Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2014) Volume 3, Issue 3
Antiretroviral treatments adverse effect is one of the challenges in HIV/AIDS prevention and control programs. The major objective of this study was assessment of the level of ART adverse effect and its associated factors among people living with HIV (PLWH) on ART in Debre Markos Referral Hospital from October 2 to November 30/2013. Institutional based cross-sectional quantitative type of study design was conducted to determine the level of ART adverse effect among randomly selected 373 adult PLWH on ART in Debre Markos referral hospital. The study participants were selected using systematic random sampling technique. Both primary and secondary data were gathered using a structured questionnaire. The collected data were entered, processed and analyzed in STATA V.11. The period prevalence of ART adverse effect was 51. 4%. The most common type of adverse effect was lipoathrophy (37.5%, n=72) and the least was Hepathotoxicity (0.52 %, n=1). The odds of ART adverse effect were 0. 523 times less likely among those who were literate compared to illiterate [AOR=0.477, 95% CI=0.28-0.812]. similarly, it was 0.44 times less likely among the study par-ticipants with preparatory school level of educational status compared to those with primary school [AOR=0.56, 95% CI=0.443-0.953]. The odds of ART adverse effect were 0.725 times less likely among those had a monthly income of ≥ 3551 Ethiopian Birr compared to those had no a regular monthly income [AOR=0.275,95%CI=0.098-0.773] and were 0.546 times less likely among substance non-abusers than abusers [AOR=0.454,95%CI=0.253-0.817]. The prevalence of ART adverse effect in Debre Markos referral Hospital was found. The leading adverse effect was Lipoathrophy. Factors such as educational status, income and substance abuse were identified independent determinants of ART adverse effect. The program managers, implementers and service providers need to take in to consideration the emerging need of adult education, health education and creation of income generating activities for adult PLWHs on ART in Debre Markos Referral Hospital. Furthermore it is better to disseminate information on the possible Antiretro-viral therapy adverse effects using leaflets and patient- physician regular education program.
<Keywords: People living with HIV; Adverse drug effect; ART; Debre Markos Referral Hospital
Human Immunodeficiency Virus (HIV) that causes AIDS is one of the world’s most serious health and development challenges. There are approximately 34million people currently living with HIV and nearly 30 million people have died of AIDS-related causes since the beginning of the epidemic. There were about 2.5 million new infections in 2011 or more than 7,000 new HIV infections per day, globally [1].
The discovery of antiretroviral therapy (ART) was a breakthrough in reducing mortality and improving the quality of life of People Living with HIV (PLWH). Today, antiretroviral therapy (ART) has become an integral part of the continuum of HIV prevention and care. The primary goals of HAART are maximal and durable suppression of viral replication, restoration of immunologic function, reduction of HIVrelated morbidity and mortality, improvement of quality of life and prolong survival [2,3].
Maximal and durable suppression of plasma viremia delays or prevents the selection of drug-resistance mutations, preserves CD4 T-cell numbers, and confers substantial clinical benefits, all of which are important treatment goals. Achieving viral suppression requires the use of ARV regimens with at least two, and preferably three, active drugs from two or more drug classes.
To Start
(Initial Combination Regimens for the Antiretroviral- Naive Patient); a baseline resistance testing and patient characteristics should guide design of the specific regimen. When initial suppression is not achieved or is lost, rapidly changing to a new regimen with at least two active drugs is required. The increasing number of drugs and drug classes makes viral suppression below detection [4].
Highly active Antiretroviral Therapy (HAART) is defined as
Two/more Nucleoside Reverse Transcriptase inhibitors (NRTIs) in combination with at least one Protease Inhibitor (PI) or one Non- Nucleoside Reverse Transcriptase inhibitor (NNRTI); alternatively it might be one NRTI in combination with at least one PI and one NNRTI; or an Abacavir/Tenofovir containing regimen of three or more NRTs in the absence of both PIs and NNRTs [5]. Adverse drug reactions (ADRs) are hard to avoid and can make life difficult. As a result, treatment of HIV infection has become a complicated balancing act between the benefits of durable HIV suppression and the risks of drug toxicity. In fact, ADRs are one of the main reasons why people living with HIV start missing doses of their medications or stop taking their drugs completely [6].
First-line drug toxicities fall into two categories
Early, usually presenting in the first few weeks to months of therapy, and later. Common early and potentially severe toxicities are hypersensitivity to NNRTIs (EFV and NVP), normally occurring within the first few weeks of therapy, and AZT-related anaemia and neutropenia, typically presenting in the first few months of therapy. Many of the acute toxicities, if not identified early, can evolve into lifethreatening and fatal events. Some of the higher mortality seen in the first six months of ART undoubtedly relates to drug toxicity [7].
The Non-Nucleoside Reverse Transcriptase Inhibitors (NRTI) such as
Zidovudin has side effects of anaemia, neutropenia, nausea, vomiting, headache, fatigue, myopathy, hepatitis, hyper pigmentation of oral mucosa and nail beds; Lamivudine , however is a safe drug in adolescent and adults. While, Tenofovir has side effects such as headache, diarrheal, nausea, vomiting, flatulence, renal toxicity, proteinuria, renal failure, decreased bone mineral density, risk of hepatitis B flare when stopped (also effective for treatment of hepatitis B). Didanosine is known to cause side effects of peripheral neuropathy, pancreatitis, gastrointestinal effects, retinal changes and optic neuritis. It has an increased risk of complications of non-cirrhotic portal hypertension when used in combination with stavudine. Abacavir might cause a potentially fatal hypersensitivity reaction; observational cohort studies found association between Abacavir plus Didanosine and myocardial infarction, but randomized studies have not yet confirmed [8].
The Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTI) such as
Enfavirenz has side effects of dizziness, insomnia, headache, inability to concentrate, abnormal dreams, CNS toxicity, teratogenicity and very rarely a fatal skin reaction (SJS). Nevirapian is also known to cause side effects of severe Hepathotoxicity, liver failure, and death; women with baseline CD4 cell count >250 per mm3 (0.25 × 109 per L) and men with baseline CD4 >400 per mm3 (0.40×109 per L) are at highest risk. Etravirine on the other hand has side effects such as nausea, peripheral neuropathy, hypertension, hypersensitivity reaction, increased liver function, and increased cholesterol and triglyceride levels [9].
Regarding the Protease Inhibitors
Indinavir is known with its side effects of indirect hyperbilirubinemia, kidney stones, renal insufficiency, alopecia, dry skin and mucous membranes, paronychia, ingrown toenails and gallstones. Whereas, Lopinavir has side effects like a potentially fatal pancreatitis and with long-term use, an increased risk of myocardial infarction. In addition, Ritonavir has an altered taste, circumoral and peripheral paresthesia side effects [8,9].
