Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2014) Volume 4, Issue 2
Objective: Because of the wide-spread use of menaquinone-7 (MK-7, a form of vitamin K2) supplements, we have investigated its pharmacokinetics following a single intake from various formulations.
Methods: Different formulations were compared in four human intervention studies with healthy volunteers. Participants received either capsules (filling material: linseed oil; MK-7 carrier material: sunflower oil) or tablets (filling material: dicalcium phosphate dehydrate (DCPD) and cellulose; MK-7 carriers: casein, Arabic gum, or sunflower oil). MK-7-absorption profiles (24 h area-under-the-curves, 24 h AUCs) were used to compare intestinal absorption. Special attention was given to intra- and inter-subject variability.
Results: The absorption (time-to-peak) of MK-7 from tablets was slower than from capsules, 6 h as compared to 2 h-4 h, respectively. Probably, the oily matrix of the capsules released the lipophilic MK-7 more rapidly than the powder matrix of the tablets. We further found a dose response relationship for MK-7 at 24 h after the single-dose intakes (at group level). As compared to baseline, circulating MK-7 levels were still elevated at 24 h after intake, confirming the relatively long half-life of MK-7. The different MK-7 carrier materials showed similar 24 h-absorption profiles, indicating that the carrier was not influencing MK-7 absorption. Next to high intra-subject variability, high inter-subject variability
was seen in the different studies. This was found for both, peak height and for total absorption (measured as 24 h-AUC). While some subjects showed a linear dose-response relation, other subjects had similar 24 h-AUCs after intake of MK-7 at different dosages
Conclusions: We have demonstrated that on a group level the bioavailability (24 h absorption) of MK-7 was similar for capsules and tablets, and also for the different MK-7 carriers. MK-7 absorption from the various formulations showed high intra- and inter-individual differences.
Keywords: Absorption; Bioavailability; Capsules; Menaquinone-7; Tablets; Vitamin K2
Vitamin K functions as a cofactor for the γ-glutamate carboxylation of proteins involved in blood coagulation (factors II, VII, IX, X), calcium and bone metabolism (osteocalcin), cell growth regulation (Gas6), as well as soft tissue calcification (matrix Gla-protein) [1]. The carboxylated glutamate residues are called Gla-residues, and the proteins in which these unusual amino acids occur are generally referred to as the Gla-protein family. The Gla-residues in these proteins form strong calcium-binding groups that are required for their biological function. Hence, vitamin K plays a key role in important metabolic processes.
The two forms of vitamin K present in the human diet are phylloquinone (also known as vitamin K1) and the group of menaquinones (collectively known as vitamin K2). The nomenclature of the menaquinones is MK-n, where n stands for the number of unsaturated isoprenoid residues in the aliphatic side chain. Dietary relevant short-chain menaquinones are MK-4 through MK-6, of which MK-4 is by far the most abundant one; long-chain menaquinones are MK-7 through MK-10, of which MK-7 is the most prominent in the Japanese diet and MK-8 and MK-9 in the Western diet. Following intake, circulating vitamin K levels rapidly increase to reach their peak value between 2 h and 6 h postprandially, followed by a rapid decline for phylloquinone and MK-4, whereas the long-chain menaquinones were reported to have more complex pharmacokinetics and disappear much slower from the circulation [2-4]. Differences in pharmacokinetics of the various K-vitamers are probably related to differences in their molecular structure and to a number of unknown factors, including the food matrix, nature and amount of macronutrients, activity of digestive enzymes, transport efficiency across the intestinal cell, and bile production, and other individual conditions [5].
Several population-based studies have reported specific health effects of the long-chain menaquinones, notably MK-7, MK-8 and MK-9 [6-10]. Because of the wide-spread use of MK-7-containing supplements, we were interested to investigate in more detail pharmacokinetics of MK-7 following a single intake from various formulations. We compared different formulations: capsules and tablets, and different MK-7 carrier materials in four independent human intervention studies with healthy volunteers. Circulating MK-7 profiles covering 24 h after a single intake were used to compare intestinal absorption, and special attention was given to intra- and inter-subject variability.
