Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2015) Volume 5, Issue 3
Objective: We designed a study with a primary objective of comparing the effectiveness of nasal continuous positive airway pressure (nCPAP) versus bi-level CPAP (BiPAP) as the primary mode of non-invasive ventilation in preterm newborns. The primary outcome was need for invasive ventilation in the first 120 hours of life. The secondary objective was to compare these two groups regarding duration of non-invasive ventilation, use of surfactant, incidence of pneumothorax, bronchopulmonary dysplasia (BPD), peri and intraventricular haemorrhage (PIVH), necrotizing enterocolitis (NEC), retinopathy of prematurity (ROP), sepsis, length of hospitalisation and mortality.
Methods: Prospective, multicentre clinical trial enrolling 220 neonates born at 27 to 32+6 weeks of gestation randomly assigned at birth for either CPAP or BiPAP.
Results: One hundred and nine neonates received NCPAP and 111 BiPAP. Invasive ventilation was needed in 18.3% in the CPAP group and 14.4% in the BiPAP group. This difference was not statistically significant. However, when stratifying the groups regarding gestational age (GA), we found a tendency favouring BiPAP in subgroup of 30 to 32+6 weeks. There was no difference regarding the secondary outcomes, except for an increase in NEC in the CPAP group. Multivariate analysis demonstrated a significant association between absence of premature rupture of membranes and the need of invasive ventilation within the first 120 hours of life, independently on the assigned mode of non invasive ventilation.
Conclusion: BiPAP and CPAP are both effective and safe as a primary mode of ventilation in preterms between 27 and 32+6 weeks without important complications. In a subgroup of 30 to 32+6 weeks of gestation a better outcome using BiPAP was observed.
Keywords: Non-invasive ventilation; Continuous positive airway pressure (CPAP); Bilevel CPAP; Preterm; Randomized controlled trial.
Since the 1970’s, non-invasive ventilation (NIV) in newborns with nasal CPAP (nCPAP) has been increasingly used. Subsequent studies demonstrated that it contributes to a reduction in the need and dependence of oxygen and respiratory rate as well as the need for mechanical ventilation [1-2].
Nasal CPAP establishes a continuous distension pressure (CDP) throughout the respiratory cycle, which is fundamental to restore the functional residual capacity, reduce working of breath and stabilize the respiratory pattern [3-4].
It is now becoming widely used in the delivery room because if it is applied from the first breaths, it will help in obtaining lung volume stabilization [5]. It creates and maintains a functional residual capacity, facilitates gas exchange and minimizes acute lung injury [6].
Bilevel CPAP (BiPAP) provides two levels of positive end expiratory pressure (PEEP) during the respiratory cycle of the patient with a frequency and a duration determined by the physician. Theoretically, BiPAP should allow a higher alveolar recruitment, a higher residual function capacity and a reduction in breath working when compared to nCPAP. Nevertheless, it hasn´t yet been proved in clinical studies. This advantage could also decrease mortality associated with neonatal ventilation and chronic lung disease with important economic impact. Some studies showed that there was no clear demonstration of a reduction of bronchopulmonary dysplasia (BPD) with the use of non-invasive ventilation [7-10]. However, recent meta-analysis made by Schmolzer [11] and Fischer [12] demonstrated that there is a statistically significant advantage in the use of non-invasive ventilation regarding death and BPD.
Gianlucca Lista hypothesized that bilevel CPAP seems to be efficient when used in preterms in the acute phase of moderate respiratory distress syndrome (RDS) [13].
These published studies use BIPAP as a secondary mode of ventilation, e.g. that after extubation. To our knowledge, there are no studies comparing CPAP and BIPAP applied immediately after birth in preterms born 27 to 32 weeks and 6 days.
The main purpose of this study is to compare nCPAP and BiPAP as a first intention mode of non-invasive ventilation in a sample of preterms with gestational age between 27 weeks and 32 weeks and 6 days.
This randomized controlled trial (RCT) was conducted from May 2011 to March 2013 in two tertiary Neonatal Intensive Care Unit (NICU) in Lisbon, Portugal (Hospital Prof Dr. Fernando Fonseca, and Maternidade Dr. Alfredo da Costa - CHLC), with a total of 20 Intensive and 50 intermediate care beds.