Magnitude of ADRs of ARV drugs not surprisingly, adverse drug reactions are common. Most adverse drug reactions are relatively mild, and many disappear when the drug is stopped or the dose is changed some gradually subside as the body adjusts to the drug. Other adverse drug reactions are more serious and last longer. Between 3% and 7% of hospital admissions in the United States are estimated to be for treatment of adverse drug reactions. Each time a person is hospitalized from the risk of having at least one adverse drug reaction was 10 to 20% [10].
A cohort study in India between 1996 and 2004, showed that among 1443 ART-naive patients received regimens containing d4T or AZT; rash (66%), Hepathotoxicity (27%) and anaemia (23%) were the most commonly faced toxicities [11].
In Abidjan, Côte d’Ivoire, 498 adults with a median baseline haemoglobin of 118 g/l started AZT + 3TC + EFV; 113 patients had grade 3/4 neutropenia and 23 had grade 3/4 anaemia. Of these patients, 80% were taking co-trimoxazole, which can cause anaemia and neutropenia [12].
A study conducted in Uganda and Zimbabwe, 219 of 3314 participants (6.6%) developed grade 4 anaemia at week 48; in the same study, Abacavir hypersensitivity reactions were reported in 2% of participants. It was indicated that gastritis (13.13%), rashes (8.75%), anaemia (8.13%), macula popular rashes (7.5%), giddiness (6.87 %), anorexia (6.87%) and paresthesia of legs (3.75%) were commonly reported ADRs. Out of 160 ADRs, 50 (31.06%) ADRs were belonging to gastrointestinal system. Use of the combination therapy of Zidovudin, Lamivudine and Nevirapian (ZDV+3TC+NVP) reported as a cause of majority of ADRs [13].
In Nairobi, Kenya, 284 patients received d4T + 3TC + NVP and the reported toxicity-free survival rate was 21% at 18 months. The risk of specific side effects varies from drug to drug, from drug class to drug class, and from patient to patient. In Tororo, Uganda, among 1073 patients on d4T + 3TC + NVP, nearly 50% of the patients experienced some form of toxicity by 18 months of treatment. Toxicity requiring a change in therapy occurred in 21% of the cohort, most commonly a switch from d4T to AZT. In a report from Khayelitsha, South Africa on 1700 patients receiving ART, one agent was substituted in approximately 10% because of toxicity. The rates were similar for d4T (8.5%), AZT (8.7%) and NVP (8.9%) [14,15].
Recommended single-drug substitutions for specific side effects with combination therapy
To the regimen d4T/3TC/NVP, if d4T-related neuropathy or pancreatitis; d4T related lipoathrophy; NVP related severe Hepathotoxicity; NVP-related severe rash (but not life threatening); and NVP-related life threatening rash (Stevens-Johnson syndrome) side effects are face, it was recommended substitute of d4T to ZDV, d4T to TDF or ABC, NVP to EFV (except for early pregnancy), NVP to EFV and NVP to PI. Regarding the regimen D4T/3TC/EFV; when d4Trelated neuropathy or pancreatitis and EFV-related persistent CNS toxicity are faced; it was recommended to substitute d4T with ZDV and EFV with NVP. With respect to ZDV/ddl/Lopinavir/Ritonavir treatment regimen, whenever ZDV related anaemia or neutropenia, ddI related pancreatitis or hepatitis, LPV/r related GIT symptoms and LPV/r related hypercholesterolemia, Lipodystrophy, impaired glucose tolerance are faced; it was advisable to substitute ZDV with d4T and consult expert [16].
With an estimated 1.1 million people living with HIV, Ethiopia has one of the largest populations of HIV infected people in the world. However, HIV prevalence among the adult population is lower than many sub-Saharan African countries. Adult HIV prevalence is currently estimated to be between 1.4% and 2.8%. A new single point estimate of HIV prevalence was generated following the completion of a population-based sero-survey in late 2010 [2].
Ethiopian government has made concerted and sustained effort over the last several years to introduce and scale-up counselling and testing services and use of antiretroviral drugs both for treatment and prophylaxis. A National Guideline on the use of ARV drugs was developed and the Antiretroviral Treatment (ART) programme was launched in 2003. Subsequently, in 2004, a free ART programme was initiated in three government hospitals in Addis Ababa [17].
The recommended drug regimens for adults and adolescents are TDF/ ZDV combined with 3TC+NVP or EFV as first line and ABC or TDF or ZDV (if not taken) with ddI, and LPV/r or SQV/r or NFV or IND/r as second line regimen. Measurement of peripheral blood CD4 cells is probably the most important laboratory assay for evaluation and monitoring of patients with HIV. The CD4 count is critical for determining the clinical stage of HIV infection, for deciding when to start antiretroviral therapy (ART), for evaluating the efficacy of treatment, and for changing the medications when necessary. Most HIV treatment decisions are therefore based upon the CD4 count [18].
Formerly, a patient with a CD4 count below 200 cells per micro Litter of blood is recommended to start ART. However, at this level of CD4 count a patient is at increased risk of developing life-threatening opportunistic diseases. To ensure patient safety, treatment must not be delayed until CD4 count falls below 200. The optimum time to initiate ART is when a patient’s CD4 count is 200-350. CD4 count levels do not determine treatment initiation in stage IV patients; regardless of CD4 count, stage IV patients are promptly started on ART, once readiness is assured. In stages I and II, immunological assessment is important to initiate ART; in stage III, treatment can be considered under certain clinical conditions with CD4 count of 350 and below. All stage III patients with a CD4 of 350 or below are recommended for initiation of ART to avoid confusion with advanced and early stage III [19].
The expansion of ART services has been rapid in Ethiopia. The HIV counselling and testing (HCT) program has shown considerable improvement both in terms of service expansion as well as utilization. The launch of free-of-charge ART in 2005, followed by the expansion of ART to health centres in 2007 significantly improved access to treatment. A total of 5.8 million people (53% male) received HIV counselling and testing in 2008/09, this is a 22% increase from the previous year. By the year 2009, 210,637 individuals had ever started ART and were accessed treatment at 481 facilities. ART coverage increased from 46% in 2008 to 53% 2009. In addition, the pre-ART program has thus, far captured 379,800 PLWHAs in chronic care follow-Up, Currently, 176,644 are on ART; however, lost to follow up to ART service was 28% by the end of 2008 [2,20].
