Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2015) Volume 5, Issue 1
Background: Within the past few years, minimally invasive surgical (MIS) techniques fortotal knee arthroplasy (TKA) have emerged as promising alternatives to conventional TKA, possibly because of less surgical trauma to the quadriceps. The purpose of this investigation was to evaluate the efficacy of MIS TKA outcomes compared to conventional TKA.
Methods: Forty-four patients, aged 50-85 years (64.3 ± 8.4 mean ± SD; 22 females, 22 males) who were scheduled for a unilateral TKA secondary to osteoarthritis were enrolled in a prospective randomized controlled trial. Patients were excluded if they had cardiopulmonary, neurological, or other unstable orthopedic conditions that limited function; uncontrolled diabetes; or a BMI ≥ 40 kg/m2. Patients were blinded and randomly assigned to one of two surgical groups: MIS or conventional. All patients completed a standardized course of rehabilitation following surgery. Patients were assessed preoperatively and 4, 12, 26, and 52 weeks postoperatively by a blinded evaluator; the 26- and 52-week
outcomes are the focus of the present manuscript. Outcomes included isometric quadriceps strength (primary outcome), isometric hamstrings strength, quadriceps activation, active knee range of motion (AROM), the six-minute walk (6MW) test, pain at rest and with 6MW, timed-up-and-go test (TUG), the stair climbing test, the Short Form 36 Health Status questionnaire (SF-36) the Western Ontario and McMaster Osteoarthritis Index (WOMAC), and leg muscle mass.
Results: There were no differences between groups at baseline. At 26 and 52 weeks postoperatively, there were no difference between MIS and control groups for any outcome measure.
Conclusions: Although the MIS surgical technique for TKA may lead to faster recovery of strength in patients undergoing TKA (previously reported at 4 weeks postoperatively), there is no apparent benefit of MIS on the longerterm recovery of strength or functional performance. Therefore, the benefits of MIS TKA may not outweigh the risks associated with limited surgical visualization.
Keywords: Total knee arthroplasty; Minimally invasive surgery; Knee; Quadriceps; Rehabilitation
While TKA reliably reduces pain and improves function in patients with knee osteoarthritis, recovery of quadriceps strength to normal levels is not common. The substantial tension and trauma to the quadriceps muscle during TKA surgery may cause permanent quadriceps muscle dysfunction, as evidenced by long-term post-operative weakness that impairs physical function [1-5]. Quadriceps strength declines precipitously after TKA, with reports of strength loss of 50-60% within the first month after surgery [2,3]. Inadequate recovery of muscle strength leads to corresponding deficits in functional performance. Walking performance remains almost 27% less than healthy agematched older adults and more physically demanding tasks, such as stair climbing, take twice as long as healthy older adults [4].
Conventional TKA has consistently led to reproducible results, but minimally invasive TKA has been touted as a promising alternative to conventional TKA [6-15]. The extensive interest in minimally invasive TKA surgery has been largely spurred by market- and patient-driven demand. In particular, patients often believe that less invasive should be better, without fully accepting the potential risks associated with this new procedure. While initial investigations suggested that MIS TKA might reduce hospital stays, decrease postoperative pain, and enable individuals to return to functional activities more quickly than conventional TKA [1,6,7,15-18], more recent studies suggest fewer benefits of MIS TKA to outweigh the risks associated with limited visualization during surgery [9,12,17-20]. Many of the initial studies were based on retrospective cohort studies, where patients were hand selected [1,6,7,16-18], and there have been few prospective randomized, controlled clinical trials. In addition, previous investigations relied on self-reports of physical function, rather than performance-based tests of physical function, such as speed on a timed stair climbing test. Yet, performance-based assessments are more responsive to changes in muscle strength and physical performance and selfreport questionnaires tend to be more closely linked to pain relief than performance capabilities [21,22]. Furthermore, few studies have standardized variability in post-operative rehabilitation.
We previously reported early results from a prospective randomized controlled trial comparing MIS and conventional TKA procedures (before, 4 weeks, and 12 weeks after TKA) [23]. The current manuscript expands upon those findings by reporting results 26 and 52 weeks after TKA. As such, the aim was to evaluate the efficacy of MIS TKA in improving functional outcomes in a blinded, prospective, randomized controlled trial (RCT). We hypothesized that MIS TKA would decrease quadriceps and hamstrings strength loss, attenuate quadriceps activation deficits, improve functional performance, increase knee ROM, decrease knee pain, and attenuate muscle mass loss when compared with conventional TKA surgery.