It included the inborn infants with gestational age (GA) between 27 weeks and 32 weeks+6 days, whose parents had signed an informed consent before delivery.
Exclusion criteria: need of endotracheal intubation in the delivery room, major congenital malformations, neuromuscular diseases, perinatal asphyxia (Apgar<4 at 5 minutes and base excess of ≥ -12 in the first hour) and early onset sepsis.
The study protocol was approved by both Hospital Ethics Committees. It is registered in the Biomed Central under the number ISRCTN11928413.
At birth, delayed cord clamping was made. The baby was placed in a polyethylene bag only with the face uncovered under the radiant warmer. An oxysensor was placed on the right fist/hand to obtain pre-ductal oxygen saturation. Babies who showed an effective respiratory drive in the delivery room were immediately connected to an Infant Flow device for non-invasive ventilation (nCPAP-PEEP of 6 cm H2O; fraction of inspired oxygen requirement (FiO2) 40%) and transferred to the NICU. To those who didn’t have well succeeded breathing movements, positive pressure ventilation via T-piece resuscitator with silicone mask was applied (positive inspiratory pressure (PIP) 16-20 cm H2O, PEEP 6 cm H2O at a rate of 1 insufflation per minute; FiO2 30-40%). If an effective breath was achieved in 30 seconds, the previous procedure was followed. If there was no improvement, resuscitation should continue and a new evaluation should be done at 60 seconds of life. If heart rate (HR) was below 100, the newborn would be intubated and invasive ventilation applied. If HR was above 100, the baby would be connected to Infant Flow device with the same parameters described above and transferred to the NICU.
At NICU admission, enrolled infants were randomly assigned to nCPAP or BiPAP using sequentially numbered sealed opaque envelopes. Randomization by variable 2-4 blocks was stratified in two GA categories: 27 weeks to 29 weeks+6 days of GA and 30 weeks to 32 weeks +6 days. The study was not blinded.
In this study it was exclusively used Infant Flow® devices - Infant Flow® Nasal CPAP System (IF; Care Fusion) and Infant Flow® SiPAP System (Vyasis, Care Fusion) and the nasal interfaces were short binasal prongs.
Protocol procedure is shown in Figure 1.
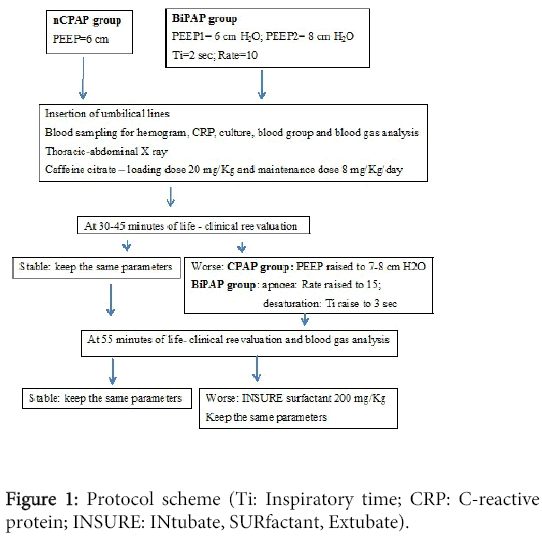
Figure 1: Protocol scheme (Ti: Inspiratory time; CRP: C-reactive protein; INSURE: INtubate, SURfactant, Extubate).
In the CPAP group a PEEP of 6 cm H2O was applied. In the BiPAP group a PEEP1 of 6 cm H2O and PEEP2 8 cm H2O, an inspiratory time (ti) of 2 seconds and a respiratory rate (RR) of 10. We decided to use a respiratory rate of 10 and provide a longer time of PEEP 2 (2 seconds) for more alveolar distension. In both groups, oxygen was administred in order to achieve a transcutaneous saturation 85-92%.
Heart rate, respiratory rate, systemic blood pressure and transcutaneous oxygen saturation were continuously measured.
