Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2015) Volume 4, Issue 2
Background: Epidemiology of acute poisoning has been extensively studied in agricultural areas of Sri Lanka. It has not been well documented in the other parts of the country. The objective of this study was to describe the pattern of acute poisoning in a Tertiary Care Teaching Hospital in urban Sri Lanka to describe the difference of poisoning patterns in different areas of a country.
Methods: This study was performed as a retrospective study in Colombo South Teaching Hospital (CSTH), Sri Lanka. The bed head tickets (BHTs) of the patients admitted to the medical units of CSTH from 1st January 2009 to 31st December 2009 were retrieved. Patients admitted to pediatric units and with snake bites and food poisoning were excluded.
Results: From 1st of January 2009 to 31st of December 2009, 92668 patients were admitted to CSTH and 1.27% (1178) was admitted following acute poisoning. Of those patients we were able to collect data on 70.46% (828). Male to female ratio was 37:63. The commonest cause of poisoning was due to medicinal drug overdose 63.52% (526) of which paracetamol overdose accounted for 37.6% (311). Organoposphate (OP) accounted for 11.11% (92) of the admissions. Mean duration of hospital stay was 3.49 (SD4.97) days.
Discussion: The pattern of poisoning observed in CSTH is significantly different to the pattern seen in agricultural areas of the country.
<Acute poisoning is a major global public health problem [1]. In industrialized countries, self poisoning predominantly occurs in young people impulsively responding to stressful events with little desire to die. Deaths are rare since the medicines commonly taken are of low toxicity or easily treated [2,3]. In Sri Lanka too the poisonings mainly occur in the economically productive young people as a reaction to stressful events however unlike in industrialized countries the mortality rate recorded is high. This pattern is mainly observed in agricultural areas. In these areas most of the poisonings are due to pesticides mainly organophosphates [4].
Epidemiology of acute self poisoning in Sri Lanka has been extensively studied but most of the studies were done in the agricultural areas of the country. Very few studies have been done in non-agricultural areas of the country thus the pattern of poisoning and the problems encountered in the urban areas of the country may be different to what has been observed. This study aimed to identify the patterns and poisons used in an urban area of Sri Lanka. That would enable us to demonstrate the differences between the poisoning patterns in different areas of a country.
This study was carried out as a retrospective descriptive study at the Colombo South Teaching Hospital, Western Province Sri Lanka. The admission books from 1st of January 2009 to 31st of December 2010 of all medical wards were screened. The BHT numbers of patients admitted with acute poisoning were recorded. The bed head tickets (BHTs) of the patients admitted to the medical units of CSTH from 1st January 2009 to 31st December 2009 following acute poisoning were retrieved from the medical records room of the CSTH. The data were collected in preformed data extraction forms. Patients admitted to pediatric units and with snake bites and food poisoning were exclude.
Data analysis was done using the SPSS (Version 16) and Microsoft Excel 2007 version. Data is presented as descriptive summary statistics. This study was granted ethical clearance by the Ethical Review committee of the Faculty of Medical Sciences and Colombo South Teaching Hospital.
In year 2009 (1st of Jan-31st of Dec) 92668 patients were admitted to the Colombo South Teaching Hospital (CSTH) (Figure 1). One thousand one hundred and seventy eight (1.27%) patients were admitted following acute poisoning to the general medical units of CSTH. We could retrieve 70.28% (828) BHTs from the hospital’s record room while others were missing or were not accessible. There were 519 (60.75%) females and, 309 males. Three hundred and twenty five (39.25%) patients were in the age group of 21 to 30 years (Table 1).
