Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2015) Volume 4, Issue 2
Objectives: This study was aimed to analyze cost components and underlying methods of cost-of-illness (COI) studies on alcohol in Japan and overseas by international systematic review, to estimate direct and indirect costs attributable to alcohol in Japan with new data, and to estimate costs impacted by reduced drinking among high-risk drinkers in Japan.
Methods: Relevant publications concerning COI studies on alcohol published during the years 2005-2014 were identified through PubMed and Embase. Google search was conducted to identify relevant studies based on references of other relevant publications. Japanese COI studies on alcohol were identified through Igaku-Chuo-Zasshi (Ichushi) database without limiting the publication year. Cost components and underlying methods were analyzed, and medical costs attributed to alcohol were calculated based on 2012 government data and alcohol-attributed fractions (AAFs), then costs impacted by reduced drinking in Japan were estimated.
Results: Seven eligible studies on 7 countries including Japan met inclusion criteria. All the countries calculated direct and indirect costs associated with alcohol, while only 2 foreign countries further calculated intangible costs. Indirect and intangible costs were 2.5-4 times larger than direct costs in all countries. Medical care costs attributed to alcohol in Japan based on 2012 data and AAFs were 1.5 times higher than 25 years ago. Furthermore, decreased number of high-risk drinkers in Japan in achieving the second term goal of Health Japan 21 was estimated to save 363.1 billion yen per year.
Conclusions: Despite methodological challenges of COI studies, it is still valuable to estimate direct and indirect costs attributable to alcohol in Japan, and related costs possibly saved by reduced drinking highlighted the importance of expanding brief interventions in a clinical setting in Japan.
<Keywords: Cost-of-illness; Methodology; Alcohol; Systematic review; Burden of disease; Reduced drinking
It is widely known that burden of diseases attributable to alcohol is substantial, despite low diagnosis and treatment rates in many countries. Many alcohol dependent and alcohol use disorder patients including undiagnosed ‘high-risk drinkers’ (men: > 60 g/day and women: > 40 g/day according to the definition of World Health Organization) [1] highlight the need for better understanding of economic burdens for health policy-makers in Japan. COI studies provide information on specific cost impacts, often serving as a health economic evidence for decision-making and planning of various health care services. However, lack of standard methodologies for COI studies make it difficult to conduct robust estimation of economic burdens associated with high-risk drinking in many countries. Thus, this study was aimed to analyze cost components and underlying methods of COI studies on alcohol in Japan and overseas by international systematic review, to estimate direct and indirect costs attributable to alcohol in Japan with new data, and to estimate costs impacted by reduced drinking among high-risk drinkers in Japan.
A systematic literature review was conducted in October, 2014 by searching major electronic databases PubMed and Embase to identify relevant publications in English between the years 2005-2014 (past 10 years) concerning the COI studies on alcohol. The literature searches were conducted by combining the following terms: “cost-of-illness” and “alcohol”. First, the titles and abstracts of the potentially relevant publications were assessed, and publications irrelevant to COI studies on alcohol were excluded. Then, COI studies focused on developing countries, or not written in English were excluded. Review articles were also excluded but eligible COI studies or relevant government reports were further identified by checking references of such review articles via Google search. Likewise, COI studies on alcohol in Japan were identified from the widely recognized Japanese electronic Ichushi database with the equivalent key words in Japanese. Since few eligible publications were expected, the year of publication was not limited in Ichushi. The search and retrieval process for the literature review is described in Figure 1.
Each eligible study identified from the systematic review was reviewed and summary tables were created to facilitate comparative analysis of the cost components included in the COI studies as well as total estimated costs of alcohol-attributable diseases and proportions of direct and indirect costs in Japan and other developed countries. Moreover, alcohol-attributable medical care costs were calculated based on the latest available Japanese government’s statistical data on medical expenses in 2012 (adjusted by disease categories, age groups, and gender) and also by using AAFs for Japan for some disease groups associated with alcohol consumption.
In order to estimate costs impacted by reduced drinking, the number of high-risk drinkers in Japan who need to reduce volume and/or frequency of alcohol consumption was calculated in the ideal scenario of achieving the second term goal of national health promotion campaign called Health Japan 21 [2], based on the latest available Japanese population data (as of Oct 1, 2012) adjusted by age groups and gender [3]. Then, additional costs incurred for additional clinical practices, i.e., costs associated with brief interventions, were estimated based on the data from a representative alcohol treatment facility in Japan. Then, annual costs likely to be impacted by reduced drinking were calculated by subtracting the newly incurred brief intervention costs from the total costs possibly saved by decreased direct and indirect costs associated with alcohol. Finally, decreased tax revenue from reduced alcohol purchase was calculated based on the 2012 government data on tax revenue [4], and it was included in the estimation of costs impacted by reduced drinking.