At 30-45 minutes of life, after insertion of umbilical catheters, X-ray, blood sampling for hemogram, C-reactive protein (CRP), cultures and gas analysis and administration of a loading dose of caffeine, a clinical evaluation was made. If the baby didn´t show clinical signs of respiratory distress (grunting, tachypnea or apnoea) or desaturation (saturation of oxygen<85%) the same parameters were kept. If there was any sign of respiratory distress or saturation<85% the following modifications were performed:
In the CPAP group, PEEP would be raised to 7-8 cm H2O; in the BiPAP group, if there was apnoea, RR would be increased to 15; if there was desaturation or other signs of respiratory distress, ti would be raised to 3 seconds.
At 55 minutes of life a new evaluation was made, based on signs of respiratory distress described above, and gas blood analysis (arterial or capillary if the insertion of the arterial umbilical catheter was not possible). If there was any sign of clinical deterioration or transcutaneous saturation of oxygen below 85% with FiO2 above 50% and/or there was blood gas deterioration (pH<7.20 and/or pCO2>65 mmHg), intubation and administration of porcine surfactant (Curosurf®) 200 mg/Kg were performed and immediate extubation to non-invasive ventilation (INSURE method) with the previous parameters was done.
An arterial blood gas analysis was made every two hours in the first 6 hours and then at 12 hours of life. Then, it was done at least twice a day.
Between the 24 to 72 hours of life, cardiac and transfontanellar ultrasound were performed.
If significant patent ductus arteriosus was diagnosed, ibuprofen would be prescribed according to the National Neonatal Guidelines.
The remaining diagnosis and treatment procedures were conducted according to the National Guidelines.
Besides all data directly related to ventilation, other variables were analyzed: prenatal and demographic data, outcome at discharge and length of stay. Prenatal data included the use of antibiotics prior to birth (in case of premature rupture of membranes (PROM) or labour).
The primary outcome of our study was the need of invasive ventilation within the first 120 hours of life. We decided to consider only the first 5 days of life because after that time there is an increasing probability of confounding variables (such as patency of ductus arteriosus or late onset sepsis) not related with the purpose of our study.
Stratification was initially intended for randomization purposes, with random variable 2-4 blocks, to better guarantee an equal allocation number to each treatment group, despite an increasing number of patients with increase in gestational age. In a Post Hoc analysis we decided to compare the GA subgroups, complementary to GA as a continuous variable.
Intubation criteria were: pH<7.25, pCO2>65 mmHg, SatO2<88% with FiO2≥40%, one episode of apnoea requiring bag-and-mask ventilation, frequent episodes of bradycardia/apnoea (>2-3 per hour).
Secondary outcomes were duration of non-invasive ventilation, use of surfactant, incidence of pneumothorax, bronchopulmonary dysplasia (BPD-defined as need of oxygen supplementation at 36 weeks of gestation), peri and intraventricular haemorrhage (Volpe grades III/IV), necrotizing enterocolitis (Bell´s stage >2), severe retinopathy of prematurity (grade>2), patent ductus arteriosus (PDA), sepsis (defined as positive hemoculture, clinical signs and intention to treat, all together), length of stay and mortality.
A sample size of 200 patients was needed to show an absolute reduction in the need of ventilation from 35% to 15% (alpha 0.05; beta 0.80; 2 tailed test).
Baseline group characteristics were compared. Statistical analyses were performed using SPSS version 13 and STATA version 11 and an intention-to-treat analysis was performed. Protocol violation was considered if there was a crossover before 120 hours of life.
For normally distributed variables we used t-test for 2 independent variables, otherwise, in non-parametric data, Mann-Whitney U test was used. Dealing with frequencies, we used chi-square and exact Fisher test whenever applicable. Logistic regression analysis with the primary binary outcome, was adjusted with covariables with p<0.2 in bivariate analysis and clinical relevant variables. The Regression Backward and Enter Conditional Method was used. Statistical significance was at the p<0.05 level.
Two hundred and twenty neonates were eligible for the study. For six patients, there was a protocol violation (crossover before 120 hours of life). Five of them were initially allocated to the BIPAP group and only one of them was intubated and ventilated. The other patient was initially allocated to the CPAP group and after the crossover was intubated and ventilated.
In the CPAP group there were 109 neonates: 31 (28.7%) with GA between 27 and 29 weeks+6 days and 78 (71.3%) with GA 30 to 32 weeks+6 days. BiPAP group consisted of 111 neonates: 31(27.9%) between 27 and 29 weeks+6 days and 80 (72.1%) with GA from 30 to 32 weeks+6 days. No statistical difference in the stratification by GA between these two groups was found (p=0.8).