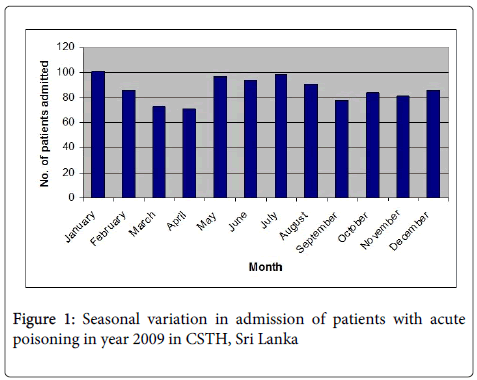
Figure 1: Seasonal variation in admission of patients with acute poisoning in year 2009 in CSTH, Sri Lanka
| Age | Sex | |
|---|---|---|
| Male | Female | |
| 12-20 | 72 | 229 |
| 21-30 | 131 | 194 |
| 31-40 | 51 | 51 |
| 41-50 | 31 | 26 |
| 51-60 | 11 | 8 |
| 61-70 | 11 | 7 |
| >71 | 2 | 4 |
| Total | 309 | 519 |
Table 1: Age and sex distribution of the poisoned patients admitted from 1st of January 2009 to 31st December 2009
Out of the total poisoning admissions 89.73% (743) were direct admissions to the CSTH while 10.27% (85) of patients were transferred from the peripheral hospitals mainly due to non-availability of antidotes. Most of the admissions 63.64% (527) were following ingestion of medicines and 11.11% (92) people ingested OPs. Kerosine oil poisoning was also found to be common accounting for 9.42% (78) of total admissions (Table 2). Medicines were ingested by 527 and of those 58.5% (272) ingested paracetamol, 10.1% (47) ingested antipsychotics, 7.1% (33) ingested chlopheniramine, and 12.5% ingested multiple drugs (Table 3). 78.74% (652) of the patients admitted following acute poisoning were given gastric decontamination following acute resuscitation and stabilization. The most commonly used decontamination methods were gastric lavage 65.2% (540) and administration of activated charcoal: 71.86% (595); Forced emesis 0.48% (4) was rarely used. In most of the cases 74.23% (484) activated charcoal has been administered following gastric lavage. In 6.52% (54) only gastric lavage has been performed and in 16.1% (105) only activated charcoal has been administered. Data on time since ingestion to gastric lavage was available in 407 patients out of 540 patients who received gastric lavage. The mean time since ingestion to gastric lavage was 5.04 (SD 9.78) hours. Only 17.22% (93) of patients were given gastric lavage within 2 hours of ingestion.
| Type of poison | Count | Percentage (%) |
|---|---|---|
| Drug overdose | 527 | 63.64 |
| OP | 92 | 11.11 |
| Domestic & industrial chemicals | 78 | 9.42 |
| Kerosin oil | 26 | 3.14 |
| Carbamates | 6 | 0.72 |
| Glyphosates | 10 | 1.21 |
| Paraquate | 7 | 0.85 |
| Toxic Plants | 5 | 0.60 |
| Others | 19 | 2.1 |
| Unknown | 58 | 7 |
| Total | 828 | 100 |
Table 2: The different type of poisons ingested by the patients admitted
| Medicinal drugs | Count | Percentage (%) |
|---|---|---|
| PCM | 272 | 58.5 |
| Chlorpheniramine | 33 | 7.1 |
| Salbutamol | 16 | 3.4 |
| Antiasthmatic | 3 | 0.6 |
| NSAIDS | 6 | 1.3 |
| Antibiotics | 9 | 1.9 |
| Antihyperglycemic | 17 | 3.7 |
| Antihypertensive | 9 | 1.9 |
| Benzodiazepine | 21 | 4.5 |
| Antipsychotics | 47 | 10.1 |
| Other Med Multi drugs |
32 62 |
6.9 12.5 |
| Total | 527 | 100 |
Table 3: Pattern of medicinal drug overdose
Only 15.97% (95) patients had been administered activated charcoal within 2 hours of ingestion. Mean hospital stay of an acutely poisoned patient was 3.49 (SD 4.97) days. Only 7 patients needed intensive care and of that 6 patients have ingested organophosphates. Fourteen (1.7%) patients admitted following acute poisoning to Colombo South Teaching Hospital died (Table 4). Majority 82.6% (684) were discharged alive and 3.00% (25) had been transferred to other hospitals for further care mainly due to unavailability of antidotes.