Study 1
In this double-blind, randomized, cross-over study, absorption of MK-7 (MenaQ7, Nattopharma, Norway; daily dose of 75 μg) from tablets of two different raw material suppliers was studied. These tablets contained the inert filling material dicalcium phosphate dehydrate (DCPD) and microcrystalline cellulose and MK-7 in three different carrier materials i.e. sunflower oil (supplier 1), soybean oil (supplier 2), or maltodextrin (supplier 2) (Table 1). These three types of tablets were compared in a cross over design. Healthy men and women, aged between 20 and 40 years, were recruited in November 2010 in the southern region of the province of Limburg through placing an advertisement. Exclusion criteria were: BMI <18.5 kg/ m2 and >30 kg/m2, metabolic or gastrointestinal diseases, chronic degenerative or inflammatory diseases, anemia, pregnancy, diabetes mellitus, soy allergy, abuse of drugs/alcohol, use of corticosteroids, oral anticoagulants, salicylates, antibiotics, and use of vitamin K supplements. Twenty-four participants (12 male / 12 female) who met the inclusion criteria were randomized to receive the first MK-7 tablet (a single dose of 75 μg MK-7). After a 2-week wash-out period, participants switched to the second type of tablet, and after another 2-week wash-out period they received the third type of tablet. On the first intervention day, blood was sampled after an overnight fast (t=0 h). Immediately after sampling, participants received a standardized breakfast (two rolls or toast with 20 g of butter, jam, 150 mL of demiskimmed milk and tea) together with the MK-7 tablet. Subsequently, blood was sampled at 2 h, 4 h, 6 h, 8 h and 24h after the single intake of MK-7. At t=4 h a standardized lunch was offered consisting of 2 rolls and toast with butter, meat and/or jam, 250 g of demi-skimmed yogurt and coffee or tea. Two weeks before the start of the study and during the study, subjects were asked to refrain from consuming foods rich in phylloquinone (spinach, green kale, broccoli, Brussels sprouts) and rich in menaquinones (curd, cheese, natto).
| Study 1 (n=24) | Study 2 (n=69) | Study 3 (n=16) | Study 4 (n=12) | |||||
|---|---|---|---|---|---|---|---|---|
| Trial reg. nr. | NCT01638143 | NCT00858767 | NCT00742768 | No | ||||
| Design | Double-blinded, randomized, cross-over | Double-blinded, randomized, parallel | Double-blinded, randomized, cross-over | Open, randomized, cross-over | ||||
| Study products | Tablets | Tablets | Tablets | Tablets | Capsules | GelpellTM caps | Capsules | Food |
| Number/amount | 1 | 2 | 2 | 3 | 4 | 4 | 4 | 40g |
| Daily dose | 75 μg | 90 μg | 90 μg | 90 μg | 180 μg | 180 μg | 360 μg | 360 μg |
| MK-7 carrier material | Sunflower oil, soybean oil or maltodextrin | Casein, Arabic gum or sunflower oil | Sunflower oil | Sunflower oil or natto food | ||||
| Filling material of supplements | Microcrystalline cellulose, DCPD | DCPD, microcrystalline cellulose | Linseed oil | Confidential | Linseed oil | |||
| Time of intake | With breakfast | With breakfast | With breakfast | With breakfast | ||||
| Standardized breakfast / lunch | Yes | Yes | Yes | Only breakfast | ||||
| Sampling times | 0h, 2h, 4h, 6h, 8h, 24h | 0h, 2h, 4h, 6h, 8h, 24h | 0h, 2h, 4h, 6h, 8h, 24h | 0h, 2h, 4h, 6h, 8h, 24h | ||||
| Vitamin K-rich food restriction | Yes | Yes | Yes | Yes | ||||
Table 1: Study design of four randomized clinical trials on MK-7 absorption.