There were no differences regarding gender, gestational age, birth weight, mother’s age, use of antenatal steroids, antenatal antibiotics.
There were no differences regarding gender, gestational age, birth weight, mother’s age, use of antenatal steroids, antenatal antibiotics.
There were no differences regarding gender, gestational age, birth weight, mother’s age, use of antenatal steroids, antenatal antibiotics and type of delivery between these two groups (Table 1). Premature rupture of membranes (PROM) was present in more patients in the CPAP group than in the BiPAP group.
| NCPAP (n=109) | BiLevel (n=111) | p | Test | ||
|---|---|---|---|---|---|
| GA (weeks) | Median [Q1-Q3] | 30,9 (29,7-32,1) | 31,1 (29,7-32,0) | 0.97 | Mann-Whitney U |
| Weight (grams) | Mean [SD] | 1373 (362) | 1355 (382) | 0.73 | t test |
| Mother age (years) | Median [Q1-Q3] | 31 (26-35) | 31 (28-34) | 0.78 | Mann-Whitney U |
| SGA (<P3) | n (%) | 23 (21,1) | 30 (27) | 0.3 | Chi-square |
| Antenatal Steroids | n (%) | 107 (98,1) | 107 (96,9) | 0.68 | Chi-square |
| Multiple | n (%) | 47 (43,1) | 43 (38,7) | 0.5 | Chi-square |
| Male | n (%) | 52 (47,7) | 48 (43,2) | 0.47 | Chi-square |
| Cesarean | n (%) | 82 (72,2) | 89 (80,2) | 0.38 | Chi-square |
| PROM (Hours) | Median [Q1-Q3] | 17 (3,25-68) | 32 (3,0-96) | 0.37 | Chi-square |
| PROM | n (%) | 41 (37,6) | 29 (26,1) | 0.6 | Chi-square |
| Prenatal AB | n (%) | 48 (44) | 44 (39,6) | 0.51 | Chi-square |
Table 1: Antenatal and demographic data (GA: Gestational Age; SGA: Small for Gestational Age; PROM: Premature Rupture of Membranes; AB: Antibiotics).
The primary outcome, the need of invasive ventilation within the first 120 hours after birth, was not significantly different between treatment groups (CPAP 18.3%, BiPAP 14.4%, OR 1.6 CI 0.76-3,4). However, there was a tendency in the subgroup of GA 30 to 32 weeks+6 days being lesser in the BiPAP group (11.0% vs 4.5% p=0.076; Table 2).
| Primary outcome: | NCPAP (n=109) | BiLevel (n=111) | p | Test | |
|---|---|---|---|---|---|
| Invasive MV until 120h life | n (%) fail | 20 (18,3) | 16 (14,4) | 0,43 | Chi-square |
| 27 - 29w+6d | n (%) fail | 8 (7,3) | 11 (9,9) | 0,41 | Chi-square |
| 30 - 32w+6d | n (%) fail | 12 (11,0) | 5 (4,5) | 0,076 | Fisher's Exact Test |
Table 2: Primary outcome (MV: Mechanical Ventilation).
Secondary outcomes are detailed in Table 3. There was no statistically significant difference between the two groups, except in the incidence of NEC, which was more frequent in the NCPAP group (5.5% vs 0.9% p=0.064). There were only 2 deaths, one in the CPAP group and another in the BIPAP group. Multivariate analysis demonstrated a significant association between absence of PROM and need of invasive ventilation within the first 120 hours of life, independently of the mode assigned (Table 4).