| Type of the Poison ingested | Number of patients died and the percentatge (%) |
|---|---|
| OP & Rodenticide | 6 (42.9%) |
| Paraquat | 4 (28.6%) |
| Domestic & industrial chemicals | 2 (14.28% ) |
| Paracetamol | 1 (7.14) |
| Carbamate | 1 (7.14) |
Table 4: Deaths according to the poison ingested
According to what has been reported previously, Sri Lanka is known as a country where the rate of pesticide poisoning is high [5]. Though this is true with the agricultural areas where most of the previously published studies have been done, the pattern of poisoning in urban part of the country is different. In this study which, was performed in an urban area of the western province of Sri Lanka we found that medicinal drug overdose accounts for approximately 64% of the poisoning admissions in contrast to 6-12% of medicinal drug overdose reported from agricultural areas [5]. This confirms the pattern identified by de Silva et al. in 2008 at the National Hospital of Sri lanka which reported that medicinal drug overdose accounts for 68% of total self-poisonings [6]. Pestcides accounted for only 14% of poisoning in this study in contrast to approximately 60% reported in 2003 [2]. Acute paracetamol poisoning accounted for 58.5% of the ingestions and chlorpheneramine accounted for 12%. This reflects the fact that the availability determines the type of poison ingested. In rural agricultural communities pesticides are freely available and they have become the choice compared to urban areas where pesticides are not available, the choice is mainly the over the counter drugs. More females have admitted following acute poisoning acounting for 61% of total poisoning admissions. In 2005 the males prodominated with 57% from agricultural areas and in 2008 it was reported that more females were admitted following poison ingestion accounting for 73% in the urban areas of the country [6]. The trend we see in the urban areas is somewhat similar to what has been observed in the industrialized countries where non-fatal self-harm rates are reported to be high in females [7].
Two hundred and twenty nine females in the age group of 12-20 years and 194 females in the age group of 21-30 years were admitted to CSTH following acute poisoning in the year 2009. In contrast the number of male patients were highest in the age group of 21-30 years. However the highest numbers were at the ages of 12-30 years, which represents the economically productive young age group. After 30 years the incidence of poisoning drastically reduced. In China, the suicide rates do tend to increase with age but there is a notable peak in rates amongst males and females aged 20-25. Recent data show that this peak is more prominent in rural localities [8]. In rural India rates of suicide in 15-24 year old females are higher than rates in males of the same age and most other female age groups [9]. Similar patterns are seen in Sri Lanka [2]. Only a few patients (n=7) needed intensive care facilities and of that 6 were due to OP poisoning. The number of hospital stay and the death rates are less than those reported in the agricultural areas of the country reflecting the fact that ingestion of pesticides causes more morbidity and mortality. In contrast most of the medicinal drug overdoses are less lethal and easily managed thus the morbidity and mortality are less. Decontamination techniques have been used inappropriately. Though there is no evidence to suggest that use of gastic lavage beyond 1-2 hours of poisoning is effective, the mean time since ingestion to gastric lavage in these patients is 5.04 (SD 9.78) hours. Only 17.2% of the patients were given gastric lavage within 2 hours of poisoning. Therefore the basic principles of management of poisoning needs to be established and strengthened in this part of the country.
Pattern of poisoning is different in different parts of Sri Lanka, thus the problems encountered are different. Though the past research has consistently stressed the fact that the acute pesticide poisoning is a major problem in Sri Lanka, it is no so in the more urbanised areas where paracetamol poisoning is the major cause for hospital admissions following acuet poisoning. The basic principle of management of poisoning needs to be established and strengthened in this part of the country.
We would like to acknowledge the support given by the medical director, the nursing staff of the general medical wards and the consultant physicians of the respective units of the Colombo South Teaching Hospital. We specially acknowledge the support extended by the staff of the medical records room of the Colombo South Teaching Hospital. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.