The systematic review resulted in final retrieval of 7 original COI studies on alcohol from 7 developed countries/legal entities (Japan, US, Portugal, Sweden, Scotland, England, Ireland) out of 572 potentially relevant studies from PubMed and Embase and 5 potentially relevant studies from Ichushi as shown in Figure 1. Irrelevant COI studies on alcohol were excluded. Then, 3 studies focused on developing countries (Estonia, South Africa, and Thailand) were excluded, given the secondary purpose of the study. Furthermore, 1 article written in Spanish except for abstract and 3 review articles were excluded, although the study by Thavorncharoensap et al. [5] provided a very good overview of international comparison.
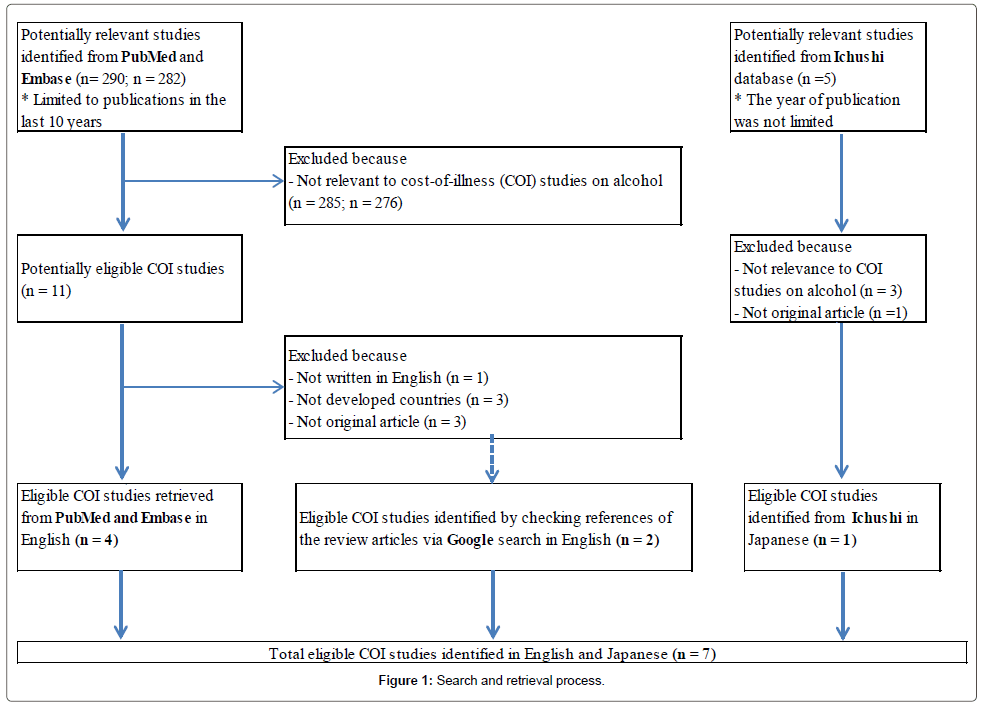
Figure 1: Search and retrieval process.
Regarding the eligible COI studies on alcohol in Japan, only one article published in 1993 by Nakamura et al. [6] was identified, in which the cost estimation was based on 1987 data. There was another relevant Japanese study reported in 2012 based on the 2008 national survey data, but the information existed only as a conference proceeding and detailed description of the methodology was not available, thus it was excluded. Actually, the cost estimation based on the 2008 national survey data was also reported in a section of White Paper on Alcohol [7], but the methodology was based on the study conducted by Nakamura et al. [6], thus it was considered as a reference.
