superior to those by closed rhinoplasty techniques and there is no retardation of the nasal growth noticed.
Keywords: Nasal deformities; Rhinoplasty technique; Cleft lip; Cleft palate management
There is significant improvement in the results of cleft lip repair in the present decade. But, nasal deformity is the greatest corrective challenge and which is more obvious once the lip has been repaired.
The nasal deformity varies in unilateral cleft lip and Bilateral cleft lip. The nasal deformity has characteristic features, but the severity varies and is related to the extent of the lip deformity and alveolar cleft.
Unilateral cleft lip nasal deformity etiology
It may be the result of the following:
1. Tissue deficiency of the cleft lip
2. Deficiency of the maxilla
3. Abnormal muscular pull on the nasal structures
Unilateral cleft lip nasal deformity etiology may cause due to the defects in the following components:
• Alar cartilage
• Nasal septum
• Columella
• Nasal tip
• Entire nasal pyramid
• Abnormal orbicularis muscle attachments
• Hypoplastic maxilla
Pathologic anatomy:
• Nasal tip is deflected towards the cleft side
• The dome on the cleft side is retro-displaced
• The angle between the medial and lateral crura is excessively obtuse
• Alar buckles inwards on the cleft side
• Alar-facial grove on the cleft side is absent
• Real or apparent maxillary deficiency
• Circumference of the naris is greater on the cleft side
• Naris on the cleft side is retro-displaced
• Columella is shorter in the antero-posterior dimension on the cleft side
• Medial crus is displaced on the cleft side
• Columella is positioned obliquely with its base toward the noncleft side
• Absence of the nasal floor
• Hypertrophy of the inferior turbinate on the cleft side
• Vestibular web- within the cleft side of interior nostril
A characteristic nasal deformity, which is usually symmetric, hence reconstruction is much easier than that of a unilateral cleft lip nasal deformity.
Etiology: several hypotheses
• Lateral traction on the alar bases and lowering of the ala due to abnormal muscle insertions
• Overgrowth of the mesoderm at the vomeropremaxillary suture due to lack of restraint by the non-united orbicularis oris muscle
• Incorporation of prolabium into the lip repair
Pathologic anatomy:
• A short columella with encroachment of the lip tissue, especially in a protruded premaxilla
• Medial crura of the alar cartilages are displaced inferiorly with lowering of the alar domes
• Alar domes are laterally displaced on a hypoplastic maxilla resulting in a widened nostril
• Prominent vestibular skin webs and buckling of the lateral crura produce a collapsed nasal contour
• The caudal septum and under-developed anterior nasal spine are displaced inferiorly or laterally depending on the degree and asymmetry of the cleft
Neonatal splintage prior to lip repair may be helpful to correct these deformities, but difficult to practice because, it needs prolonged nasal splintage and non-compliance by the parents.
Surgical correction
Timing of the surgery:
Primary Rhinoplasty: If nasal deformity is corrected along with the lip repair. Otherwise it is known as Secondary Rhinoplasty [1,2], which could be done during the school going age (5-6 years), early adolescence (10-12 years) or in adult age (above 18 years).
Primary Rhinoplasty can be done by closed approach, semi-open approach or open approach.
Primary cheilo-rhinoplasty-open approach: Proper reconstruction of the clefted musculo-apeneurotic complex by a subperiosteal dissection and placing the muscles in their proper anatomic and physiologic orientation after detaching from their abnormal insertions with adequate mobilization. Muscle Repair is the ‘key’ for the establishment of a normal nasolabial complex. Primary Rhinoplasty by delicate dissection and accurate repositioning of the lower alar cartilages during the primary lip repair enhances normal nasal shape and breathing [3-7].
Advantages:
• Identification and proper repositioning of the lower alar cartilages by accurately placed sutures under direct vision
• Approach of this procedure through the hidden rim incisions without any residual scars
• Septal cartilage can be easily dislocated and relocated into normal position without any resection
• Easy procedure comparable to the closed technique with a shorter operating time
• Procedure of choice where there is no preoperative orthodontic treatment or naso alveolar moulding.
