Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2015) Volume 4, Issue 1
Background: Adult megacolon comprises a heterogeneous group of conditions. This study is a retrospective review of a series of adult megacolon aimed to discriminate a subpopulation of this condition by elucidating shared physiopathology.
Methods: Eight adult megacolon patients without Hirschsprung’s disease were treated over 15 years. Their clinical characteristics were evaluated with an epmphasis on manometric studies.
Results: There were three females and five males aged 60.9 years on average. Seven of the eight patients had central nervous system disorders including epilepsy (4), Parkinson’s syndrome (2) and others (5). Three patients had hemorrhoids. All of these eight patients suffered from chronic constipation, and six of them had a history of sigmoid volvulus. Manometric study revealed anal Ultra Slow Waves, a manometric finding representing hyper-active internal anal sphincter, in five patients.
Conclusion: Anal ultraslow waves and central nervous disorders were highly prevalent in adult megacolon. Hyperactive internal anal sphincter may be responsible for long standing constipation. Persisting hyperactivity of the internal anal sphincter after surgical treatment is a possible explanation for the recurrence of sigmoid volvulus or megacolon in these patients. More attention should be paid for the physiopathology of the anorectum in adult megacolon.
<Keywords: Megacolon; Ultra slow wave; Constipation; Epilepsy; Parkinson’s syndrome
Adult megacolon is an unusual clinical condition seen in middleaged to elderly populations. There have been reported several series of megacolon in the literature since 1950s; however, the clinical details such as physiopathology, natural course and appropriate therapy is yet to be investigated. The authors experienced eight patients of adult megacolon, and all of them were evaluated on their anorectal functions using manometry. Out of the eight patients, we found seven patients accompanying central nervous system disorders and five patients with hyperactive internal anal sphincter. These observations lead us to hypothesize that altered colonic motility and hyperactive, namely functionally stenotic, anal canal may cause long-standing severe constipation and megacolon in some population. High prevalence of anal Ultra Slow Waves (USWs), a manometric finding representing hyper-active internal anal sphincter, in the patients with adult megacolon suggests the presence of a subpopulation sharing the same physiopathology. The clinical characteristics of these eight patients were presented with a review of literatures.
A retrospective review was undertaken of all patients underwent anorectal manometric studies on adult megacolon over a 15 year period. The manometric recordings were obtained at Akita University Hospital and Fujiwara Memorial Hospital during the period from 1995 to 2009. All the recordings were of good quality, which allowed us to make a correct judgment regarding the presence or absence of anal Ultra Slow Waves. Presence of ganglion cells and absence of prominent nerve fibers in the lamina propria and muscularis mucosa were histologically confirmed respectively by hematoxylin and eosin staining and acetylcholineesterase activity staining to rule out Hirschsprung’s disease. Presence of recto-anal reflex was also confirmed by manometric study.
Manometric study
After emptying the rectum by glycerine enema, patients lay with the left side down. One pressure-monitor-probe was positioned in the rectum and another in the anal canal. The transducers (DTS DX-360, Nihon Kohden Co., Japan or CTU/P-1, Gaeltec Co, Scotland) were connected via an amplifier (AD100F, Tokyo, Nihon Kohden Co., Japan) to a chart recorder (RTA-1100M, Nihon Kohden Co.,Tokyo, Japan). Anal resting pressure was measured using the pull-through method. Then, the probe was positioned at the point of maximal pressure in the anal canal to know the presence (or absence) of USWs and recto-anal inhibitory reflex elicited by balloon inflation in the rectum.
Fecoflowmetry
Normal saline (0.9% NaCl solution) was infused in the rectum at a rate of 100 ml/minutes by open infusion until the patient began to feel an urge to defecate. If the patient felt no urge by 500ml of saline infusion, the infusion was stopped at 500ml. Then, the patient was instructed to sit on the commode equipped with a flow meter (SAKURA UROFLO-MET SUF-200, Sakura Co.,Tokyo, Japan) to evacuate the saline in the same manner as usual defecation. Saline evacuation curve was recorded. In addition to the shape of evacuation curve, maximum flow rate (ml/sec) and total evacuation time (sec) were automatically calculated [1].