Table 1 provides an overview of the cost components included in the COI studies on alcohol in the 7 countries. All countries estimated the direct costs (outpatient and inpatient care including drug/service costs and hospitalization, property damage due to criminal justice, motor vehicle crashes due to drunken driving) and indirect costs (productivity loss due to premature mortality, presenteeism or “days at work but limited in performing job tasks because of health”), but cost estimation on absenteeism or “days of work missed because of illness” [8] was unknown in Japan. More than 4 countries included following direct costs (research and prevention, nursing homes, fire losses, welfare assistance/social work) and indirect costs (productivity loss due to early retirement). Only US included cost items on Fetal Alcohol Syndrome (FAS).
| Cost Components | Japan (Nakamura, 1993) |
US (Bouchery, 2011) |
Portugal (Cortez-Pinto, 2010) |
Sweden (Jarl, 2008) |
Scotland (Johnston, 2012) |
England (Dept of Health, 2008) |
Ireland (Byrne, 2010) |
|
|---|---|---|---|---|---|---|---|---|
| Direct costs | Health care costs/outpatient care costs | ○ | ○ | ○ | ○ | ○ | ○ | ○ |
| Hospitalization/inpatient care costs | ○ | ○ only primary diagnosis-related |
○ | ○ | ○ | ○ | ○ | |
| Ambulatory care costs | unknown | ○ only primary diagnosis-related |
○ | unknown | ○ | ○ | ○ | |
| Fetal alcohol syndrome (FAS) | × | ○ | × | × | unknown | × | × | |
| Health insurance administration costs | ○ | ○ | unknown | unknown | unknown | unknown | unknown | |
| Drugs/services | ○ | ○ | ○ | ○ | ○ | ○ Drug dispensing costs are not included |
○ | |
| Research and prevention costs | ○ | ○ | × | ○ | ○ | ○ | × | |
| Nursing homes | ○ | ○ | unknown | unknown | ○ | ○ | unknown | |
| Crime victims | unknown | ○ | ○ (Thavorncharonsap, 2009) |
○ | unknown | ○ | ○ | |
| Property damage due to criminal justice | ○ | ○ | ○ | ○ | ○ | ○ | ○ | |
| Motor vehicle crashes due to drunken driving | ○ | ○ | ○ | ○ | ○ | ○ | ○ | |
| Fire losses | ○ | ○ | unknown | ○ | unknown | ○ | unknown | |
| Crime victim property damage | unknown | ○ | ○ | ○ | × | ○ | ○ | |
| Special education costs on FAS | × | ○ | × | × | unknown | × | × | |
| Welfare assistance/social work | ○ | unknown | ○ | ○ | ○ | × | ○ | |
| Indirect costs | Productivity loss due to premature mortality | ○ | ○ Underage drinking and productivity loss at home are included |
○ | ○ | ○ | ○ | ○ Suicide related to alcohol are included |
| Presenteeism (reduced on-the-job productivity) | ○ | ○ | ○ | ○ | ○ | ○ | ○ | |
| Absenteeism (being absent from work) | unknown | ○ | ○ | ○ | ○ | ○ | ○ | |
| Productivity loss due to early retirement | ○ | × | ○ | ○ | ○ | ○ | ○ | |
| Lost day due to crime victims and incarceration | × | ○ | ○ | ○ | unknown | ○ | unknown | |
| Fetal alcohol syndrome (FAS) | × | ○ | × | × | unknown | unknown | unknown | |
| Intangible costs | QOL losses from alcohol consumption (pain, suffering, distress, loss of life/bereavement) | × Due to methodological limitation |
× Due to methodological limitation |
× Due to methodological limitation |
○ Alcohol consumers, their relatives and friends, and crime victims are considered |
× Despite mentioning importance |
○ Only high-risk drinkers are considered (counseling fees are calculated by Willingness-to-pay approach) |
× Due to methodological limitation |
Table 1: Cost components included in the COI studies.
Sweden and England had an additional cost category called “intangible costs.” According to the study which estimated economic and human costs in Sweden in 2002 [9], intangible costs refer to Quality of Life (QOL) losses from alcohol consumption (pain, suffering, distress, loss of life/bereavement), and there is no appropriate methodology existing and this approach is seldom used in the COI analysis. In England, Department of Health [10] also calculated intangible costs related to alcohol, but it was limited to the costs of high-risk drinkers (more than 3-4 units of alcohol for men and 2-3 units for women per day, when one unit is equal to 10 ml of pure alcohol), thus it was not possible to compare with the case of Sweden, where QOL losses of relatives, friends, and crime victims were also estimated. Other countries mentioned methodological limitation for not calculating intangible costs.