Primary rhinoplasty by open approach with repair of unilateral complete cleft lip
The markings are made showing a modification of the Millard rotation-advancement technique and harashima open rhinoplasty technique as shown in Figures 1 and 2. A triangular flap of 2 mm is incorporated at the advancement flap (Millard B Flap) near the Vermillion to break the scar and subsequent scar contraction. Addition points (Philtro-columellar points) are also marked at the junction of the columellar and the philtrum on both the cleft and the non-cleft side. Millard C flap is drawn at the mucocutaneous junction of the rotation flap (Millard A Flap) at the level of the philtro-columellar angle with its base in continuity with the mucosal lining of the septum as mucocutaneous flap. From the philtro-columellar points, the incisions are extended in the nose as standard rim incisions through the edge of the columella, extending through the inside margin of the nostril rim upto its middle on the cleft and non-cleft side [8,9].
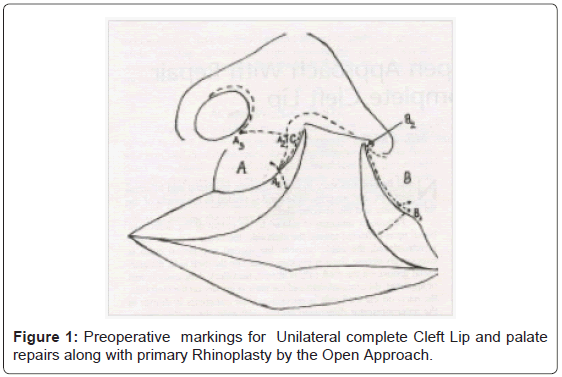
Figure 1: Preoperative markings for Unilateral complete Cleft Lip and palate repairs along with primary Rhinoplasty by the Open Approach.
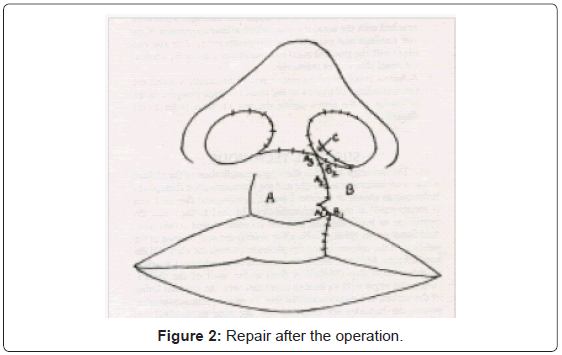
Figure 2: Repair after the operation.
Orbicularis oris muscles are radically mobilized from the vestibular nasal lining down to the edge of the bony cleft. The lateral nasal mucosa is elevated upward subperiosteally upto the inferior turbinate. The medial nasal septal mucosal flap is raised and extended posteriorly as a vomerine flap. Subperiosteal dissection of the cheek is performed widely from the anterior maxilla, respecting the inferior orbital nerve, to allow tension-free advancement of the soft tissue across the bony cleft. Columellar skin is dissected upward along the rim incision to expose the medial crura of the alar domes. Care is taken to free the fibrofatty tissue between the domes of the alar cartilage and to leave attached to the overlying skin. The nasal skin is dissected widely over the nasal skeleton to allow redraping over the reconstituted nasal tip. The nasal septum is dislocated from its base to provide a symmetrical appearance of the nostrils.
Suturing begins with the repair of the anterior palate. The vomerine flap and lateral nasal mucosa are approximated to reconstruct a nostril tube. The C flap is incorporated into the nostril sill, which is an important step to avoid stenosis of the nostril. Lip repair is carried out in the conventional manner as in the Millard rotation-advancement technique. The length of the rotation flap A (A1+A2+A3) is equal to the length of the advancement flap B (B1 and B2). The role of the triangular flap is mentioned earlier. Union of the orbicularis muscle from the cleft and non-cleft sides without tension should be given adequate emphasis.
The colemellar skin retracted with the skin hook. This maneuver tends to symmetrically align the alar cartilages. Four to five 5/0 Vicryl (Ethicon) sutures are used to suture the medical crura of the alar domes. The cranial edges of the lateral crura are sutured, securing the upward rotation of the lateral crura on the affected side (Figures 3 and 4). Finally, the nasal and the columellar incisions are sutured.
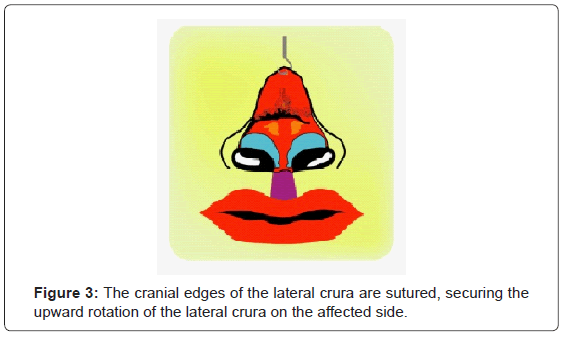
Figure 3: The cranial edges of the lateral crura are sutured, securing the upward rotation of the lateral crura on the affected side.