Design overview
This was a prospective, randomized, controlled trial with a 1-year follow-up to evaluate potential benefits of MIS TKA. Patients meeting inclusion criteria were randomized using concealed allocation to a MIS or conventional (CONTROL) TKA group. Randomization included stratification for sex and decade of age. Patients were assessed 1-2 weeks before surgery and 4, 12, 26, and 52 weeks after TKA, although this manuscript focuses on longer term outcomes at 26 and 52 weeks after TKA. All testing was performed at the Clinical and Translational Research Center at the (blinded). This study was approved by the (blinded) and conducted in conformity with ethical principles of research. Informed consent was obtained from all participants. This study is registered at www.clinicaltrials.gov, registry number (blinded). None of the authors had conflicts of interest with this study.
Setting and participants
Patients anticipating a primary, unilateral knee replacement for OA, aged 50-85 years who met the following inclusion criteria were enrolled between December 2006 and June 2010: 1) no significant neurologic impairments, 2) no uncontrolled hypertension, 3) minimal contralateral knee OA (as defined by pain greater than 5/10 with activity), and 4) no other unstable lower-extremity orthopedic conditions. In addition, although only half of the patients were randomized for MIS, all patients met additional criteria for MIS eligibility: 1) minimum of 80° degrees of active knee flexion, 2) no greater than 15° knee varus, 15° valgus, and 3) body mass index ≤ 40 kg/m2.
Randomization and interventions
Blocked randomization was used to assure balanced assignment of subjects to the two intervention groups by sex and decade of age, with random block sizes of 4, 6, or 8. Group assignment occurred after enrollment criteria were met and after the preoperative testing session. Except for the surgeon performing the TKA, patients, investigators, and treating physical therapists were all blinded to group assignment because identical skin incision lengths were used for both groups.
Surgical approach
Both conventional (CONTROL) and MIS TKA approaches were performed using a medial parapatellar approach with an anterior midline incision by a single surgeon as previously described [23]. Briefly, surgery for both study groups began with patellar resurfacing, then proceeded with proximal tibial resection, followed by resurfacing of the femur with distal cut, then anterior, posterior, chamfer and notch cuts. The MIS group had the extensor mechanism dissection length limited to the distance from superior patella distal to the proximal tibial tubercle. The proximal arthrotomy for the MIS group was limited by a stay suture placed no more than 1 cm cephalad to the superior patella placed at the time of arthrotomy. The distal extent of the deep incision in the MIS group was limited to a distance of no more than 1 cm distal to the join line. In cases of the CONTROL group, a conventional arthrotomy with no limitation in the length of the deep incision was used; the proximal extent was 4-6 cm cephalad to the superior patella and the distal extent was extended to most inferior portion of the tibial tubercle. Patella eversion was not used for MIS procedures, but was used for CONTROLS. All TKA procedures utilized mobile-bearing, cemented implants using a P.F.C. Sigma Rotating Platform Knee System by DePuy (Johnson & Johnson). Tourniquet application throughout the TKA procedure was identical for both groups. Finally, identical superficial incision lengths for both groups allowed for patient blinding to surgical group because neither patients nor investigators were able to discern cosmetic differences between groups.
Rehabilitation
All patients were provided the same standard rehabilitation protocol for TKA, consisting of a standard set of core exercises as previously described [23,24]. Briefly, patients received inpatient rehabilitation twice daily for approximately 3 days. Following hospital discharge, patients were treated at home for 6 visits over 2 weeks and then began outpatient physical therapy for 10-12 visits over 6 weeks. Specifics of the interventions used have been previously described [23,24]. Physical therapists reported on treatment sessions via a detailed flow sheet that were monitored for treatment consistency.
Pain management
Post-operative pain management was identical for all study participants. A multi-modal perioperative pain protocol was used for all patients undergoing TKA, regardless of group. The protocol included 1) pre-operative femoral block with indwelling catheter for 36 hours post-operative, 2) pre-operative sciatic single shot block, 3) twice daily administration of oral Cyclooxygenase-2 (COX-2) inhibitor while inpatient; and 4) the addition of post-operative immediate release opioids as needed. No extended release oral agents were utilized. Further, use of post-operative nonsteroidal anti-inflammatory drugs (NSAIDs) beyond the inpatient stay was avoided due to concurrent administration of fractionated heparin anti-coagulant.