Study 2
In this double-blind, randomized, parallel study, we compared absorption of MK-7 (MenaQ7, Nattopharma, Norway; daily dose of 90 μg) from tablets (filling material: DCPD and microcrystalline cellulose) containing three different MK-7 carriers, namely casein, Arabic gum, and sunflower oil (Table 1). Healthy men (n=28) and women (n=41), aged between 20 and 40 years, were recruited in October 2008 in the southern region of Limburg through placing small advertisements. Exclusion criteria were BMI >30 kg/m2, metabolic or gastrointestinal diseases, chronic degenerative or inflammatory diseases, anemia, soy allergy, abuse of drugs/alcohol, use of corticosteroids, oral anticoagulants, use of vitamin K supplements, and high dietary intake of vitamin K. Eligible participants were randomly divided to consume daily either two casein tablets, two Arabic gum tablets, or three sunflower oil tablets during 8 weeks. After an overnight fast and a first blood sample (t=0 h), the participants took the MK-7 tablets together with a standardized breakfast, followed by a standardized lunch at t=4 h (as detailed for Study 1). The subsequent samples were taken at 2 h, 4 h, 6 h, 8 h and 24 h. One week before the start of the study and during the study, participants were asked to refrain from consuming foods rich in vitamin K. This study has been shortly mentioned in the recently published paper “Vitamin K status in healthy individuals” [11]. However, different data were presented, namely the MK-7-induced changes in circulating desphopho-uncarboxylated matrix Gla-protein (marker for vitamin K status) in relation to baseline.
Study 3
Newly developed MK-7 (MenaQ7, Nattopharma, Norway) capsules with sunflower oil (GelpellTM, matrix pellets from gelatin, Gelpell AG, Swiss Caps AG, Switzerland) were compared to conventional gelatin soft gel capsules with sunflower oil and MK-7 (MenaQ7, Nattopharma, Norway) in a double-blind, randomized, cross-over study (Table 1). The difference between both capsules was that the MK-7 in the GelpellTM capsules was encapsulated in microspheres, a technique known to give more complete absorption. Healthy men (n=8) and women (n=8), aged between 20 and 30 years, were recruited June 2008 in the southern region of Limburg through placing small advertisements. Exclusion criteria were: BMI >30 kg/m2, metabolic or gastrointestinal diseases, chronic degenerative or inflammatory diseases, anemia, soy allergy, use of corticosteroids, oral anticoagulants, and use of vitamin K supplements. Eligible participants were randomized to receive a single dose of 180 μg MK-7 (four soft gel or four GelpellTM capsules; 45 μg MK-7 per capsule). Every two weeks, participants switched to another treatment. The capsules were consumed together with the standardized breakfast followed by lunch as defined for Study 1. Blood sampling of the participants took place before (0 h, after an overnight fast) and after the intake of the capsules at 2 h, 4 h, 6 h, 8 h and 24 h. The week before intake of the capsules and during the study participants were asked to refrain from consuming foods rich in vitamin K. During the wash-out period, subjects were allowed to consume their normal diets, but not to consume more than normal amounts of green vegetables (200 g/day of spinach, broccoli, etc.) and (curd) cheese (< 50 g/day), and no natto.
Study 4
This study had an open, randomized, crossover design (Table 1). Healthy men (n=6) and women (n=6), aged between 20 and 30 years, were recruited among students of Maastricht University in January 2008. Exclusion criteria were: BMI >30 kg/m2, metabolic or gastrointestinal diseases, chronic degenerative or inflammatory diseases, use of corticosteroids, oral anticoagulants, and vitamin K supplements. Eligible volunteers were randomized in two groups to receive a single dose of either 40 g homogenized natto (360 μg of MK- 7) or four MK-7 (MenaQ7, Nattopharma, Norway) capsules (90 μg MK-7 per capsule with sunflower oil) at breakfast (as defined for Study 1). Subsequently, blood samples were taken at 0 h, 2 h, 4 h, 6 h, 8 h and 24 h after intake of the single dose natto or the MK-7 capsules. After a 2-week wash-out period, participants switched to the second treatment. One week before the study and during the study period, subjects were not allowed to consume vitamin K-rich foods; only small amounts of (curd) cheese (<100 g/d) were acceptable during this period.