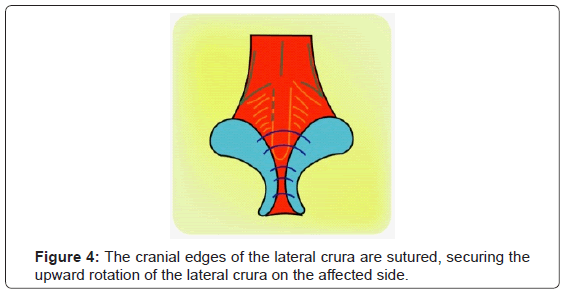
Figure 4: The cranial edges of the lateral crura are sutured, securing the upward rotation of the lateral crura on the affected side.
Transparent thin sterristrips are applied over the suture lines in the lip, followed by the application of the nostril conformers. Skin sutures and nostril conformers are removed after a week under a short general anesthesia.
Primary rhinoplasty by open approach with repair of bilateral complete cleft lip
Pre-surgical orthodontic correction by means of strapping is given to bilateral cleft lip with protruded premaxilla. The markings are made showing a modification of the Millard rotation-advancement technique and Harashina open rhinoplasty technique as shown in Figures 1 and 2. Additional points (philtral-columellar Points) are also marked at the junction of the columella and the philtrum. The width of the prolabium is made the same as the width of the columella from the philtral-columellar points. These prolabial incisions are extended into the nose as standard rim incisions through the edges of the columella extending through the inside margins of the nostril rim up to its middle. The remaining prolabial skin is left attached to the skin of the membranous septum as 2 nasal septal mucosal flaps [10] (Figures 1 and 2).
Orbicularis oris muscles are radically mobilized from the vestibular nasal lining down to the edge of the bony cleft from the lateral lip elements. The lateral nasal mucosa is elevated upward subperiosteally up to the inferior turbinate. The medial nasal septal mucosal flap is raised and extended posteriorly as a vomerine flap. A central strip of the nasal septal mucosa at least approximately I cm in width is to be kept intact to preserve the blood supply of the premaxilla. Subperiosteal dissection of the cheek is performed widely from the anterior maxilla, respecting the inferior orbital nerve, to allow tension-free advancement of the soft tissue across the bony cleft (Figures 3-5).
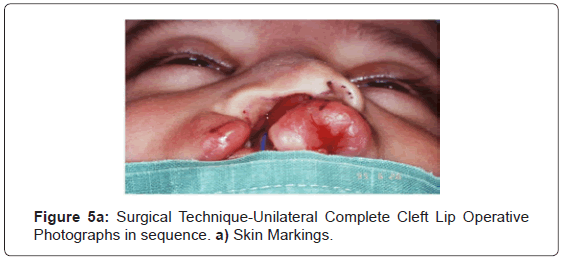
Figure 5a: Surgical Technique-Unilateral Complete Cleft Lip Operative Photographs in sequence. a) Skin Markings.
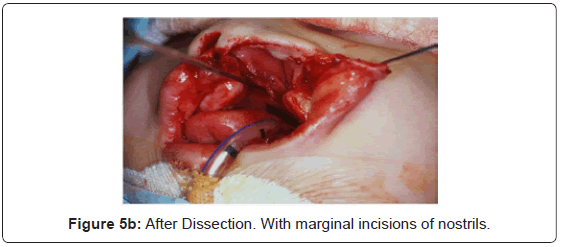
Figure 5b: After Dissection. With marginal incisions of nostrils.
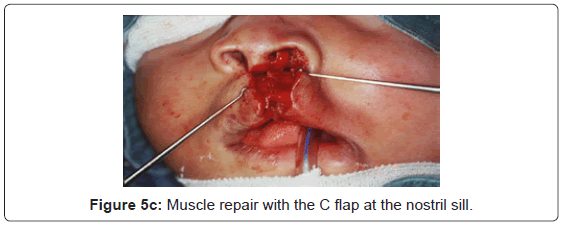
Figure 5c: Muscle repair with the C flap at the nostril sill.