Outcomes and follow-up
Isometric quadriceps torque and activation testing: Maximal isometric quadriceps muscle torque and activation testing were performed using a doublet interpolation test, as described previously [24,25]. Torque was measured using a HUMAC NORM (CSMi, Stoughton, MA) electromechanical dynamometer. Data were collected using a Biopac Data Acquisition System and a Grass S48 stimulator with a Grass Model SIU8T stimulus isolation unit (Grass Instruments, West Warwick, RI) was used for testing voluntary muscle activation via self-adherent, flexible electrodes (7.6 × 12.7 cm, Supertrodes, SME, Inc). Voluntary activation of the quadriceps muscle was assessed at 60° of knee flexion using the doublet interpolation technique, where a supramaximal stimulus (2-pulse, 600-μs pulse duration, 100-Hz electrical train) was applied during an maximum voluntary isometric contraction (MVIC) and again, immediately afterwards, while the quadriceps muscle was at rest [25-27]. A value of 100% represents full voluntary muscle activation; less than 100% indicates incomplete motor unit recruitment or decreased motor unit discharge rates [26-28].
Isometric hamstrings torque: The same positioning described for quadriceps torque measurements was used for hamstrings torque assessments, although no hamstrings muscle activation testing was performed. Both quadriceps and hamstrings measures were performed twice, with a third trial if maximal torque differed by more than 5%.
Functional performance measures: Functional performance was assess using the stair climbing test (SCT), timed-up-and-go test (TUG) and 6-minute walk test (6MW), as previously described [24]. The SCT measures the total time to ascend, turn around, and descend a flight of stairs [29]. The TUG measures the time to rise from an arm chair, walk 3m, turn around, and return to sitting in the same chair without physical assistance [30]. The 6MW measures the distance walked over 6 minutes to evaluate endurance and has been validated as a measure of functional mobility following knee arthroplasty [31]. Pain during the 6MW test was measured utilizing an 11-point verbal numeric pain rating scale (NPRS). Patients were asked to rate their pain towards the end of the 6MW on a scale of 0 to 10 with 0 representing no pain and 10 representing the worst pain imaginable. Patients were also asked to report their pain levels using the NPRS at rest.
Range of motion: Active ROM (AROM) of the knee was measured in supine with a long-arm goniometer as previously described [24,32]. Active knee extension was measured with the heel on a 4-inch block while the participant actively extended the knee. Active knee flexion was measured with the participant actively flexed the knee as far as possible while keeping the heel on the supporting surface.
Health status questionnaires:
Short form-36: Health status was assessed using the Physical and Mental Component Scores (PCS and MCS) of the Short Form-36 (SF- 36). The SF-36 has been shown to capture improvements in 7 of its 8 domains in patients after TKA within the first 3 months after surgery [33] and continues to indicate improvements in health-related quality of life over the next 6 to 12 months [34]. The SF-36 is reliable and internally consistent [34-36].
Western ontario and Mcmaster universities osteoarthritis index: The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was used to evaluate self-reported knee-specific impairment [37]. It determines the overall level of disability in a person with OA by assessing pain, joint stiffness, physical, social & emotional function. The WOMAC is a valid, reliable, and responsive self-administered instrument for short-term and long-term follow-up of knee injury, including OA [37].
Dual-energy X-ray absorptiometry: Muscle mass of the surgical leg was estimated using dual-energy X-ray absorptiometry (DXA) as previously described [23] using a DXA-enhanced body analysis (v5.64, Hologic Delphi-W; Waltham, MA) [38]. Non-bone fat-free tissue, which is a good surrogate of extremity muscle mass, was measured for the entire surgical leg as well as a customized region of interest (ROI) for the thigh [39]. For the thigh ROI muscle mass measurements, the proximal border of the ROI was the most proximal aspect of the femoral head and the distal border of the ROI was the lateral joint line. Medial and lateral borders were positioned outside the boundaries of the leg from distal border and extended upward to the proximal border. DXA was performed before TKA, and 4 (previously reported) and 26 weeks after TKA.
Data analysis
Sample size estimates were calculated for our primary outcome measure (quadriceps strength). Twenty-three patients per group were necessary to attain 80% power using quadriceps strength data from a study comparing a medial parapatellar TKA approach (41.4 ± 19.0 N-m) and a less invasive midvastus technique (27.6 ± 12.6 N-m) at 3 weeks [40]. The primary outcome and endpoint for the RCT was difference in quadriceps torque between intervention (MIS) and CONTROL TKA at 4 weeks, which was previously reported. The 26- and 52-week changes from baseline for all outcomes were regressed on sex, age, and baseline values (using intention-to-treat analysis). Baseline characteristics of the treatment groups were previously compared using two-sample t tests for continuous measures or a chi-square test for independent proportions for categorical measures. A two-sided alpha level of 0.05 was designated for statistical significance.