Criteria for ultra slow waves
Since there were no fixed criteria for USWs besides their low frequency (usually <2 min-1), we proposed criteria for USWs as follows [2,3]:
1. Rhythmical pressure fluctuations with a frequency less than 2 minutes
2. Amplitude greater than 25 cm H2O
3. Lack of synchronicity with rectal contractions
4. Lack of complete disappearance of anal slow waves at the nadir of the wave
5. By using these criteria, we can exclude a series of repeated recto-anal inhibitory reflex.
Ethical aspects
The patients need to be well-informed about the study. The procedures of the anorectal function test were done after obtaining informed consent from the patients. This study was approved by the Ethics Committee of Akita University School of Medicine (Approval No 334).
Patient characteristics
There were eight patients with idiopathic megacolon studied on their anorectal functions using manometry. There were three females and five males aged 60.9 years on average (range 25 to 84 years). Hirschsprung’s disease was ruled out. Ogilvie syndrome, acute colonic pseudo obstruction, was also ruled out because of the slow onset in our series. Seven of the eight patients had central nervous system disorders including epilepsy (3), Binswanger’s disease (1), Parkinson’s syndrome (2), Bourneville-Pringle disease (1), brain tumor (1), alcoholism (1) and left hemiplegia due to cerebral infarction (1). All of the eight patients suffered from chronic constipation, and six of them underwent surgery for accompanied sigmoid volvulus.
Anorectal function tests
Five patients were proved to have USWs in the anal canal (Figure 1). Furthermore, hemorrhoids were found in three patients (Table 1). Fecoflowmetic curve was recorded in five patients to evaluate actual state of defecation. All of these patients needed excessive straining at excretion of the rectal content. And, as a result, the fecoflowmetric curves were segmental in shape with long excretion time and low flow rate in three patients (Figure 2). Other two patients with massive type fecoflowmetric curves were both young men. None of the patients expressed urge to defecate even after 500ml of saline was infused in the rectum. The anal resting pressure of the patients with USWs was significantly higher than that of the patients without USWs (116.6 ± 40.0 vs. 40.0 ± 26.5 cm H2O).
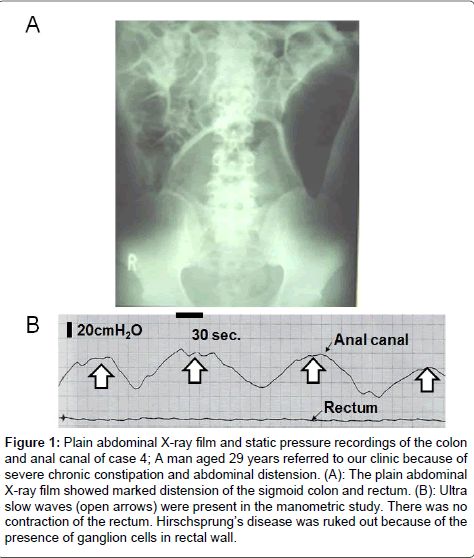
Figure 1: Plain abdominal X-ray film and static pressure recordings of the colon and anal canal of case 4; A man aged 29 years referred to our clinic because of severe chronic constipation and abdominal distension. (A): The plain abdominal X-ray film showed marked distension of the sigmoid colon and rectum. (B): Ultra slow waves (open arrows) were present in the manometric study. There was no contraction of the rectum. Hirschsprung’s disease was ruked out because of the presence of ganglion cells in rectal wall.
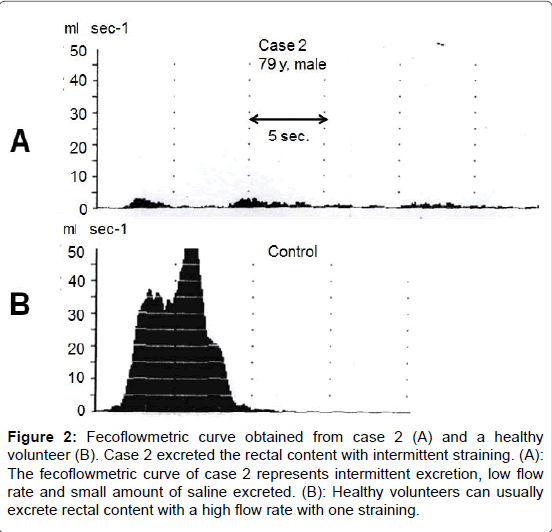
Figure 2: Fecoflowmetric curve obtained from case 2 (A) and a healthy volunteer (B). Case 2 excreted the rectal content with intermittent straining. (A): The fecoflowmetric curve of case 2 represents intermittent excretion, low flow rate and small amount of saline excreted. (B): Healthy volunteers can usually excrete rectal content with a high flow rate with one straining.