All studies were conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Medical Ethics Committee of the Maastricht University Medical Center (Maastricht, The Netherlands). Written informed consent was obtained from all subjects before entering the study. Trial registration codes were clinicaltrials.gov: NCT01638143 (study 1), NCT00858767 (study 2), and NCT00742768 (study 3). Study 4 was not registered.
Circulating MK-7 levels
Plasma MK-7 levels (ng/mL) were determined according to standard procedures. In short, samples were extracted with hexane and after pre-purification on silica columns, they were analyzed by high performance liquid chromatography (HPLC) using a C-18 reversed phase column with online zinc reduction and fluorescence detection. Vitamin K1-25 (a synthetic form of vitamin K1 containing 5 isoprenoid residues) was used as an internal standard. Individual AUC values were calculated from the individual MK-7 absorption profiles using the trapezoidal rule. MK-7 measurements were performed at the research laboratory of VitaK BV (ISO9001-certified lab, Maastricht, The Netherlands).
Statistics
To ensure homogeneity of the four studies, we used the following sampling points for statistics: 0 h, 2 h, 4 h, 6 h, 8 h, and 24 h. Within one study, between-group differences in AUC values were analyzed by the non-parametric Mann-Whitney, Kruskal-Wallis, or Wilcoxon- Signed Rank tests. Differences were considered statistically significant at p<0.05 (SPSS 19). Inter-study and intra-subjects comparisons regarding MK-7 absorption were done by comparison of the timeto- peak, peak heights, and AUC-values. Finally, we identified three subjects that participated in studies 1, 2, and 3, and we could therefore perform the intra-subject comparisons.
Inter-study comparisons regarding MK-7 absorption
Based on the change from baseline of the biomarkers (UACR, plasma BNP) and their percent change, the profile will be compared between the treatment groups and reviewed by repeated-measure analysis of variance with measurement time points as repetition. Primary endpoints will be analyzed by the closed testing procedure in the order of UACR, plasma BNP, and their percent change in consideration of multiplicity.
Study 1
The time-to-peak was 6 h after intake of one tablet of MK-7 (Table 2 and Figure 1A). A first peak was observed after 2 h of intake, with a second peak at 6 h corresponding to a peak height of about 1 ng/ mL for all three formulations. The 24 h AUC values were calculated to range between 13.8 ± 4.3 and 16.1 ± 6.7 ng/mL x h. At 24 h after intake, circulating MK-7 levels were still increased as compared to baseline. Similar patterns were found for all three formulations, and no significant differences were observed between the average absorption curves (time-to-peak and AUC) for each formulation (Figure 1A).