One hundred seventy-five patients scheduled for TKA at the University of Colorado Hospital were assessed for eligibility when they were scheduled for TKA surgery. Forty four patients (22 males, 22 females) aged 50-85 years (64.3 ± 8.4 years) were enrolled in the study (Figure 1). There were no differences between groups in sex, age, height, weight or body mass index (BMI), as previously described [23]. Furthermore, there were no significant group differences in any outcome measure at baseline. At 26 and 52 weeks after TKA, there were no significant differences between groups in quadriceps or hamstrings strength, quadriceps activation, functional performance (SCT, TUG, or 6MW), 6MW knee pain, resting knee pain, AROM (flexion or extension), WOMAC or SF-36 scores (Table 1 and Appendix 1). There were also no differences in muscle mass at 26 weeks after TKA.
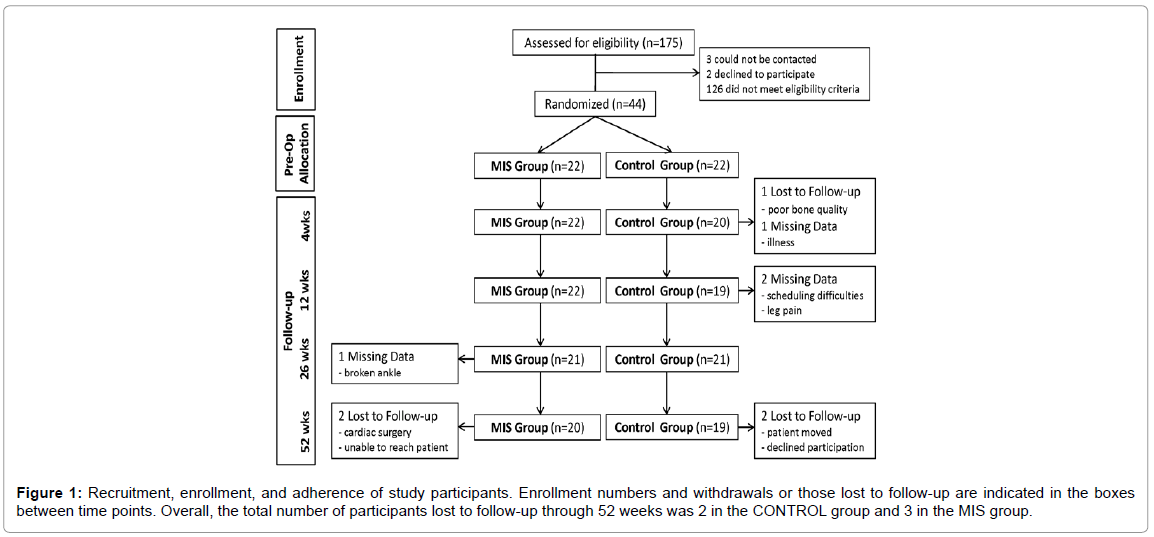
Figure 1: Recruitment, enrollment, and adherence of study participants. Enrollment numbers and withdrawals or those lost to follow-up are indicated in the boxes between time points. Overall, the total number of participants lost to follow-up through 52 weeks was 2 in the CONTROL group and 3 in the MIS group.