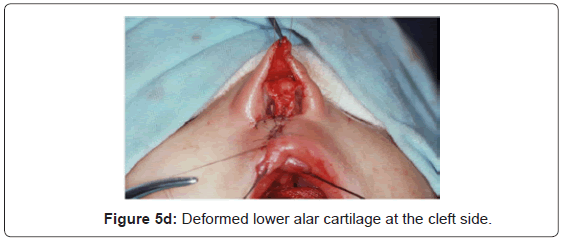
Figure 5d: Deformed lower alar cartilage at the cleft side.
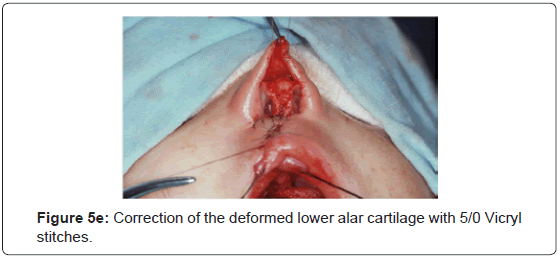
Figure 5e: Correction of the deformed lower alar cartilage with 5/0 Vicryl stitches.
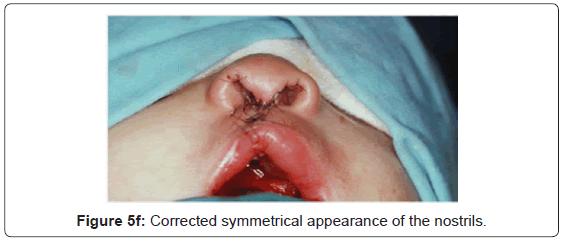
Figure 5f: Corrected symmetrical appearance of the nostrils.
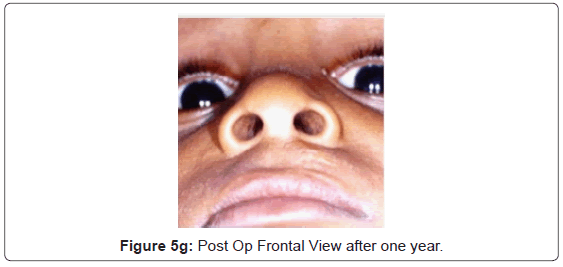
Figure 5g: Post Op Frontal View after one year.
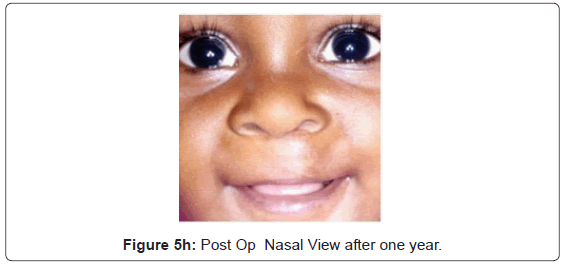
Figure 5h: Post Op Nasal View after one year.
The prolabial flap is reflected along with columellar skin by careful dissection especially at the base of the columella to dissect all fibrofatty soft tissue from the medial crura of the alar cartilages up to the dome and then from off the lateral crura, the septum, and upper lateral cartilages. Thus, the fibrofatty soft tissue is left attached to the elevated skin of the nose, which is dissected back to the dorsum of the nasal skeleton. The nasal skin is dissected widely over the nasal skeleton to allow red raping over the reconstituted nasal tip.
Suturing begins with the repair of the anterior palate. The vomerine flap and the lateral nasal mucosa are approximated to reconstruct a nostril tube on both sides. Lip repair is carried out in the conventional manner-first, the mucosa followed by the muscle repair. Union of the orbicularis oris muscle from both lateral elements across the premaxilla should be given adequate emphasis. The columellar skin is retracted with a skin hook, and this maneuver tends to symmetrically align the alar cartilages. Three to four 5/0 Vicryl (Ethicon) sutures are used to suture the medial crura and the alar domes. Cranial edges of the lateral crura are sutured securing the upward rotation of the lateral crus. The skin suturing is carried out with the prolabium to the lateral elements up to the philtral-columellar angle. Care should be taken to create an obtuse angle at the philtral-columellar junction by accurately placed sutures. The nasal and columellar skin incisions are sutured (Figures 6-8).