| Case | Age (yr) | Sex | Clinical Diagnosis | Accompanying disease | Anorectal function tests | Treatment | Prognosis | Follow-up period | ||||
| USW | Maximal anal resting pressure (cmH2O) | SET | FFM | |||||||||
| Flow rate | Evacuation curve | |||||||||||
| 1 | 74 | F | Sigmoid volvulus, | Binswanger's disease | P | 183 | ND | ND | ND | Sigmoidectomy and Sigmoid Colostomy | Bowel movements via colostomy without marked abdominal distension | 2years |
| Megacolon, | Hemorrhoids | |||||||||||
| Chronic constipation | ||||||||||||
| 2 | 79 | M | Sigmoid volvulus, | Parkinson syndrome, | P | 80 | No urge to defecate | 2.9ml sec-1 | Segmental type | Sigmoidectomy | Constipation | 3 years |
| Megacolon, | Bowen's disease (rt. leg) | Weakened rectal contraction | Laxatives | Recurrence of sigmoid volvulus | ||||||||
| Chronic constipation | ||||||||||||
| 3 | 46 | M | Megacolon, | Parkinson syndrome, | P | 120 | No urge to defecate | 2ml sec-1 | Segmental type | Glycerine Enema | Constipation | 15years |
| Chronic constipation | Alcoholism, | Weakened rectal contraction | Insertion of rectal tube for decomplession | Marked abdominal distension | ||||||||
| Epilepsy | ||||||||||||
| 4 | 29 | M | Megacolon, | None | P | 100 | No urge to defecate | > 50ml sec-1 | Massive type | Sigmoidectomy | Upper abdominal distension | 1 month |
| Chronic constipation | Incontinence for waterly rectal content | No constipation | ||||||||||
| 5 | 25 | M | Sigmoid volvulus, | Bourneville-Pringle disease, | A | 20 | ND | > 50ml sec-1 | Massive type | Sigmoidectomy | No recurrence of sigmoid volvulus | 5 years |
| Megacolon, | Brain tumor, | No constipation | ||||||||||
| Chronic constipation | Epilepsy | Abdominal distension | ||||||||||
| 6 | 70 | M | Sigmoid volvulus, | Cerebral infarction, | P | 100 | No urge to defecate | ND | ND | Sigmoidectomy | Colostomy was made because of the recurrence of sigmoid volvulus | 5 years |
| Megacolon, | Hemorrhoids | |||||||||||
| Chronic constipation | ||||||||||||
| 7 | 84 | M | Sigmoid volvulus, | Epilepsy, | A | 30 | ND | ND | ND | Sigmoidectomy | No recurrence of sigmoid volvulus | 1 year |
| Megacolon, | Hemorrhoids | No constipation | ||||||||||
| Chronic constipation | Abdominal distension | |||||||||||
| 8 | 80 | F | Megacolon, | Epilepsy, | A | 70 | ND | ND | ND | Sigmoidectomy and Sigmoid Colostomy | Bowel movements via colostomy without marked abdominal distension | 2 years |
| Chronic constipation | Rheumatoid arthritis, | |||||||||||
| Note: yr: Year; F: Female; M: Male; P: Present; A: Absent | ||||||||||||
Table 1: Details of hemorrhoids found in three patients.
Treatments
Case 3, a 46 year-old male with alcoholism, was treated conservatively with glycerine enema, laxatives, manual extraction and insertion of rectal tube for gas bloating on demand, and remained stable without much improvement in his bowel symptoms. He developed recurrent attack of consciousness loss, and was diagnosed as epilepsy five years after the evaluation of megacolon. Seven patients underwent sigmoidectomy. Case 1 and 8 underwent sigmoidectomy and colostomy simultaneously in the first surgical treatment because of their impaired physical activity. Case 2 and 6 had recurrent episodes of sigmoid volvulus, and colostomy was made in case 6. Case 3, 4 and 7 had no episode of recurrent sigmoid volvulus, but had persisting or re-emerging abdominal distension after surgery. Laxatives and glycerin enema were used as needed in combination with Daikenchuto, a traditional herbal medicine. Topical use of nitrogen oxide containing cream might be a choice of treatment for hyperactive internal anal sphincter. But nitrogen oxide containing cream could not be used, since it was not approved as a therapeutic medication in Japan.