| MK-7 at t0 (ng/mL) | MK-7 at 24h (ng/mL) | Time to peak* (h) | Peak-Height† (ng/mL) | AUC (ng/mL x h) | p# | |
|---|---|---|---|---|---|---|
| Study 1 | ||||||
| Sunflower oil | 0.27 ± 0.15 | 0.49 ± 0.15 | 6 | 0.99 ± 0.38 | 16.08 ± 6.73 | P=0.105 |
| Soybean oil | 0.27 ± 0.18 | 0.48 ± 0.18 | 6 | 0.83 ± 0.37 | 14.33 ± 4.72 | |
| Maltodextrin | 0.30 ± 0.15 | 0.44 ± 0.14 | 6 | 0.86 ± 0.37 | 13.78 ± 4.26 | |
| Study 2 | ||||||
| Casein | 0.27 ± 0.23 | 0.79 ± 0.39 | 6 | 1.63 ± 0.74 | 22.59 ± 8.86 | 0.904 |
| Arabic Gum | 0.31 ± 0.32 | 0.70 ± 0.32 | 6 | 1.94 ± 1.14 | 21.69 ± 8.56 | |
| Linseed oil | 0.23 ± 0.40 | 0.61 ± 0.26 | 6 | 1.64 ± 1.07 | 21.13 ± 8.20 | |
| Study 3 | ||||||
| Sunflower oil | 0.14 ± 0.29 | 1.19 ± 0.58 | 2 | 2.22 ± 0.93 | 37.44 ± 14.73 | 0.049 |
| Sunflower oil (Gelpell) | 0.18 ± 0.41 | 1.43 ± 0.50 | 4 | 3.38 ± 2.37 | 43.34 ± 14.18 | |
| Study 4 | ||||||
| Sunflower oil | 0.13 ± 0.13 | 1.51 ± 0.73 | 4 | 6.77 ± 3.30 | 65.90 ± 28.60 | 0.773 |
| Natto | 0.13 ± 0.12 | 1.94 ± 0.81 | 6 | 5.91 ± 2.75 | 63.03 ± 25.18 | |
| Data are given as mean values ± SD. *Time to the highest peak; †Highest peak; #Between-group difference in AUC as tested by the non-parametric Kruskal-Wallis or Wilcoxon-Signed Rank tests within one study Abbreviations: AUC, area-under-the-curve; MK-7, menaquinone-7; n.s, no significant differences between any arm. | ||||||
Table 2: Absorption measures of MK-7 from single-dose capsules and tablets.
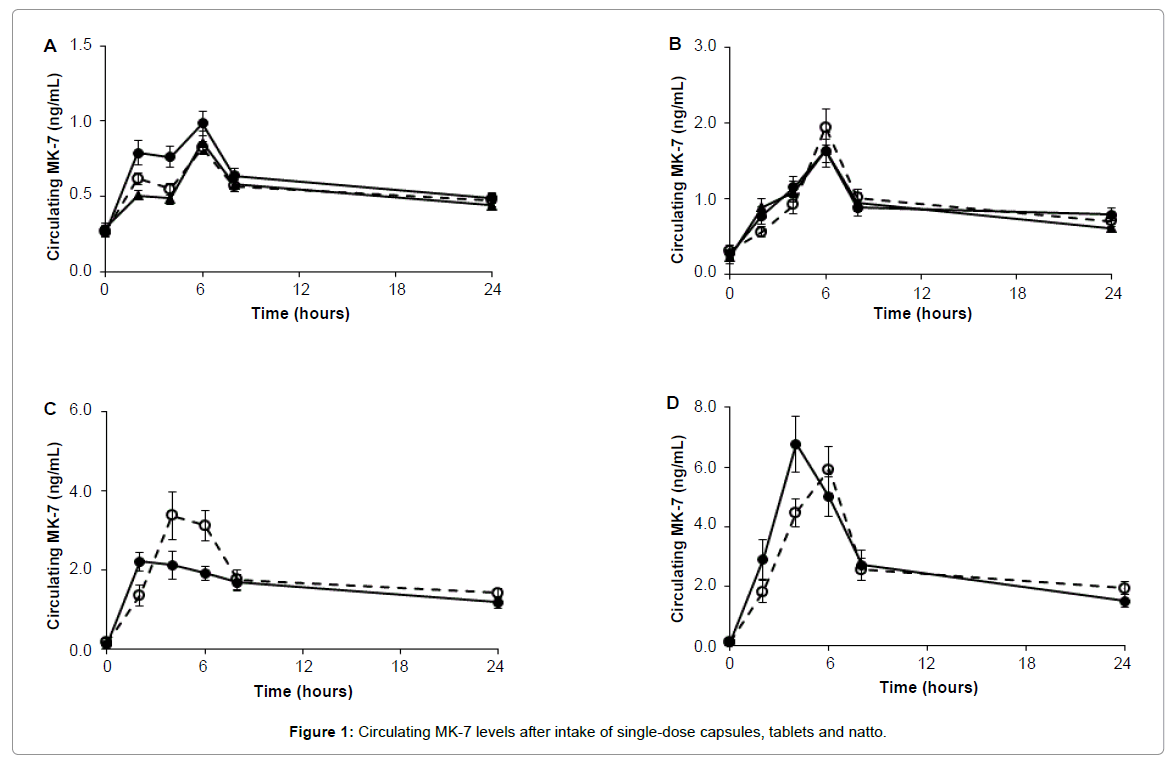
Figure 1: Circulating MK-7 levels after intake of single-dose capsules, tablets and natto.