The costs related to crime victims, crime victim property damage, and lost day due to incarceration were not calculated in Japan due to limited data, while they were calculated in the US [11], Portugal [12], Sweden [9], England [10], and Ireland [13]. Table 2 shows total estimated COI on alcohol and proportions of direct and indirect costs in 5 selected countries (Japan, US, Sweden, England, and Ireland). Portugal [12] and Scotland [14] were excluded from the comparative analysis because health care and hospitalization costs (sum of outpatient and inpatient care costs) did not account for the largest share of direct costs, which was different from Japan.
| Total estimated costs and proportions | Japan (Nakamura, 1993) |
US (Bouchery, 2011) |
Sweden (Jarl, 2008) |
England (Dept of Health, 2008) |
Note: England (Cabinet Office, 2003) |
Ireland (Byrne, 2010) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| billion ¥ | % | million $ | % | million SEK | % | % | million £ | % | % | million £ | % | |||
| Direct costs | health care costs/outpatient care costs | 1,174.2 | 19.6 |
10,668 | 28.9 | 1,540 | 37.5 |
6.3 | 167.6 | 14.0 |
38.0 | 1,200 | 83.1 | |
| hospitalization/inpatient care costs | Included in health care costs | 5,116 | 1,680 | Included in health care costs | Included in health care costs | |||||||||
| ambulatory care costs | NA | 1,196 | NA | Included in health care costs | Included in health care costs | |||||||||
| fetal alcohol syndrome (FAS) | NA | 2,054 | NA | NA | NA | |||||||||
| Health insurance administration costs | 88.6 | 1,586 | NA | NA | NA | |||||||||
| Drugs/services | Included in health care costs | 1,212 | 75 | Included in health care costs | Included in health care costs | |||||||||
| Research and prevention costs | Included in insurance administration costs | 1,207 | 479 | Included in health care costs | NA | |||||||||
| Nursing homes | Included in health care costs | 1,003 | NA | Included in health care costs | NA | |||||||||
| Crime victims | NA | NA | 2,850 | NA | 3 | |||||||||
| property damage due to criminal justice | 0.2 | 20,973 | Included in crime victims costs | Included in health care costs | 435 | |||||||||
| motor vehicle crashes due to drunken driving | 3.5 | 13,718 | Included in crime victims costs | Included in health care costs | 526 | |||||||||
| fire losses | 8.9 | 2,137 | Included in crime victims costs | Included in health care costs | NA | |||||||||
| crime victim property damage | NA | 440 | Included in crime victims costs | Included in health care costs | 171 | |||||||||
| special education costs on FAS | NA | 369 | NA | NA | NA | |||||||||
| welfare assistance/social work | 23.5 | NA | 4,364 | Included in health care costs | 264 | |||||||||
| Indirect costs | productivity loss due to premature mortality | 923.1 | 80.4 |
65,062 | 71.1 | 8,520 | 62.5 |
10.5 | 1,023 | 86.0 |
37.0 |
277 (including suicide) | 16.9 | |
| presenteeism (reduced on-the-job productivity) | 4,257.3 | 74,102 | 1,175 | Included above | 197 | |||||||||
| absenteeism (being absent from work) | NA | 4,238 | 4,908 | Included above | 330 | |||||||||
| productivity loss due to early retirement | 158.3 | NA | 3,177 | Included above | Included in presenteeism | |||||||||
| lost day due to crime victims and incarceration | NA | 6,329 | 614 | NA | NA | |||||||||
| fetal alcohol syndrome (FAS) | NA | 2,054 | NA | NA | NA | |||||||||
| Intangible costs | QOL losses from alcohol consumption (pain, suffering, distress, loss of life/bereavement) |
NA | NA | NA | NA | 145,356 (lost QALY) |
NA | 83.2 | Unknown (referred to Cabinet Office report) |
NA | 25.0 | NA | NA | |
Table 2: Costs and proportions.