| Change from Baseline to 26weeks Mean ± SEb | Difference in the Change from Baseline: MIS - Control (95% CI) | Change from Baseline to 52 weeks Mean ± Seb | Difference in the Change from Baseline: MIS - Control (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | MIS | Control | p value | MIS | Control | p value | ||
| Normalized Quadriceps Strengthc (N-m/kg) | 0.14 ± 0.09 | 0.00 ± 0.10 | 0.14 (-0.13, 0.41) | 0.29 | 0.40 ± 0.10 | 0.26 ± 0.10 | 0.14 (-0.14, 0.43) | 0.32 |
| Normalized Hamstrings Strengthc (N-m/kg) | 0.10 ± 0.04 | 0.01 ± 0.04 | 0.08 (-0.04, 0.21) | 0.17 | 0.13 ± 0.04 | 0.06 ± 0.04 | 0.06 (-0.05, 0.17) | 0.25 |
| Quadriceps Activation (%) | 14.77 ± 2.63 | 10.04 ± 2.81 | 4.73 (-3.07, 12.52) | 0.23 | 15.37 ± 1.69 | 12.36 ± 1.84 | 3.01 (-2.04, 8.06) | 0.23 |
| 6-minute walk (m) | 38.94 ± 12.25 | 41.74 ± 12.76 | -2.80 (-38.7, 33.14) | 0.88 | 60.77 ± 13.57 | 72.97 ± 15.53 | -12.2(-54.5, 30.14) | 0.56 |
| 6-minute walk involved pain (points) | -3.37 ± 0.33 | -3.31 ± 0.33 | -0.06 (-1.02, 0.90) | 0.9 | -3.06 ± 0.47 | -3.38 ± 0.53 | 0.32 (-1.14, 1.78) | 0.66 |
| Stair Climb (sec) | -5.68 ± 1.00 | -3.89 ± 1.01 | -1.79 (-4.67, 1.09) | 0.22 | -6.05 ± 1.00 | -3.94 ± 1.12 | -2.11 (-5.17, 0.95) | 0.17 |
| Timed Up-and-Go (sec) | -1.31 ± 0.35 | -0.75 ± 0.35 | -0.56 (-1.56, 0.45) | 0.27 | -1.65 ± 0.33 | -0.79 ± 0.37 | -0.86 (-1.86, 0.15) | 0.09 |
| Extension Active ROM (deg) | -0.26 ± 1.04 | -0.07 ± 1.05 | -0.19 (-3.22, 2.84) | 0.9 | -2.37 ± 1.09 | -1.71 ± 1.16 | -0.66 (-3.93, 2.61) | 0.68 |
| Flexion Active ROM (deg) | -2.91 ± 1.82 | -3.71 ± 1.84 | 0.80(-4.43, 6.04) | 0.76 | -0.52 ± 2.36 | -2.69 ± 2.48 | 2.17 (-4.69, 9.04) | 0.52 |
| Resting Pain (points) | -1.47 ± 0.23 | -2.01 ± 0.24 | 0.54(-0.14, 1.23) | 0.11 | -1.38 ± 0.33 | -1.64 ± 0.36 | 0.26 (-0.72, 1.24) | 0.59 |
| WOMAC (total score) | -29.4 ± 2.87 | -23.9 ± 2.75 | -5.51(-13.5, 2.51) | 0.17 | -30.3 ± 3.03 | -23.2 ± 3.37 | -7.09 (-16.5, 2.28) | 0.13 |
| SF-36 PCS (points) | 10.74 ± 2.01 | 10.47 ± 2.05 | 0.27 (-5.65, 6.18) | 0.93 | 11.14 ± 2.23 | 10.27 ± 2.75 | 0.87 (-6.47, 8.21) | 0.8 |
| DXA Thigh FFM (g) | 144.1 ± 93.66 | 58.18 ± 94.32 | 85.89 ( -193, 364.7) | 0.53 | NT | NT | NT | NT |
| DXA Leg FFM (g) | 313.5 ± 120.7 | 154.1 ± 121.5 | 159.4 ( -200, 518.8) | 0.37 | NT | NT | NT | NT |
aCI: Confidence Interval, ROM: Range of Motion, WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, SF-36=36-Item Short-Form Health Survey questionnaire, PCS: Physical Component Score, MCS: Mental Component Score, DXA: Dual-Energy X-ray absorptiometry, NT: Not Tested
bValues are ± standard error of the estimate. Negative values reflect a deficit from baseline; positive values reflect an improvement from baseline. P values are from the estimated between-group difference in change from baseline, conditioned on baseline and controlling for age and sex. The model is change from baseline regressed on baseline and treatment assignment.
cNormalized to weight.
Table 1: Mean Changes and 95% Confidence Intervals for the Primary and Secondary Outcome Measures at 26wks and 56wks.