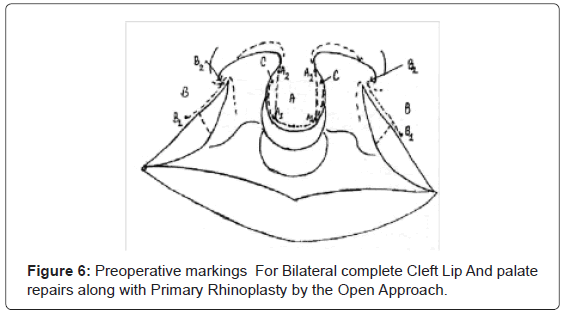
Figure 6: Preoperative markings For Bilateral complete Cleft Lip And palate repairs along with Primary Rhinoplasty by the Open Approach.
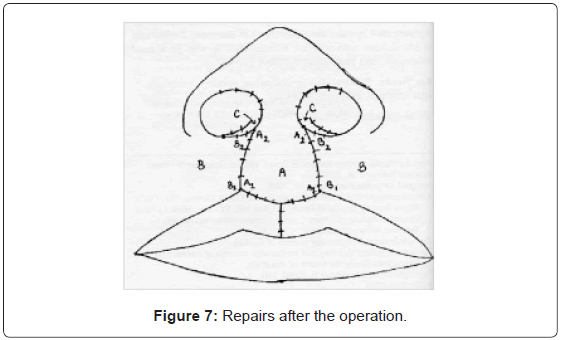
Figure 7: Repairs after the operation.
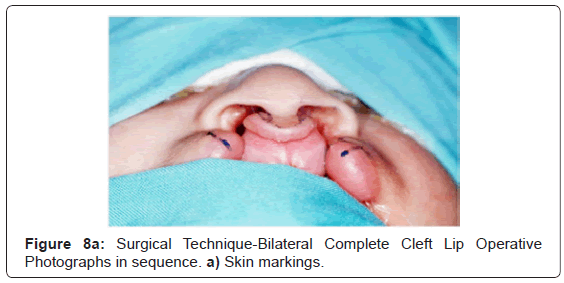
Figure 8a: Surgical Technique-Bilateral Complete Cleft Lip Operative Photographs in sequence. a) Skin markings.
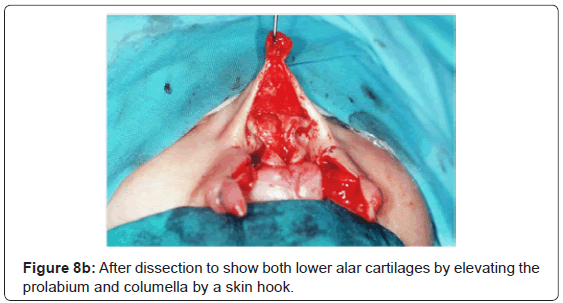
Figure 8b: After dissection to show both lower alar cartilages by elevating the prolabium and columella by a skin hook.
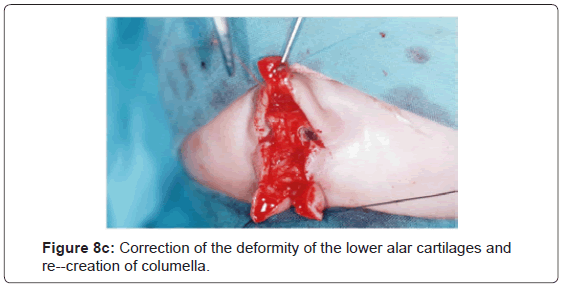
Figure 8c: Correction of the deformity of the lower alar cartilages and re--creation of columella.
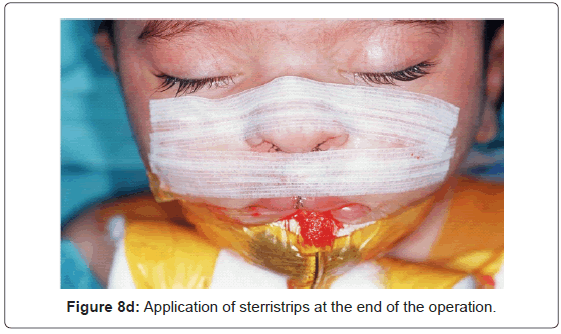
Figure 8d: Application of sterristrips at the end of the operation.