Study 2
The time-to-peak was 6 h after intake of the MK-7 tablets (Table 2 and Figure 1B), to peak heights of 1.63 ± 0.74 ng/mL, 1.94 ± 1.14 ng/ mL, and 1.64 ± 1.07 ng/mL for the casein, Arabic gum, and linseed oil carriers, respectively. The corresponding 24 h AUCs were calculated to be 23 ± 9 ng/mL x h, 22 ± 9 ng/mL x h, and 21 ± 8 ng/mL x h, respectively. No between-group differences were found with regards to the calculated AUCs. At 24 h after intake, circulating MK-7 levels were still higher than those at baseline for all three groups.
Study 3
The time-to-peak for MK-7 was 2 h and 4 h after intake of the standard soft gel and GelpellTM capsules, respectively (Table 2 and Figure 1C). The corresponding peak heights were 2.22 ± 0.93 ng/mL and 3.38 ± 2.37 ng/mL. The 24 h AUCs were 37 ± 15 ng/mL x h and 43 ± 14 ng/mL x h for the standard soft gel and GelpellTM capsules, respectively. A significant between-group difference was found with regards to the calculated AUCs, showing a better absorption for the patented Gelpell product. At 24 h after intake, circulating MK-7 levels were still higher than those at baseline for both groups.
Study 4
The time-to-peak was 4h after intake of the MK-7 capsules (Table 2 and Figure 1D), corresponding to a peak height of 6.77 ± 3.30 ng/ mL. The 24 h AUC was calculated to be 66 ± 29 ng/mL x h. Again, circulating MK-7 levels were still elevated at 24 h after intake as compared to baseline. It was also clear that MK-7 uptake from natto was slightly slower than from the capsules, with a time-to-peak of 6 h (Figure 1D). Since the AUC values for uptake from natto (63 ± 25 ng/ mL x h) was comparable to that of the capsules, the efficacy of MK-7 was regarded to be similar for both groups.
Inter-study comparisons
As can be seen in Table 2, the tablets gave a slower absorption of MK-7 than the capsules, 6 h as compared to 2 h-4 h, respectively. A dose-response curve was prepared from the average AUC values obtained for all four different dosages (Figure 2). Although the number of data points is only small, curve fitting gave a linear relationship between intake and 24 h-AUC. The fact that the line crosses the Y-axis at 7.4 ng/mL x h is explained by the baseline level of circulating MK-7 found in most participants.