| Secondary outcomes: | NCPAP (n=109) | BiLevel (n=111) | p | Test | ||
|---|---|---|---|---|---|---|
| Time of NIV (h) | Median [Q1-Q3] | 45 (15,8-113,7) | 44,9 (23,7-115,1) | 0,31 | Mann-Whitney U | |
| 27 - 29w+6d | Median [Q1-Q3] | 84,5 (14,3-168,5) | 49,3 (21,8-182,4) | 0,6 | Mann-Whitney U | |
| 30 - 32w+6d | Median [Q1-Q3] | 37,7 (17,3-90,3) | 44,2 (23,8-102) | 0,4 | Mann-Whitney U | |
| Surfactant use | n (%) | 26 (23,8) | 25 (22,9) | 0,79 | Chi-square | |
| Pneumothorax | n (%) | 5 (4,6) | 2 (1,8) | 0,28 | Fisher's Exact Test | |
| 27 - 29w+6d | n (%) | 1 (3,3) | 2 (6,4) | >0,9 | Fisher's Exact Test | |
| 30 - 32w+6d | n (%) | 4 (5,1) | 0 | |||
| O2 need at CGA 36wks | n (%) | 5 (4,6) | 8 (7,2) | 0,41 | Chi-square | |
| 27 - 29w+6d | n (%) | 5 (16,1) | 5 (16,1) | >0,9 | Fisher's Exact Test | |
| 30 - 32w+6d | n (%) | 0 | 3 (4) | |||
| PDA | n (%) | 7 (6,5) | 10 (9) | 0,49 | Chi-square | |
| 27 - 29w+6d | n (%) | 5 /16,7) | 7 (22,6) | 0,56 | Chi-square | |
| 30 - 32w+6d | n (%) | 2 (2,6) | 3 (3,8) | >0,9 | Fisher's Exact Test | |
| NEC (Bell´s grade >2) | n (%) | 6 (5,5) | 1 (0,9) | 0,28 | Fisher's Exact Test | |
| 27 - 29w+6d | n (%) | 3 (9,7) | 1 (3,2) | 0,61 | Fisher's Exact Test | |
| 30 - 32w+6d | n (%) | 3 (3,8) | 0 | |||
| Severe IPVH (>2) | n (%) | 1 (0,9) | 4 (3,7) | 0,37 | Fisher's Exact Test | |
| 27 - 29w+6d | n (%) | 1 (3,3) | 4 (12,9) | 0,35 | Fisher's Exact Test | |
| 30 - 32w+6d | n (%) | 0 | 0 | |||
| Severe ROP (>2) | n (%) | 0 | 0 | |||
| Any late Sepsis | n (%) | 14 (12,8) | 12 (10,8) | 0,64 | Chi-square | |
| 27 - 29w+6d | n (%) | 8 (25,8) | 9 (26,1) | >0,9 | Chi-square | |
| 30 - 32w+6d | n (%) | 6 (7,7) | 3 (3,8) | 0,32 | Fisher's Exact Test | |
| Mortality | n (%) | 1 (0,9) | 1 (0,9) | 1 | Fisher's Exact Test | |
| 27 - 29w+6d | n (%) | 1 (3,3) | 0 (0) | >0,9 | Fisher's Exact Test | |
| 30 - 32w+6d | n (%) | 0 (0) | 1 (0,6) | >0,9 | Fisher's Exact Test | |
| Survivors only: | NCPAP (n=108) | BiLevel (n=110) | p | Test | ||
| O2 need (days) | Median [Q1-Q3] | 4 (1-10) | 5 (2-11) | 0,44 | Mann-Whitney U | |
| 27 - 29w+6d | Median [Q1-Q3] | 14 (4-33,3) | 22 (8,3-41) | 0,27 | Mann-Whitney U | |
| 30 - 32w+6d | Median [Q1-Q3] | 3,5 (1-7) | 4 (1-6) | 0,78 | Mann-Whitney U | |
| O2 need CGA (weeks) | Median [Q1-Q3] | 32,3 (31,5-32,7) | 31,3 (32,1-33,1) | 0,36 | Mann-Whitney U | |
| 27 - 29w+6d | Median [Q1-Q3] | 31,4 (29,5-33,3) | 32,4 (30,1-33,7) | 0,53 | Mann-Whitney U | |
| 30 - 32w+6d | Median [Q1-Q3] | 32,3 (31,8-32,7) | 32,3 (35,6-33,6) | 0,41 | Mann-Whitney U | |
| LOS (days) | Median [Q1-Q3] | 33 (23-47) | 32 (23-47) | 0,83 | Mann-Whitney U | |
| 27 - 29w+6d | Median [Q1-Q3] | 52 (40-61) | 53 (45,7-66,5) | 0,22 | Mann-Whitney U | |
| 30 - 32w+6d | Median [Q1-Q3] | 27 (25-35,3) | 27 (20-36) | 0,7 | Mann-Whitney U | |
Table 3: Secondary outcomes.
| Need of Invasive MV | p | OR | 95% CI | |
| BiLevelvs NCPAP | 0,21 | 1,6 | 0,76 | 3,4 |
| PROM | 0,014 | 3,6 | 1,3 | 9,7 |
Table 4: Multivariate analysis (outcome variable “need of invasive ventilation”, adjusted for covariables ”PROM“ and ”Randomization group”).