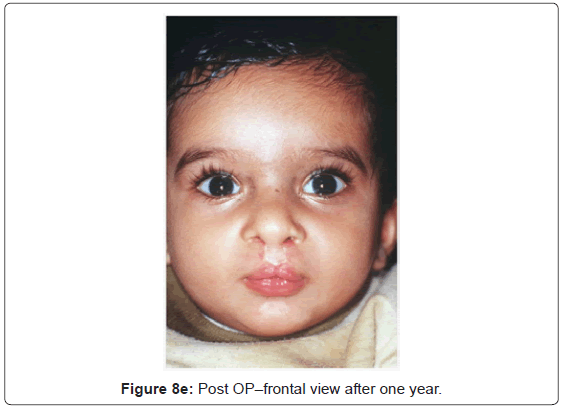
Figure 8e: Post OP–frontal view after one year.
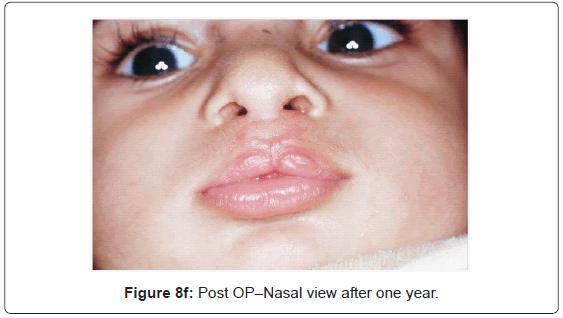
Figure 8f: Post OP–Nasal view after one year.
Cupid’s bow of the philtral column is formed by the advancement of the vermillion flaps from both lateral elements. The length of flap A (A1 to A2) is equal to the length of advancement flap B (B1 to B2). Transparent thin sterri-strips are applied over the suture lines in the lip followed by the application of the nostril conformers. Skin sutures and the nostril conformers are removed after a week under a short general anesthesia (Figures 9 and 10).
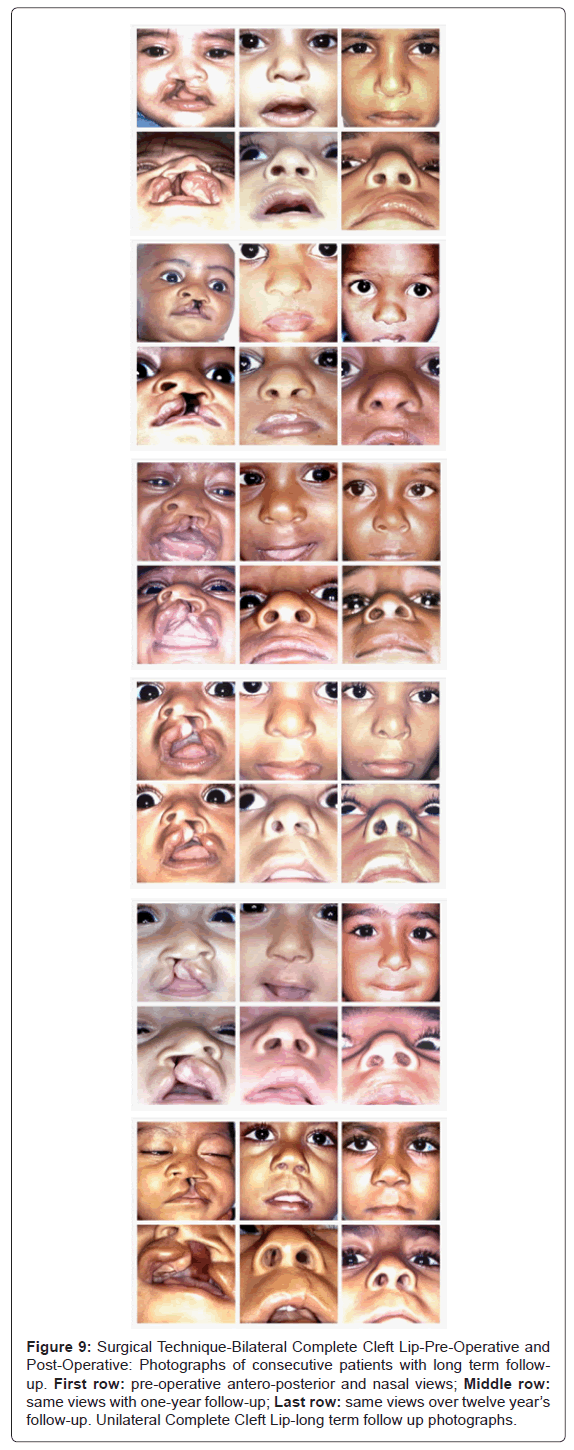
Figure 9: Surgical Technique-Bilateral Complete Cleft Lip-Pre-Operative and Post-Operative: Photographs of consecutive patients with long term followup. First row: pre-operative antero-posterior and nasal views; Middle row: same views with one-year follow-up; Last row: same views over twelve year’s follow-up. Unilateral Complete Cleft Lip-long term follow up photographs.