Despite all the efforts made and achievements gained, Ethiopia has now thousands of patients on ART. Most initial regimens used in ARV scale-up since 2003 have included AZT with 3TC and NVP or EFV. The predominant toxicities from the use of these drugs have included the adverse effects expected in other settings, e.g. anaemia, peripheral neuropathy, lactic acidosis, and, in cohorts with more than one year of treatment, lipoathrophy. Moreover, There are evidences that ART drugs do have negative impacts resulted in increased prevalence of Rash, lipoathrophy, peripheral neuropathy, renal toxicity. An assessment of adherence to antiretroviral therapy among 422 patients on ART at the Ministry of National Defence Force Hospitals showed that 221(54.0%) developed mild adverse drug reactions. A study further examined the influence of age, HAART and specific antiretroviral drugs on risk of ADR in HIV-infected individuals [7,21,22]. In spite of few researches on areas of adherence that mentioned ADRs as a cause for noncompliance, there is no study conducted to assess the magnitude and factors of ADRs among AIDS patients on ART in the study area. Hence, this study hoped to contribute a lot for health care provider, health researchers and police makers with its provision of the magnitude of a specific ART drug, commendable solutions to systematically address the problem, further search and develop a relevant and context specific policy aimed at an improved management of ART adverse reaction in health care setting.
◊ To determine the prevalence of ART adverse effect among adult HIV/AIDS Patients on ART in Debre Markos Referral Hospital.
◊ To identify factors associated with ART adverse effect among adult HIV/AIDS Patients on ART in Debre Markos Referral Hospital.
Study area and setting
The study was conducted in Debre Markos Referral Hospital which was one of the two in East Gojjam Zone and of the eleven Hospitals in Amhara Region. It is one of the early established Governmental Hospitals. It was located 300 and 265 kilometres away from the capital city of Ethiopia (Addis Ababa) and Amhara Region (Bihar Dar), respectively. The Hospital is found in Debre Markos Town in an area of 18915 square meters. This hospital renders comprehensives HIV/ AIDS related services including VCT, PITC (provider initiated testing and counselling), PMTCT and ART program. The Hospital has a catchment population of 3.5 million with nearly 1:1 male to female ratio. Currently, there are about 2779 HIV/AIDS patients attending ART in the hospital.
Study design and Population
Institutional based cross sectional survey was conducted. The target (source population) of this study was all adult (age >15 years old) known HIV/AIDS patients’ on ART follow up in Debre Markos Referral Hospital. While all adult cases of HIV/AIDS on ART follow up for at least six months in the Hospital were the study population. Depending on the data that were obtained from patient/client charts and cards of the Hospital, magnitude and risk factors of specific Drug Adverse Effect were analyzed. The data which were record at the time of study was compared with the regional states and the national level.
Sample size and sampling
Sample size was determined using a single population proportion formula; considering 5% marginal error, 95% level of confidence and 50% prevalence of ADR among Adult HIV/AIDS patients on ART. Correcting for finite population and 10% for possible none response rate, 373 randomly selected cases of HIV/AIDS patients on ART were included in the study. Total HIV/AIDS patients on ART in DMRH were 2779 & the required Sample size was 373.Taking a sampling fraction of 7 (2779/373), a random start of card number 2 was selected with lottery method. having, the daily patient flow on average of 60 and a sampling frame of the patient card number, starting from the first date to the last 44th date of data collection, every 7th patient’s cards (a total of nine) were selected at every working day and distributed to the ART clinic OPDs for data collectors until a sample size of 373 was fulfilled.
Variables and measurement
The dependent variable was presence of ART Adverse Effect, while the independent variables were socio-demographic characters: Age, sex, educational status, Income, CD4, nutritional status. Behavioral Factors: smoking, alcohol drink, chat chewing, physical exercise, income, Nutritional Status, CD4 count. Drug adverse effect is defined as any response to a drug that is noxious, unintended and occurs at doses used in man for prophylaxis, diagnosis or therapy (WHO). Data about presence of ADR to a specific ART were obtained from participants medical chart. Side effects are problems that occur when treatment goes beyond the desired effect or problems that occur in addition to the desired therapeutic effect. ART is combination of three antiretroviral drugs given to HIV/AIDS patients eligible for treatment according to the national guideline. Anemia is the presence of at least one documented hemoglobin value of ≤ 10 mg/dl after having started ART. (Severe anemia is defined as less than 7 g/L) [11]. Peripheral Neuropathy is the presence of documented persistent pain, numbness, tingling or burning sensation on the extremities or the presence of any documented peripheral neuropathy in the charts after started on ART.
Skin rash is the presence of documented generalized mildly itchy or non pruritic urticarial, erythematous or maculopapular rash, which may have vesicular lesion and desquamative lesions over the mucous membranes in severe cases, or the presence of documented skin rash after started on ART. Operationally defined study variables were and measured using a carefully designed structured questionnaire and a check list after consultation of related literatures in line with the study objectives.
Data collection methods
Both primary (of patient interview) and secondary (of patient cards) data sources were used. A pre-tested, structured and interview administered questionnaire, translated into Amharic language was used to collect primary data from the study subjects, while a check list was used to collect data from medical charts/patient cards/hospital registers of the study subjects. Five diploma holder nurses working in ART clinic were trained and collected the data from October 2 to November 30/2013. The principal investigator regularly supervised the data collection process. Checking of questionnaires before, during and at the end of each day of data collection for consistency, completeness, clarity and accuracy was made.
Data processing and analysis
The data gathered were coded, entered; cleaned, recoded using SPSS version 16 statistical packages and analysis was started. The Period prevalence rate of ART Adverse Effects among the study subjects was estimated using simple descriptive summary statistics such as frequency and proportion. Similarly, the magnitude of independent study variables was summarized using numerical summary measures. Tables and graphs were used to present the result of the analyzed data. Odds ratio was calculated to assess the possible statistical association between presence of ART adverse effect and selected explanatory variables at 5% level of significance. A multivariable analysis using logistic regression was made to identify possible independent determinants of ART adverse effect. Finally, a best fitted regression model was developed.
Ethical clearance
Ethical clearance was requested and approval was obtained from Debre Markos University, Health Sciences College Ethical Review Committee. A letter of permission was submitted to Debre Markos Referral Hospital medical director office prior to the beginning of undertaking the study. All the study participants were informed about the purpose of the study, their right to refuse was maintained and informed written (signed) consent was obtained from each study participant. Ethical conduct was maintained during data collection and throughout the research process. To ensure confidentiality anonymous type interview was followed.