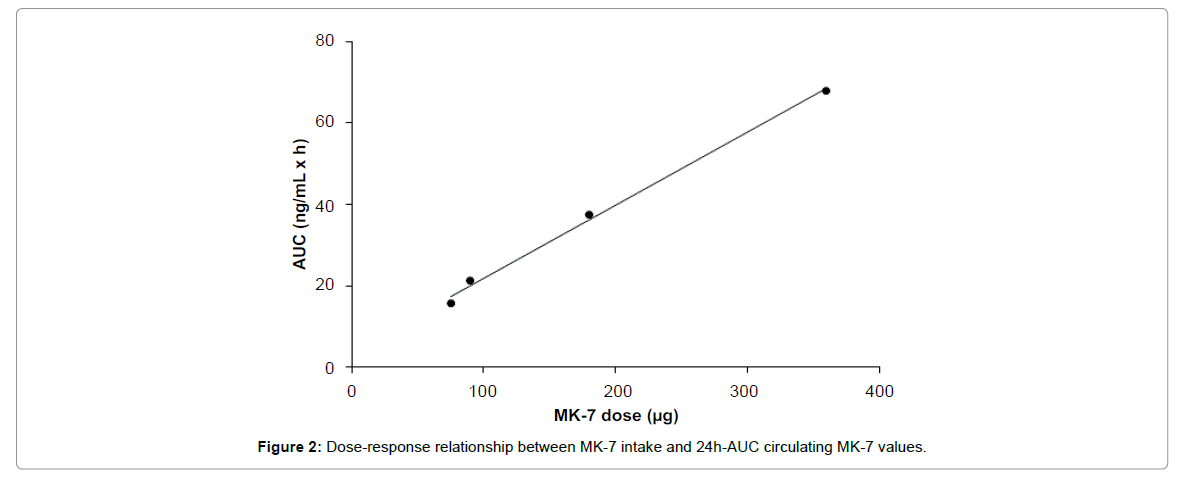
Figure 2: Dose-response relationship between MK-7 intake and 24h-AUC circulating MK-7 values.
Intra- and inter-subject comparisons of MK-7 absorption
There were three individuals who participated in three trials (studies 1-3), and as is shown in Table 3, there were substantial differences in the MK-7 absorption from the 75, 90 and 180 μg formulations. In subject 1 the respective AUC values were 9.9, 24.6 and 39.3 ng/mL x h, and for subject 2 these values were closely similar: 8.9, 22.0 and 31.7 ng/mL x h. For subject 3, however, the dose-response effect was negligible with respective AUC values of 22.4, 29.6 and 28.6 ng/mL x h, respectively.
| Study product | Daily dose (μg) | MK-7 at t0 (ng/mL) | MK-7 at 24h (ng/mL) | Time to peak (h)* | Peak height† (ng/mL) | AUC (ng/mL x h) | |
|---|---|---|---|---|---|---|---|
| Subject 1 | |||||||
| Sunflower oil | Tablets | 75 | 0.34 | 0.42 | 6 | 0.49 | 9.92 |
| Casein | Tablets | 90 | 0.00 | 1.07 | 4 | 2.92 | 24.64 |
| Sunflower oil | Capsules | 180 | 0.00 | 1.53 | 2 | 2.13 | 39.27 |
| Subject 2 | |||||||
| Sunflower oil | Tablets | 75 | 0.00 | 0.40 | 6 | 0.59 | 8.87 |
| Casein | Tablets | 90 | 0.00 | 0.58 | 2 | 1.80 | 22.02 |
| Sunflower oil | Capsules | 180 | 0.00 | 1.11 | 2 | 2.30 | 31.73 |
| Subject 3 | |||||||
| Sunflower oil | Tablets | 75 | 0.37 | 0.45 | 6 | 2.04 | 22.43 |
| Casein | Tablets | 90 | 0.44 | 1.06 | 6 | 2.51 | 29.59 |
| Sunflower oil | Capsules | 180 | 0.13 | 0.77 | 4 | 1.21 | 28.55 |
| Data are given as mean values ± SD. *Time to the highest peak; †Highest peak. Abbreviations: AUC, area-under-the-curve; MK-7, menaquinone-7 | |||||||
Table 3: Absorption measures of MK-7 from single-dose capsules and tablets in 3 healthy volunteers.