According to Nakamura et al. [6], the total costs of inappropriate drinking in Japan were approximately 6.6 trillion yen (sum of direct costs of 1,298.9 billion and indirect costs of 5,338.7 billion yen). The proportions of direct and indirect costs in Japan were 19.6% and 80.4%, respectively, while those in other countries ranged widely from 14.0% to 83.1% for direct costs and from 16.9% to 86.0% for indirect costs. England had the lowest proportion of direct costs (14%); however, when the intangible cost (25%) was included, the proportions of direct and indirect costs were equivalent (38% and 37%, respectively). In Sweden, intangible costs accounted for as much as 83.2% of total estimated costs, lowering the proportions of both direct and indirect costs to one sixth compared to the pre-inclusion. According to the global burden of disease study attributable to alcohol [15], the top 3 diseases associated with high-risk drinking in Japan were cancer, followed by unintentional and intentional injuries and liver cirrhosis. Moreover, the AAFs for Japan were following: cancer (11% in men, 6% in women), unintentional and intentional injuries (18% in men, 13% in women), liver cirrhosis (70% in men, 68% in women), neuropsychiatric disorders (4% in men, 2% in women), cardiovascular diseases (4% in men, 0% in women), where 0% indicates fewer than 500 alcohol-attributable DALYs in the disease category. Gatjahr et al. [16] describes that alcohol-related negative health consequences are categorized into chronic conditions such as cancer and liver cirrhosis and acute conditions such as injuries and suicide. AAFs for chronic conditions are usually determined by combining relative risks (RRs) and prevalence data at different alcohol consumption levels, and AAFs for acute conditions are usually determined by including the cases happened under the influence of alcohol at the time of the event. Table 3 shows calculation of alcohol-attributable medical treatment costs in Japan, based on electronic statistical data released on Oct 8, 2014 by Japan’s Ministry of Health, Labour and Welfare (MHLW) and Statistics Bureau of the Ministry of Internal Affairs and Communications [17], and 2012 national medical expenditure data by diagnostic disease category (adjusted by hospitalization status, age groups and gender). AAFs for Japan were used and the results were compared with those by Nakamura et al. [6]. In the study by Nakamura et al. [6], the national medical expenditures in 1987 were calculated by multiplying the ratios of alcohol-attributable service utilization rates by different diagnostic disease categories. The service utilization ratios were estimated with the number of inpatients, average hospitalization length, and alcoholattributable morbidity percentage based on ICD-9 (the 9th International Classification of Disease) codes. Thus, the main difference from the previous study [6] is the use of AAFs for Japan obtained from the Comparative Risk Assessment of the Global Burden of Disease study for 2002 for chronic disease categories [15], except for AAFs for digestive disorders. Since AAFs for liver cirrhosis in England (78% in men and 52% in women) were comparable to those in Japan (70% in men, 69% in women), it was considered reasonable to estimate AAFs for digestive disorders in Japan (52% in men and 37% in women) by calculating the average AAFs of following 3 relevant disease categories in England and then rounding the numbers off to the nearest integer values: acute and chronic pancreatitis (30% in men, 13% in women), gastro-oesophageal laceration-haemorrhage syndrome (47% in men and women), and oesophageal varices (78% in men, 52% in women) for all ages above 16 years old [10].
| AFFs for Japan (Rehm, 2009 [15]) |
Medical costs in Japanin 2012 (billion¥) (Gov’t stats Table15, 2014) |
AAFs-multiplied medical costs in Japan in 2012 (billion¥) | |||||
|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | Total | |
| Cancer | 11% | 6% | 2051.3 | 1714.3 | 225.64 | 102.86 | 328.50 |
| Neuropsychiatric disorders | 4% | 2% | 885.8 | 967.7 | 35.43 | 19.35 | 54.79 |
| Cardiovascular disorders | 4% | NA | 1003.5 | 719.8 | 40.14 | NA | 40.14 |
| Cirrhosis of the liver | 70% | 68% | 94.7 | 77 | 66.29 | 52.36 | 118.65 |
| Digestive disorders (% assumed) | 52% | 37% | 849.9 | 775.6 | 441.95 | 286.97 | 728.92 |
Table 3a: Medical care costs with AAFs.
AAFs for cancer and cardiovascular disorders in Japanese men in 2012 were much higher than the corresponding alcohol-attributable service utilization rates used 25 years ago [6]. This is not so surprising given the fact that 2012 medical costs for treating cancer (disease category name: Neoplasm) and cardiovascular disorders (disease category name: Diseases of the circulatory system) were 3.2 and 1.5 times higher, respectively. When alcohol-attributable medical care costs were calculated based on the 2012 data using the same alcoholattributable service utilization rates of 1987, the total amount was 1,545 billion yen, and when AAFs-multiplied medical costs based on 2012 data were used for the 4 disease categories that were available, the total amount was 1816.5 billion yen as shown in Table 3. Given Japan’s total national medical care expenses of approximately 39.2 trillion yen in 2012, these alcohol-attributable treatment costs accounted for 3.9-4.6% of the total expenses.