Socio-demographic characteristics of PLWHAS on ART
Among 373 study subjects, included in the study, data were collected from all of them; this made the response rate to be 100%. Most (36.7%, n=137) study participants were within the age group of 26-35, followed by 36-45 years old age group (34.2%, n=121). The mean age was 39.2 years, + 1.06 S.D. The majority (62.7%, n=234) were females. Nearly half (49.9%, n=186) and only 11.3 %( n=42) were married and not married, respectively. While most (39.1%, n=146) were able to read and write only. Above half (52.3%, n=195) and few (4.8%, n=18) had no regular income and had an estimated income of 2351 to 3550 ETB per month, respectively. Slightly, higher a quarter (26.3%, n=98) were government employed, followed by housewives (15%, n=56). Most (96.2%, n=359) were Orthodox Christian in religion and Amhara (98.4%, n=367) in Ethnicity (Figure 1 and Table 1).
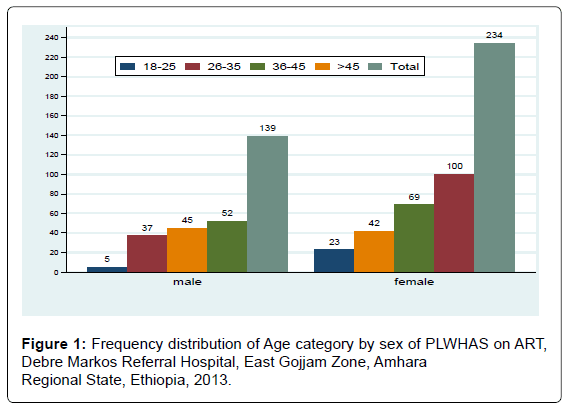
Figure 1: Frequency distribution of Age category by sex of PLWHAS on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara Regional State, Ethiopia, 2013.
| Characteristics | Frequency | Percent |
|---|---|---|
| Marital status | ||
| Never married | 42 | 11.30 |
| Married | 186 | 49.90 |
| Divorced | 58 | 15.50 |
| Widowed | 87 | 23.30 |
| Educational status | ||
| Literate | 216 | 57.90 |
| Illiterate | 157 | 42.10 |
| Religion | ||
| Orthodox | 359 | 96.20 |
| Others | 14 | 3.80 |
| Ethnicity | ||
| Amhara | 367 | 98.40 |
| Others | 6 | 1.60 |
| Income | ||
| No regular income | 195 | 52.30 |
| ≤650 | 64 | 17.20 |
| 651-1400 | 35 | 9.40 |
| 1401-2350 | 35 | 9.40 |
| 2351-3550 | 18 | 4.80 |
| ≥3551 | 26 | 7.00 |
| Occupation | ||
| Government employee | 98 | 26.30 |
| Merchant | 65 | 17.40 |
| Housewife | 56 | 15.00 |
| Private business | 55 | 14.70 |
| Daily labourer | 31 | 8.30 |
| Non-employee | 31 | 8.30 |
| Others | 37 | 9.90 |
Table 1: Socio-demographic characteristics of PLWHAS on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara National Regional State, Ethiopia, 2013.
ART Adverse Effect among PLWHs
Half of (51.47%, n=192) the participants had faced at least one of the ART induced adverse effects. Of the adverse effects, lipoathrophy was the most (37.5%, n=72) prevalent, followed by peripheral neuropathy, anemia and dermatitis/skin rash with their respective prevalence’s of 23.96% (n=46), 14.06% (n=27) and 13.02 %( n=25). The least frequently occurred, ART induced adverse effect, was Hepathotoxicity with a prevalence rate of 0.52% (n=1) next to renal toxicity (3.65%, n=7) and mental disorder (6.25%, n=2), respectively (Table 2 and Figure 2).
| Variables | Frequency | Percent |
|---|---|---|
| ART adverse effect | ||
| Yes | 192 | 51.47 |
| No | 181 | 48.53 |
| Lipoathrophy | ||
| Yes | 72 | 37.50 |
| No | 120 | 62.50 |
| Peripheral neuropathy | ||
| Yes | 46 | 23.96 |
| No | 146 | 76.04 |
| Anaemia | ||
| Yes | 27 | 14.06 |
| No | 165 | 85.94 |
| Dermatitis/skin rash | ||
| Yes | 25 | 13.02 |
| No | 167 | 86.98 |
| Mental disorder | ||
| Yes | 12 | 6.25 |
| No | 180 | 93.75 |
| Renal toxicity | ||
| Yes | 7 | 3.65 |
| No | 185 | 96.35 |
| GI intolerance | ||
| Yes | 2 | 1.04 |
| No | 190 | 98.96 |
| Hepathotoxicity | ||
| Yes | 1 | 0.52 |
| No | 191 | 99.48 |
Table 2: Frequency distribution of ART adverse effects among PLWHAS on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara National Regional State, Ethiopia, 2013.
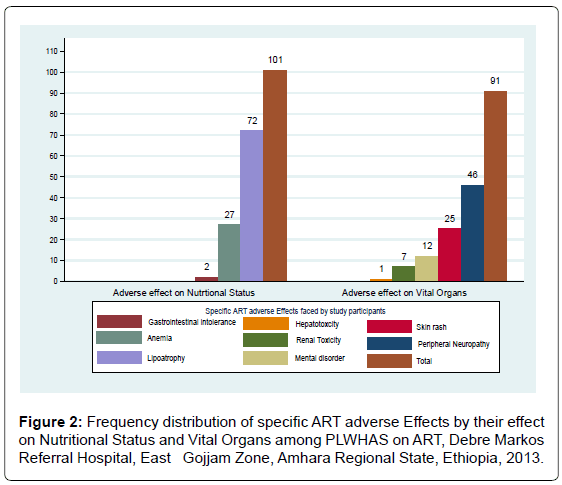
Figure 2: Frequency distribution of specific ART adverse Effects by their effect on Nutritional Status and Vital Organs among PLWHAS on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara Regional State, Ethiopia, 2013.
ART Adverse Effect on Nutritional Status of PLWHAs
Among 51.5% (n=192) ART adverse effect prevalent cases, effect on nutritional status contributed the majority (52.66%, n=101) with the most commonly observed effect on body fat distribution, lipoathrophy (71.29%, n=72) followed by effect on iron absorption, Anemia (26.73%, n=27) and the least on GI, GI intolerance (1.98%, n=2). Separate analysis of adverse effects on nutritional status in terms of body weight, blood sugar level and body fat status indicated that most(83.84%, n=83) were in the range of a normal weight (BMI=18.5- 24.9 kg/m2). However, about 3.03% (n=3) were in sever underweight (BMI<17 kg/m2), 7.07% (n=7) were underweight (BMI=17-18.49 kg/ m2) and the rest 6.06 % (n=6) were obese (BMI>/=25 kg/m2). Regarding blood sugar level, almost all 99.01% (n=100) were in the normal range (FBS=70-126 mg/dL). About 0.99 % (n=1) were hypoglycemic (FBS<70 mg/dL) respectively (Table 3 and Figure 2).