Non-invasive ventilation is an excellent method to assist preterm neonates, allowing a good ventilation and oxygenation and avoiding intubation and the consequences of invasive ventilation. It is used in several clinical circumstances and it includes different modes that can be applied. A recent meta-analysis performed by Schmolzer et al. showed that nCPAP initiated in the delivery room compared with intubation reduces death or bronchopulmonary dysplasia in very preterm babies [11].
The use of CPAP and BiPAP as a mode of ventilation after extubation has already been studied. O´Brien et al. randomized 136 infants less than 1250 g to one or other mode and found no difference in successful extubation at 7 days [14].
Lampland et al. conducted a study enrolling 20 neonates with GA 24 weeks+3 days to 31weeks+4 days to test if there was an improvement in CO2 removal with the use of BiPAP. Nineteen of them had previous intubation and mechanical ventilation and were at an average 33 days of age. The authors compared CPAP and BiPAP in the same patient for a period of one hour and found that BiPAP didn´t improve removal of CO2, oxygenation and other physiological parameters [15]. Non-invasive ventilation has also being used for moderate RDS. There is one RCT by Lista et al. where the secondary outcome demonstrated that preterm receiving BIPAP one hour after birth had fewer days of respiratory support and supplemental oxygen [13].
It may be expected that BiPAP could have some preferences over CPAP because a higher level of pressure would allow a better gas exchange. The studies published are considering the use of BiPAP after extubation but not as a first intention mode. Hence, we carried out this investigation to evaluate if there is any advantage of one mode over the other immediately after birth. The randomly allocated groups had no difference regarding the prenatal and demographic variables, except for PROM (less frequent in the BiPAP group).
These two modes were evaluated regarding the need of intubation within the first 120 hours. Overall, we found no statistically significant difference between these two groups, although in the subgroup of 30 to 32+6 weeks gestation, BiPAP mode had less need of invasive ventilation (11,0% vs 4,5% p=0,076) After performing an analysis based on the intention-to-treat we found a tendency (but not statistically significant) of the preference of BIPAP over CPAP. We speculate that this might happen because a second level of pressure allows more alveolar distension and better gas exchange in a group with a more alveolar maturity and better lung compliance. An optimal surface for gas exchange can be achieved with a higher level of pressure in a more stable lung.
In the lower age group (27 to 29+6 GA) the effect is not noticed, probably because of immaturity of the lung function. A higher pressure will not additionally distend alveoli with small dimensions and less surfactant. Another possibility is that in this group a higher PEEP would provoke overdistension of the alveoli and, thus, not allowing a good gas exchange. Possibly, the more immature the infant is, the lower pressure will be needed.
Concerning secondary outcomes, the two groups were similar in respect to most of them except for NEC. We found a slightly higher incidence of NEC (Bell´s stage>2) in the CPAP group (5.5% vs 0.9% p=0.28), but the number of newborns who presented this condition is very small and so only a tendency can be speculated.
By multivariate analysis, adjusting for confounding variables, there is a protective effect if there is not PROM probably because PROM implicates infection and inflammatory mediators exposure.
As a limitation of this study, we could consider the sample size. Indeed, a larger number of patients would reinforce the main results of this work.
In summary, BiPAP and CPAP are both effective and safe as a primary mode of ventilation in preterms between 27 and 32+6 weeks without important complications. In a subgroup of 30 to 32+6 weeks of gestation there was a tendency to have better (although not statistically significant) results using BIPAP.
The authors thank Dr. Catarina Costa for her contribution in the statistical analysis, the entire medical and nurse staff of both NICU and section of Neonatology of the Portuguese Society of Paediatrics (Abbott grant) for financial support.