The emergence of MIS TKA surgery has provided a unique opportunity to investigate the impact of surgical trauma on the magnitude of quadriceps dysfunction. Our previously reported early results from this prospective RCT indicated that, by four weeks after TKA, the MIS group had greater improvements than the CONTROL group in hamstrings strength (p=0.02) and a trend towards better quadriceps strength (p=0.07) [23]. However, improvements in muscle strength with MIS did not translate into better functional performance 4 weeks after TKA. Furthermore, there were no clinically meaningful differences in outcomes between groups 12 weeks after TKA. The present results focusing on 26 and 52 weeks after TKA further expand upon our previously reported findings and indicate that there were no long-term differences in muscle strength, knee ROM, or functional performance. Again, early changes in muscle strength did not translate into significant or clinically meaningful differences between groups in outcomes at 26 and 52 weeks after TKA. The inclusion of confidence intervals and mean differences for all outcomes provides additional information for interpretation of these study findings.
Proponents of MIS TKA have suggested that it allows for faster recovery time, greater early post-operative quadriceps strength, shorter hospital stay, less perioperative pain, less need for inpatient rehabilitation, less narcotic usage, less need for assistive devices, better knee flexion during the early post-operative period, and improvements in function [9,12]. Opponents of MIS TKA have raised concerns that limited visualization during surgery could increase complications, such as component malalignment that affects long-term outcomes [9,12] and lengthen the learning curve required for successful implementation of MIS TKA [41].
Recently published, small-scale prospective randomized controlled trials (RCTs) support our current findings and thereby question whether benefits of MIS surgery outweigh the risk of decreased visualization during surgery [9,10,12,19]. A meta-analysis of RCTs examining MIS and conventional TKA surgical approaches reported faster recovery of Knee Society Scores at 6 and 12 weeks with MIS TKA, but found no differences 6 months after surgery [9]. There were no differences between MIS and conventional approaches in short-term overall complications and alignment of femoral and tibial components. However, surgical times were 10-19 minutes longer and wound healing problems and infections occurred more frequently in the MIS group. More recently, another meta-analysis of RCTs focusing on clinical and radiological outcomes found that knee flexion range of motion was significantly greater early after MIS surgery and, with trends for improvements in quadriceps muscle strength, but neither persisted with later follow-up [12]. Therefore, the present study corroborates previous findings that short-term benefits of MIS TKA surgery may not persist long term.
While the findings from this study support those of recent RCTs investigating MIS TKA surgery, this investigation was unique because it included measured functional performance rather than just self-reported perception of functional status. This is important because self-report measures tend to be more closely linked to pain relief than performance measures and, therefore, overstate performance capabilities [21,22]. Furthermore, no prior study had evaluated the impact of MIS TKA on the function of the quadriceps muscle by including muscle activation as a possible mechanism for improved outcomes. Also, few studies used a standardized postoperative rehabilitation program to further decrease variability in outcome measures and no previous studies blinded patients and testers to group assignment by standardizing incision lengths [12].
Importantly, the rate of complications with MIS surgery in the present study was no greater than the CONTROL group, which agrees with some studies [12,19,42] yet other studies have found greater rates of complications with MIS TKA surgery [9,20,43]. We also previously reported that MIS surgery resulted in no greater intra-operative blood loss, tourniquet time or mechanical axis mal-alignment [44], in contrast to the findings of some previous studies [13,20]. The extensive experience of the surgeon performing the MIS TKA surgeries for the present study may have contributed to our lower than expected rates of complications. Therefore, caution is still warranted for surgeons with less experience in TKA MIS techniques, given the potential for greater complications associated with limited visualization during the surgery.
Future investigations should expand upon the findings of this investigation by 1) including larger samples sizes, 2) involving more than 1 surgeon to further validate the findings of this study, and 3) longer follow-up years after surgery to better assess the durability of TKA with MIS surgery. In conclusion, while MIS techniques for TKA may facilitate faster recovery of muscle strength, there is no apparent benefit of MIS on the longer-term recovery of strength or functional performance. Therefore, the benefits of MIS TKA may not outweigh the risks associated with limited surgical visualization during the procedure.
We thank Jaclyn Balter, MS; Ligia Coelho, BA; Jere’ Hamilton, BA; Elizabeth Regan, MD, PhD; Michelle Reynolds, MS; John Kittelson, PhD; Frank Somoza, MA; and physical therapists at the University of Colorado Hospital for their invaluable assistance with this investigation.
This study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (R03AR054538), an Arthritis Foundation New Investigator Award, the National Institute on Aging (T32 AG00279), a Promotion of Doctoral Studies Award from the Foundation for Physical Therapy, a Nutrition and Obesity Research Center grant (P30 DK048520), and a Clinical and Translational Science Award Grant (UL1 RR025780). None of the sponsors had any influence on the study design, implementation, or data analysis and interpretation.