| Variables | Frequency | Percent |
|---|---|---|
| ART adverse effect on nutritional status | ||
| Yes | 101 | 52.66 |
| No | 91 | 47.34 |
| Lipoathrophy | ||
| Yes | 72 | 71.29 |
| No | 29 | 28.71 |
| Anaemia | ||
| Yes | 27 | 26.73 |
| No | 74 | 73.27 |
| GI intolerance | ||
| Yes | 2 | 1.98 |
| No | 99 | 98.02 |
| Weight loss | ||
| Sever underweight(BMI<17kg/m2) | 3 | 3.03 |
| Underweight (BMI=17-18.49kg/m2) | 7 | 7.07 |
| Normal weight(BMI=18.5-24.9kg/m2) | 83 | 83.84 |
| Obese /overweight(BMI ≥ 25kg/m2) | 6 | 6.06 |
| Blood sugar level | ||
| Hypoglycaemic (FBS<70mg/dL) | 1 | 0.99 |
| Normal(FBS=70-126mg/dL) | 100 | 99.01 |
Table 3: ART Adverse effect on nutritional status among PLWHAS on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara National Regional State, Ethiopia, 2013.
ART Adverse Effect on Vital Organs of PLWHAs
Of ART adverse effects, effect on vital organs was less (47.4%, n=91) prevalent, of which nearly half of the effect observed on Peripheral Nerves, peripheral neuropathy (50.55%, n=46) and the least effect on liver, Hepathotoxicity (1.1% n=1). Adverse effects on skin, brain and kidneys, such as dermatitis/skin rash, mental disorder and renal toxicity contributed 27.47 %( n=25), 13.19 % (n=12) and 7.69 % (n=7), respectively. Separate analysis of the level of blood pressure showed that most (83.52%, n=76) had had a normal range of 90/60 to 120/90 mmhg and few were hypertensive (16.48%, n=15) with more than 120/90 mmhg blood pressure (Table 4 and Figure 2).
| Characteristics | Frequency | Percent |
|---|---|---|
| ART adverse effect on vital organs | ||
| Yes | 91 | 47.34 |
| No | 101 | 52.66 |
| Peripheral neuropathy | ||
| Yes | 46 | 50.55 |
| No | 45 | 49.45 |
| Dermatitis/skin rash | ||
| Yes | 25 | 27.47 |
| No | 66 | 72.53 |
| Mental Disorder | ||
| Yes | 12 | 13.19 |
| No | 79 | 86.81 |
| Renal toxicity | ||
| Yes | 7 | 7.69 |
| No | 84 | 92.31 |
| Hepathotoxicity | ||
| Yes | 1 | 1.10 |
| No | 90 | 98.90 |
| Blood pressure | ||
| Normal | 76 | 83.52 |
| Hypertension | 15 | 16.48 |
Table 4: ART adverse effect on Vital Organs among PLWHAS on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara National Regional State, Ethiopia, 2013.
ART year of Initiation, type of Regimen and HAART combination
Most (23.06%, n=86) study subjects started ART in the year 2011, and the least (11.53%, n=43) in 2006 G.C. Among those who started in the year 2011G.C, about 10.72% (n=40) and in the year 2006 G.C, 5.09% (n=19) developed at least one of the ART adverse effects. Nearly all (98.66%, n=368) of the study subjects were on the first line ART regimen, of which more than half (50.67%, n=189) faced at least one of the ART adverse effects. Of the study subjects, most (96.51%, n=360) did not know the type of ART they were taking, among which 49.06% (n=183) faced ART adverse effect. The majority (34.58%, n=129) were on a HAART combination of Tenofovir, Lamivudine and Enfavirenz (TDF, 3TC & EFV), of which 14.75% (n=55) faced ART adverse effect. Only one of the study subjects was on a HAART combination of Tenofovir, Abacavir and Caletra, who was among those faced adverse effect. Similarly, three of the study subjects were on a combination of Tenofovir, Lamivudine and Caletra and all developed at least one of the ART adverse effects (Table 5 and Figure 3).
| Variables | ART adverse effect | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | |||||||||||
| Male | Female | Total | Male | Female | Total | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Year of ART start | ||||||||||||
| 2006 | 10 | 5.21 | 9 | 4.69 | 19 | 9.90 | 8 | 4.42 | 16 | 8.84 | 24 | 13.26 |
| 2007 | 7 | 3.65 | 17 | 8.85 | 24 | 12.50 | 10 | 5.52 | 15 | 8.29 | 25 | 13.81 |
| 2008 | 15 | 7.81 | 34 | 17.71 | 49 | 25.52 | 9 | 4.97 | 13 | 7.18 | 22 | 12.15 |
| 2009 | 12 | 6.25 | 13 | 6.77 | 25 | 13.02 | 12 | 6.63 | 20 | 11.05 | 32 | 17.68 |
| 2010 | 14 | 7.29 | 21 | 10.94 | 35 | 18.23 | 8 | 4.42 | 24 | 13.26 | 32 | 17.68 |
| 2011 | 14 | 7.29 | 26 | 13.24 | 40 | 20.83 | 20 | 11.05 | 26 | 14.36 | 46 | 25.41 |
| ART Regimen | ||||||||||||
| First line | 70 | 36.46 | 119 | 61.98 | 189 | 98.44 | 65 | 35.91 | 114 | 62.98 | 179 | 98.90 |
| Second line | 2 | 1.04 | 1 | 0.52 | 3 | 1.56 | 2 | 1.10 | 0 | 0.00 | 2 | 1.10 |
| Know ART Reg. | ||||||||||||
| Yes | 3 | 1.56 | 6 | 3.13 | 9 | 4.69 | 2 | 1.10 | 2 | 1.10 | 4 | 2.21 |
| No | 69 | 35.94 | 114 | 59.38 | 183 | 95.31 | 65 | 35.91 | 112 | 61.88 | 177 | 97.79 |
| HAART taken | ||||||||||||
| AZT,3TC & NVP | 16 | 8.33 | 34 | 17.71 | 50 | 26.04 | 19 | 10.50 | 25 | 13.81 | 44 | 24.31 |
| AZT,3TC & EFV | 16 | 8.33 | 16 | 8.33 | 32 | 16.67 | 5 | 2.76 | 10 | 5.52 | 15 | 8.28 |
| TDF,3TC & NVP | 15 | 7.81 | 36 | 18.75 | 51 | 26.56 | 14 | 7.73 | 34 | 18.78 | 48 | 26.51 |
| TDF,3TC & EFV | 22 | 11.46 | 33 | 17.19 | 55 | 28.65 | 29 | 16.02 | 45 | 24.86 | 74 | 40.88 |
| TDF,3TC &Caletra | 2 | 1.04 | 1 | 0.52 | 3 | 1.56 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| TDF,ABC &Caletra | 1 | 0.52 | 0 | 0 | 1 | 0.52 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 |
| Total | 72 | 37.50 | 120 | 62.50 | 192 | 100 | 67 | 37.02 | 114 | 62.98 | 181 | 100 |
Table 5: Frequency distributions of ART year of start, type of Regimen and HAART combination by presence of ART Adverse effect and sex of PLWAs on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara Regional State, Ethiopia, 2013.