Besides the observed intra-subject variability, high inter-subject variability was seen in studies 1, 2, and 3. Some subjects had little absorption, while other subjects had good absorption of MK-7 from the tablets. While some subjects showed a dose-response relation, other subjects had similar absorption after intake of MK-7 at different dosages. Differences were also seen in time-to-peak, peak height, and 24 h AUC
Because of the widespread use of MK-7 containing supplements, it is important to study its pharmacokinetics from different formulations. We therefore measured MK-7 absorption following a single intake from oil-based capsules and powder-based tablets in four intervention trials. Tablets gave a slower absorption of MK-7 (time-to-peak) than capsules, 6 h as compared to 2 h-4 h, respectively. Probably, the oily matrix of the capsules released the lipophilic MK-7 more rapidly than the powder matrix of the tablets. Within the dose range between 75 and 360 μg/day, we found a linear 24 h dose-response relationship for MK-7 after the single-dose intakes; the curve shown in Figure 2 is based on the average AUC values from all four studies, and is only valid for the narrow dose range investigated. Circulating MK-7 levels were still elevated at 24 h after intake as compared to baseline, confirming the relatively long half-life of MK-7 [4].
In study 2, the three different MK-7 carrier materials used in the tablets showed similar absorption profiles, indicating that the carrier material was not influencing 24 h absorption. In study 3, two different encapsulation technologies were compared with regards to MK-7 absorption, i.e. standard soft gel and GelpellTM capsules. A significant between-group difference was found with regard to the calculated 24h-AUCs, demonstrating that the GelpellTM capsules give better absorption of MK-7 than the standard soft gel ones. This confirms the increased bioavailability as reported by the manufacturer (http://www.gelpell.com/EN/download.html). Next to high intra-subject variability, high inter-subject variability was seen in studies 1, 2, and 3. Some subjects had no or poor absorption, while other subjects had good absorption of MK-7 from the tablets. Whereas some subjects showed a linear dose-response relation, other subjects had similar 24 h-AUCs after intake of MK-7 at different dosages. These results further indicate that one subject can have variable absorption on different days, as seen in different studies. Absorption efficiency is influenced by a number of external factors, including the food matrix and effecters of absorption (lipids, dietary fiber, drugs); also individual conditions, like age, sex, and genetic factors are assumed to govern absorption. Although the practical external influences on absorption in the four studies were kept similar as good as possible (i.e. overnight fast, intake with breakfast, standardized meals, restriction on vitamin K-rich foods), these may have affected absorption as well. A limitation to our study is that we evaluated retrospectively four individual trials; ideally, the different formulations need to be compared in one intervention trial.
To our knowledge, only three studies are available on single-dose kinetics of menaquinones after consumption of food supplements [12] or fortified foods [3,4]. Sato et al. [12] showed that MK-7 was well absorbed in Japanese healthy women after single-dose (420 μg MK-7) intake with maximum serum levels at 6 h after intake. In our studies 3 and 4 (using oil-based capsules), the maximum MK-7 peak was seen earlier, i.e. at 2 h-4 h after intake of the capsules. Powder was used in the Japanese gelatin capsules, which may explain the difference in timeto- peak. The maximum peak value in the Japanese participants equaled the maximum peak value after intake of 360 μg MK-7 in study 4 (6.77 ± 3.30 ng/mL). Previously, our group showed that phylloquinone, MK-4, and MK-9 consumed as vitamin K-enriched (2 μmol of each vitamin K form) corn oil gave lower plasma peaks for MK-4 and MK-9 than for phylloquinone [3]. Maximal circulating levels were reached at 2.5, 4, and 5 h postprandially for MK-4, phylloquinone, and MK-9, respectively. Their half-lives differed substantially: whereas phylloquinone and MK-4 disappeared overnight, the estimated half-life for the long-chain MK-9 was about 60 h, which is consistent with the long half-life time of MK-7 reported in the present paper.
In conclusion, we have demonstrated similar MK-7 bioavailability for capsules and tablets, and for the different MK-7 carrier materials used in the tablets. MK-7 absorption from various formulations showed high intra- and inter-individual differences; the mechanism behind it is not yet understood. More research is needed to clarify these differences in bioavailability of MK-7.
CV designed the research; ET analyzed the data, all authors contributed to the writing of the paper.
All authors declare no competing financial interests.