Histological findings of resected colon
The dilated sigmoid colon was resected in seven patients. Pathological examination of operative specimens showed hypertrophy of the colonic wall. No specific findings were pointed out about intestinal nervous system except case 1 who exhibited hyperplasia of Auerbach’s plexus. The ganglion cells were present in all cases and no degenerative change was observed.
Adult megacolon is a rare clinical condition characterized by longstanding defecatory problems, marked abdominal distension and air-filled dilated colon on abdominal X-ray film. Adult megacolon can be differentiated from Hirschsprung’s disease by the presence of rectoanal inhibitory reflex and ganglion cells in myenteric plexus. After Hirscsprung’s disease is ruled out, adult megacolon accompanying severe clinical symptoms is often treated with colectomy. Since the physiopathology of adult megacolon is thoroughly understood, the outcome of surgical treatment is uncertain. As suggested in our series, surgical treatment without thorough understanding of the physiopathology of functional colonic diseases may result in unsatisfactory outcome. Subpopulations with different physiopathology may be included in the patients with adult megacolon. Predisposing risk factors for adult megacolon are chronic constipation, neuropsychiatric diseases including Parkinson’s syndrome [4-6], diabetes [6] and elderly people [7]. In a case of Parkinson’s disease, Lewy bodies were recognized in the ganglion cells in the resected intestine [8]. There are only a few studies on the anorectal manometric anomalies found in central nervous disorders. Weber et al. [9] reported hypertonia in the anal canal in two of the seven patients with frontal lobe brain damage. There is no epidemiological data on the comorbidity of anal hypertonia with USWs and central nervous disease. The physiopathology of colonic motility disorders is complicated. Not only disturbance of intrinsic intestinal nervous system but also extrinsic autonomic nervous system may cause intestinal dysmotility. In fact, acute colonic pseudo obstruction caused by herpes zoster invading celiac plexus has been reported [10]. In our series, seven of the eight patients had disorders of central nervous system including three cases of epilepsy. Constipation is a common side effect of phenytoin, anti-convulsants widely prescribed for patients with epilepsy; however, case five had megacolon and USWs more than five years before the diagnosis of epilepsy was made and treatment with phenytoin was started. In addition, possible role of the functional alterations in intestinal smooth muscle cells and connective tissue elements in idiopathic megacolon were also reported in some studies [11-13]. The physiopathological mechanism connecting central nervous system disorders and megacolon is yet to be elucidated. Presence of recto-anal inhibitory reflex, diminished sensitivity for rectal distension and delayed colonic transit time are usual findings in intestinal function tests of megacolon. USWs have been described in several clinical conditions such as haemorrhoids [13,14] and anal fissures [14,15]. In our previous studies on manometric findings, hemorrhoids, anal fissure and megacolon were risk factors for USWs [1,2]. Hemorrhoids and anal fissure is directly diagnosed by inspection; however, anorectal manometry may be performed in very limited cases. In this study, we showed a high prevalence rate of USW in patients with adult megacolon with an Odds ratio of 30.8 (95% confidence interval: 5.4-177.4) when compared with the prevalence rate of USW among people without problems in their bowel movements [16-18]. The high prevalence of USWs in our series would have an important clinical relevance to the treatment for adult megacolon. So far, special treatments such as internal anal sphincterotomy [19] and topical use of cream or suppository containing nitrogen oxide [20,21] for hyperactive internal anal sphincter have not been applied in our series. Thus, hyperactive internal anal sphincter left after the treatments might be responsible for the persisting symptoms after the treatments in our series. In the cases of adult megacolon exhibiting UWSs, not only the resection of dilated bowel but also the treatments for a hyperactive internal anal sphincter may be required to improve the clinical outcome; however, nitrogen oxide containing cream has not been approved as a therapeutic medication for the anal sphincter hyperactivity in Japan. Application of a stereotyped surgical procedure to all the cases of adult megacolon would result in unsatisfactory results in some populations with heterogeneous physiopathology [22]. For elucidating a subpopulation in adult megacolon and their proper management, a prospective cohort study is required; however, it will require accumulation of the cases and much time. Further investigations are needed for thorough understanding of adult megacolon.
This research was funded through The Mitsubishi foundation.