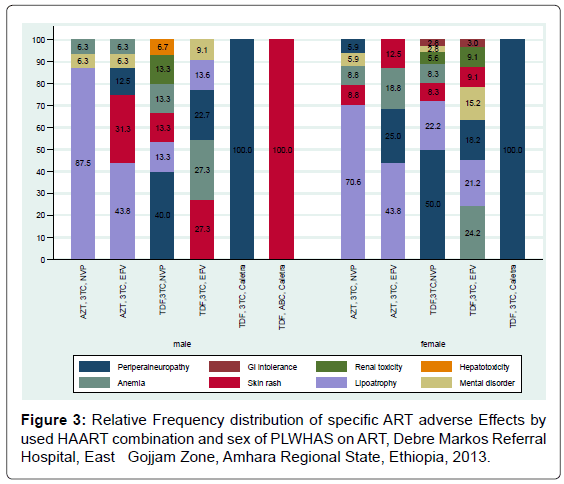
Figure 3: Relative Frequency distribution of specific ART adverse Effects by used HAART combination and sex of PLWHAS on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara Regional State, Ethiopia, 2013.
CD4 count
The median CD4 count before ART among the study subjects, who faced ART adverse effect, was 134 with a minimum, maximum and IQR of 5, 372 and 325, respectively. While after ART initiation, the median was 434, the minimum 5 and the maximum was 1415 with IQR of 1025. Similarly, among those who did not face ART adverse effect, the median CD4 count before ART was 131 with a minimum, maximum and IQR of 2, 506 and 295, respectively, while after ART initiation, the median was 414 with the minimum 38, the maximum 1415 and IQR of 989. Despite ART adverse effect, the median CD4 count had better improvement among Females than Males after ART initiation from the base line median CD4 count. Males with ART adverse effect had improved CD4 count from base line median of 103.5 to 345, the minimum from 11 to 5, the maximum from 372 to 806 and the IQR from 356 to 549. However, females CD4 count improved from base line median of 149.5 to 479, the minimum had no change from 5 to 5, the maximum from 339 to 1161 and IQR from 292 to 953 (Table 6).
| Variables | ART adverse effect | |||||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| Male | Female | Total | Male | Female | Total | |
| Median CD4 count | ||||||
| Before ART | 103.5 | 149.5 | 134 | 121 | 143 | 131 |
| After ART | 345 | 479 | 434 | 383 | 435.5 | 414 |
| Minimum CD4 count | ||||||
| Before ART | 11 | 5 | 5 | 2 | 16 | 2 |
| After ART | 5 | 5 | 5 | 38 | 66 | 338 |
| Maximum CD4 count | ||||||
| Before ART | 372 | 339 | 372 | 506 | 378 | 506 |
| After ART | 806 | 1161 | 1161 | 1246 | 1415 | 1415 |
| The 25th percentile of CD4 count | ||||||
| Before ART | 19 | 23 | 12 | 20 | 20 | 16 |
| After ART | 73 | 127 | 55 | 165 | 138 | 99 |
| The 75th percentile of CD4 count | ||||||
| Before ART | 218 | 315 | 337 | 297 | 296 | 311 |
| After ART | 622 | 1080 | 1080 | 761 | 1053 | 1088 |
| IQR of CD4 count | ||||||
| Before ART | 199 | 292 | 325 | 277 | 276 | 295 |
| After ART | 549 | 953 | 1025 | 596 | 915 | 989 |
Table 6: Frequency distributions of CD4 count summary statistics by ART Adverse effect and sex of PLWAs on ART, Debre Markos Referral Hospital, East Gojjam Zone, Amhara Regional State, Ethiopia, 2013.
Physical exercise, substance use and dietary habit
Among the study subjects, about 9.90% (n=37) were respond having experience of physical exercise, most (37.73%, n=20) had exercise for more than one hour per a day. Of those with ART adverse effects, 7.71 % (n=29) had exercise, of which 30 %(n=15) carried out exercise for more than one hour per a day. Few (1.07%, n=4) had history of cigarette smoking. Only one respondent (0.27%) responded that currently smoking. Regard to chat chewing; only one respondent (0.27%) responded that chew chat. Nearly one-sixth (16.35%, n=61) of the study subjects were respond drunk alcohol, of which most (85.25%, n=52) drunk every 2-4 days per week. The majority (68.90, n=257) had vegetable and fruit dietary habit, 95.72%, n=232) of them feed every 2-3 days per a week (Table 7).
| Variables | Frequency | Percent |
|---|---|---|
| Physical exercise | ||
| Yes | 37 | 9.90 |
| No | 336 | 90.10 |
| Frequency | ||
| <30 min | 16 | 30.19 |
| 30-60min | 17 | 32.08 |
| >60min | 20 | 37.73 |
| Cigarette smoking history | ||
| Yes | 4 | 1.07 |
| No | 369 | 98.93 |
| Chat chewing | ||
| Yes | 1 | 0.27 |
| No | 372 | 99.73 |
| Alcohol drinking | ||
| Yes | 61 | 16.35 |
| No | 312 | 83.65 |
| Frequency | ||
| Every day | 3 | 4.92 |
| 2-4 days per wk. | 52 | 85.25 |
| 5-6 days per wk. | 6 | 9.84 |
| Feed fruit/vegetables | ||
| Yes | 257 | 68.90 |
| No | 116 | 31.10 |
| Frequency | ||
| Every day | 11 | 4.41 |
| 2-3 days per wk. | 232 | 90.44 |
| 4-6 days per wk. | 14 | 5.15 |
Table 7: Frequency distributions of Physical exercise, Substance use and dietary habit among PLWHAs on ART, DMRH, East Gojjam Zone, Amhara National Regional State, Ethiopia, 2013.