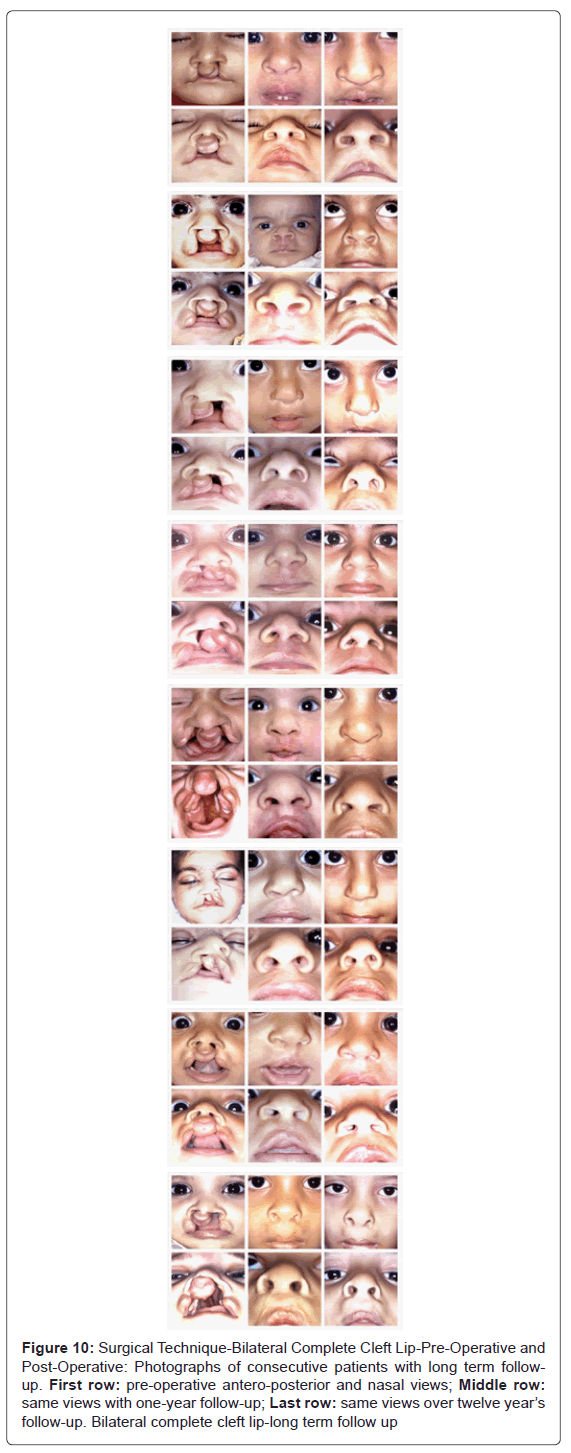
Figure 10: Surgical Technique-Bilateral Complete Cleft Lip-Pre-Operative and Post-Operative: Photographs of consecutive patients with long term followup. First row: pre-operative antero-posterior and nasal views; Middle row: same views with one-year follow-up; Last row: same views over twelve year’s follow-up. Bilateral complete cleft lip-long term follow up
Nostril conformers encourage the proper nasal contours and keep up the patency of the nostrils for breathing (Figures 11 and 12).
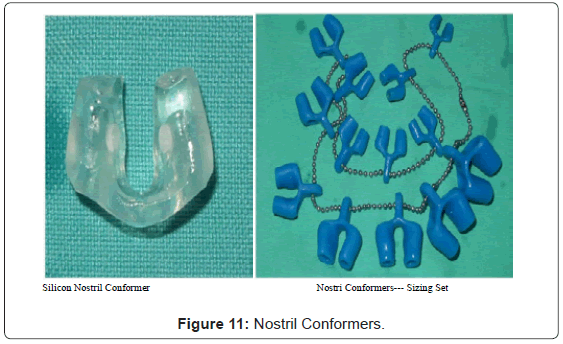
Figure 11: Nostril Conformers.

Figure 12: Application of Nostril Conformer after cleft lip repair.