Bivariate and multivariable analysis
Socio-demographic characteristics in relation to ART adverse effect: Even if sex had no statistically significant association, male respondents were 1.02 fold at risk of ART adverse effect compared to females [COR=1.02, 95% CI=0.67-1.55]. Similarly, those with in the age group of 25-35 years old were 1.04 times at high risk of ART adverse effect compared to those in the age group of 18-25 years old [COR=1.04, 95% CI=0.46-2.35]. Marital status of the respondents was not statistically, significantly associated with ART adverse effect. However, those who married were 26% at less risk of ART adverse effect than the never married once [COR=0.74, 95% CI=0.38-1.45]. Moreover; Religion, Ethnicity and occupation of the respondents were not significantly associated with ART adverse effect. Educational status, Level of literacy and Income of the respondents, however were statistically, significantly associated with ART adverse effect. Those who illiterate were 1.57 times at high risk of ART adverse effect than those who were literate [COR=1.57, 95%CI=1.04-2.38]. Literates to preparatory level were 83% at less risk of ART adverse effect compared to those who were in literacy level of write and read only [COR=0.17, 95% CI=0.09-0.34]. Respondents who had 3551 or more ETB per month income were 0.25 times at less risk of ART adverse effect compared to those who had no regular monthly income [COR=0.75, 95% CI=0.01 -0.65].
CD4 count and type of regimen in relation to ART adverse effect: CD4 count both before and after ART start was not statistically associated with ART adverse effect [COR=1.001, 95%CI=0.999- 1.004] and [COR=1, 95%CI=0.999-1.001] respectively. The odds of ART adverse effect were 0.70 times less likely among those who were on second line than those on first line ART regimen [COR=0.70, 95%CI=0.12-4.26].
Physical exercise, Substance use and dietary habit in relation to ART adverse effect: The odds of ART adverse effect were 52% less likely among those who had at least a half an hour daily physical exercise compared to those who had no physical exercise[COR=0.48,9 5%CI=0.23-0.97]. The odds of ART adverse effect were 46% less likely among those who did not use at least one of the substances (Chat, cigarette and alcohol) compared to those who did use[COR=0.54, 95%CI=0.32-0.91]. Those who had had fruit and vegetable diet for at least 2-3 days per a week were 37% less likely at risk of ART adverse effect than those who did not had [COR=0.63, 95%CI=0.4-0.98] (Table 8). Variables which were significant at P=0.05 level of significance in Bivariate analysis were further treated at multivariate analysis (Tables 8 and 9).
| Variables | ART adverse effect | COR(95%CI) | P-Value | |||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| n | % | n | % | |||
| Sex | ||||||
| Female | 120 | 32.17 | 114 | 30.56 | 1 | |
| Male | 72 | 19.30 | 67 | 17.96 | 1.02(0.67-1.55) | 0.923 |
| Age group | ||||||
| 18-25 | 15 | 53.60 | 13 | 46.40 | 1 | |
| 25- 35 | 72 | 52.60 | 65 | 47.40 | 1.04 (0.46-2.35) | 0.922 |
| 36- 45 | 61 | 50.40 | 60 | 49.60 | 1.14 (0.50-2.59) | 0.763 |
| >45 | 44 | 50.60 | 43 | 49.40 | 1.13 (0.48-2.65) | 0.783 |
| Marital status | ||||||
| Never married | 19 | 45.20 | 23 | 54.80 | 1 | |
| married | 98 | 52.70 | 88 | 47.30 | 0.74 (0.38-1.45) | 0.384 |
| divorced | 31 | 53.40 | 27 | 46.60 | 0.72 (0.32-1.60) | 0.418 |
| widowed | 44 | 50.60 | 43 | 49.40 | 0.81 (0.39-1.69) | 0.570 |
| Religion | ||||||
| Orthodox | 184 | 51.30 | 175 | 48.70 | 1. | |
| Others | 8 | 57.10 | 6 | 42.90 | 0.79(0.27-2.32) | 0.665 |
| Ethnicity | ||||||
| Amhara | 189 | 51.50 | 178 | 48.50 | 1 | |
| Others | 3 | 50.00 | 3 | 50.00 | 1.06(0.21-5.33) | 0.942 |
| Occupation | ||||||
| Gov’t employed | 52 | 53.10 | 46 | 46.90 | 1 | |
| Merchant | 33 | 50.80 | 32 | 49.20 | 0.81(0.42-1.58) | 0.542 |
| Housewife | 27 | 48.20 | 29 | 51.80 | 1.21(0.63-2.34) | 0.563 |
| Daily labourer | 19 | 61.30 | 12 | 38.70 | 1.10(0.59-2.05) | 0.918 |
| Non-employed | 9 | 29.00 | 22 | 71.00 | 0.71(0.31-1.63) | 0.774 |
| Others | 20 | 54.10 | 17 | 45.90 | 0.96(0.45-2.05) | 0.423 |
| CD4 count before ART | 192 | 51.50 | 181 | 48.50 | 1.001 | 0.402 |
| CD4 count after ART | 192 | 51.50 | 181 | 48.50 | 1.00 | 0.503 |
| Type of ART regimen | ||||||
| First line | 189 | 51.40 | 179 | 48.60 | 1 | |
| Second line | 3 | 60.00 | 2 | 40.00 | 0.70(0.12-4.26) | 0.701 |
Table 8: Socio-demographic characteristics in relation to ART adverse Effect, DMRH, EGZ, ANRS, Ethiopia, 2013.
| Variables | ART adverse effect | COR(95%CI) | AOR(95%CI) | P-Value | |
|---|---|---|---|---|---|
| Yes (n) | No (n) | ||||
| Educational status | |||||
| Illiterate | 91 | 66 | 1 | 1 | |
| Literate | 101 | 115 | 1.57(1.04-2.38) | 0.477(0.28-0.812) | 0.006* |
| Level of Literacy | |||||
| Read and write only | 11 | 4 | 1 | 1 | |
| Primary | 54 | 40 | 0.20(0.06-0.69) | 0.34(0.021-5.66) | 0.334 |
| Secondary | 61 | 19 | 0.41(0.23-0.74) | 0.67(0.177-2.547) | 0.559 |
| Preparatory | 32 | 57 | 0.17(0.09-0.34) | 0.56(0.443-0.953) | 0.009* |
| Certificate and above | 34 | 61 | 0.99(0.54-1.81) | 0.19(0.013-0.219) | 0.024 |
| Income | |||||
| No regular income | 89 | 106 | 1 | 1 | |
| ≤650 | 37 | 27 | 0.61(0.35-1.08) | 0.569(0.30-1.08) | 0.084 |
| 651-1400 | 18 | 17 | 0.79(0.39-1.63) | 0.615(0.267-1.42) | 0.254 |
| 1401-2350 | 19 | 16 | 0.71(0.34-1.46) | 0.542(0.225-1.30) | 0.171 |
| 2351-3550 | 9 | 9 | 0.84(0.32-2.21) | 0.384(0.126-1.174) | 0.093 |
| ≥3551 | 20 | 6 | 0.25(0.01-0.65) | 0.275(0.098-0.773) | 0.014* |
| Physical exercise | |||||
| No | 179 | 157 | 1 | 1 | |
| Yes | 13 | 24 | 0.48(0.23-0.97) | 0.54(0.235-1.233) | 0.143 |
| Substance use | |||||
| Yes | 47 | 27 | 1 | 1 | |
| No | 145 | 154 | 0.54(0.32-0.91) | 0.454(0.253-0.817) | 0.008* |
| Fruit &vegetable diet | |||||
| No | 69 | 47 | 1 | 1 | |
| Yes | 123 | 134 | 0.63(0.4-0.98) | 0.687(0.409-1.153) | 0.155 |
Table 9: Multivariate analysis of factors associated with adverse effect, DMRH, EGZ, ANRS, Ethiopia, 2013.
Multivariable analysis
Educational status, literacy, Income and substance use remain significant at multivariate analysis. The odds of adverse effect were 0.477 times less likely among those who were literate in educational status than those who were illiterate [AOR=0.477, 95%CI=0.28-0.812]. Those attained a literacy level of preparatory school were 0.56 times less likely at risk of developing ART adverse effect compared to those who attained only reading and writing level of a literacy skills [AOR=0.56, 95%CI=0.443-0.953]. The odds of ART adverse effect were 0.275 times less likely among those who had a monthly income of 3551 ETB and above compared to those who had no a regular monthly income [AOR=0.275, 95%CI=0.098-0.773]. The odds of ART adverse effects were 0.45 times less likely among those who had no abused substances (cigarette, alcohol and khat) compared to those who had abused substance [AOR=0.454,95%CI=0.253-0.817].
This Study was aimed at determining the prevalence of Anti retroviral Drug Reactions (ADRs) and associated risk factors among patients on Highly Active Anti Retroviral Drugs (HAART). About 373 Adult HIV/AIDS patients on active follow up of HAART were studied for having ADR in Debre Markos Referral Hospital.
In this study, the prevalence of ADR was 51.44% (n=192), which was much higher than prevalence findings of other African countries. In Cameron, of 339 PLWHS on HAART by the year 2013, the prevalence of ADRs was 19.55%, in Indian of 400 PLWHs on HAART studied in 2010, it was 17.55% [11,16,22].
Regarding the type of HAART regimen, in this study about 98% of the HAART regimen was first line, which is in line with other African countries like Cameron (95%). The commonly used HAART regimens include combinations of either of Nevirapian (NVP), Lamivudine (3TC), Enfavirenz (EFV), Zidovudin (AZT) and Tenofovir (TDF). More than half (50.35%, n=94) of this study participants were on a HAART combination of AZT-3TC-NVP and nearly one-fourth (24.95%, n=47) were on ATZ-3TC-EFV.
In this study around 26.04% of respondents reported at least one ADR were patients taking regimens containing first line of AZT-3TC and NVP and the most common ADR was Lipoathrophy (37.50%) followed by peripheral neuropathy (23.96%). This finding was relatively higher than the study findings of other African setting like Cameron (21.2%), urban Kenya (20.7%), rural Uganda (17.2%) and urban and rural Botswana (35%). This discrepancy might be explained for possible variations of the study settings and time gap in which the studies were conducted.
The prevalence of lipoathrophy in this study was 37.5%. The study finding was low when compared to a finding in Botswana (16%). However, it was similar with a finding in Rwanda (34.2%). The occurrence of Lipoathrophy was high with the regimen of ATZ, 3TC, and NVP in both sex, which was 37.55% [22-24].
Anemia has highly associated with the regimen of ATZ, in this study the prevalence was 14.06% but in other related African countries such as Cameron in 2005, ATZ related severe anemia accounted for 28% of all ADRs, in Ivory cost 3.4%, and in Malawian and Senegal studies in the year 2007 indicated AZT-related Anemia of 7.8% and 6.3%, respectively [12,22].
The prevalence of ART related skin rash in this study was 13.2% in contrast, a prospective study in Thailand reported rash in 34% of PLWHs on Nevirapian. The finding of this study was similar to findings in African countries. In the studies of rural Uganda and Kenya it was 6% and 3.7% respectively [6,23].
Hepathotoxicity was highly associated with NVP. The prevalence of Hepathotoxicity in this study was 0.52%. It was in line compared with study findings in Uganda and Kenya reported as 0.5% and 0% respectively [23].
Sex, age and marital status were not statistically significantly associated with ADR. Similarly, CD4 count before and after ART initiation as well as physical exercise had no any statistical significant association with ART adverse effects.
Concerning socioeconomic status, majority of the study participants were in low status, with a monthly income of less and 650 Ethiopian Birr. It was found statistically significantly associated with Adverse Effects of ART. In this study those with income above 3551Birr/month were at less risk of ADR compared to those who had no a regular monthly income.
With regard to the level of education, 57.9% (n=216) patients were literate and 42.10% (n=157) were illiterate these finding was more or less similar to a study finding of Josh et al. [24], However it was much lower than a study finding of India , where level of literacy was 77.5% [13]. Participants with educational status of preparatory school level were at less risk of ARD compared to those who attained a primary school level of education. It may be inferred that higher educational level offered some protection of ADR due to proper understanding of ARV adherence. Generally variables like educational status and income were significantly associated with the ADR.
To some extent the magnitude of Adverse Drug Reaction in this study was high compared to different countries. This might be due to different reason like poor knowledge about drug adherence and inadequate income. The majority of the respondents’ monthly income was insufficient for getting proper nutrition In case of this condition the patient cannot resist the effects of ART toxicity and may synergize the adverse effect of ART.
The prevalence of ART adverse effect in Debre Markos referral Hospital was high compared to other settings with the leading adverse effect of Lipoathrophy. Factors such as educational status, literacy, Income were identified to be independent determinants of ART adverse effect. To reduce the prevalence of ADR in the study area it was recommended to increase the level of education among the target population about HAART adherence, the government should create job opportunities that helps to enhance the level of income in support of their life and modification of feeding habit like consumption of fruits and vegetable. Federal Ministry of Health and Regional Health office in collaboration with Drug Administration and Control Authority and other stakeholders need to support further studies on ADRs. In addition, health care providers should be trained and updated on appropriate selection of ART, early identification of ART side effects, timely substitution of offending drugs and management ART short term and long term adverse effects.
We would like to thank and appreciate the Debre Markos University Public health department for its unreserved assistance, follow up and guidance throughout this work. Our appreciation should also further go to all volunteers who assisted us in gathering all the necessary information to do this study, especially Debre Markos Referral Hospital. We also Thank GAMBY college of health science and Amhara Regional Health Bureau for their assistance with provision of the required resources and supplies in this project.