| Nakamura et al. (1987 data) [6] | Gov’t Stats (2012 data) Table 13 |
Gov’t stats (2012 data) Table 15 and AAFs |
||||
|---|---|---|---|---|---|---|
| Disease Category | Total medical costs (billion ¥) (above 15 years old) |
Alcohol-attributable service utilization rate (%) * | Alcohol-attributable medical costs (billion ¥) |
Total medical costs (billion ¥) (above 15 years old) |
Alcohol-attributable medical costs (billion ¥) When the same serviceutilization rate* was used |
Alcohol-attributable medical costs (billion ¥) When AAFs-multiplied medical costs were combined |
| Infectious and parasitic diseases | 456 | 16.38 | 74.7 | 557 | 91.2 | 91.2 |
| Neoplasm | 1,174 | 6.30 | 74.0 | 3,766 | 237.3 | 328.50 |
| Mental disorders | 1,114 | 4.78 | 53.2 | 1,853 | 88.5 | 54.79 |
| Diseases of the circulatory system | 3,780 | 0.04 | 1.6 | 5,780 | 2.4 | 40.14 |
| Diseases of the digestive system | 1,881 | 34.00 | 639.5 | 1,626 | 552.6 | 728.92 |
| Diseases of the nervous system | 978 | 1.76 | 17.2 | 1,183 | 20.8 | 20.8 |
| Endocrine, nutritional and metabolic diseases | 669 | 18.89 | 126.4 | 1,942 | 366.8 | 366.8 |
| External causes of injury and poisoning | 1,091 | 10.00 | 109.1 | 1,853 | 185.3 | 185.3 |
| (Other disease categories) | 4,673 | Included in total | NA | |||
| Total | 15,816 | 1095.7 | 18,558 | 1,545.0 | 1,816.5 | |
Table 3b: Medical care costs with AAFs.
Estimation of high-risk drinkers and costs impacted by reduced drinking in Japan
According to the national survey conducted in 4,153 adults in Japan (response rate of 58%) based on 2012 population data [18], a life-time prevalence of alcohol dependence was 2.1% (950,000) for men and 0.2% (140,000) for women, totaling 1.09 million. When more than 20 points in the Alcohol Use Disorders Identification Test (AUDIT) screening are considered as probable alcohol dependence and more than 16 points as potential alcohol dependence, 1.13 million probable and 2.63 million potential alcohol dependent persons are assumed to exist in Japan.
Although a traditional treatment goal of alcohol dependence in Japan has been abstinence alone, an early intervention of reduced drinking as a mid-term treatment goal for some patients (such as diagnosed alcohol dependent patients who have difficulty in maintaining abstinence or undiagnosed high-risk drinkers) has also been discussed among both alcohol specialists and non-specialists [19], because of ‘health gain’ or decreased mortality rate [20], particularly among high-risk drinkers (men: >60 g/day and women: >40 g/day).
In 2000, the MHLW initiated a 10-year health promotion campaign (the first term) under the Health Japan 21 to prevent premature death from non-communicable diseases and injuries. Decreasing the number of high-risk drinkers who have high potential of developing life-style related diseases (men: >40 grams/day and women: >20 grams/day) was included in the objectives, but it was not so successful. Thus, the Japanese government has continuously set a goal in 2010 (the second term) to reduce a proportion of high-risk drinkers from current 15.3% to 13% in men, and from current 7.5% to 6.4% in women by 2022. To achieve this goal, approximately 3.05 million adults aged 20 or older need to reduce their alcohol consumption over 12 years from 2010, based on 2010 Japanese population. This means that approximately 0.2% or 254,210 adults per year need to receive brief interventions, which is “10 to 15 minutes of counseling, with feedback about drinking, advice and goal setting, and follow-up contact (one or more discussions lasting 10 to 15 minutes with a clinician)” [21]. Since brief interventions are known to be successful in half of the patients according to the case of Kurihama Medical and Addiction Center [22], it is considered that 508,420 adults per year would need to receive such brief interventions.
Miyakawa et al. provides medical costs on alcohol treatment in Japan by following 4 categories: 1) one routine examination (visit by abnormal value found in the annual health examination), 2) preventive treatment as an outpatient for education and testing (group psychotherapy plus 5 examinations), 3) normal outpatient treatment after discharged from the hospital, and 4) hospitalization of alcohol dependent patients for 3 months [23]. The costs associated with introducing brief interventions to high-risk drinkers in Japan are related to 1) and 2), because patients for 3) and 4) are usually instructed to keep abstinence and avoid binge drinking. Assuming that one person needs to visit a medical institution 2 times for 1) and 6 times for 2), the total costs (100% costs, not out-of-pocket payment amount) per person per year will be 9,360 yen for 1) and 51,750 yen for 2). Also assuming that 254,210 adults (50%) undergo type 1) and another 254,210 adults (50%) undergo type 2) interventions, annual costs for conducting brief interventions to 508,420 adults in Japan become approximately 15.5 billion yen per year, considering the optimistic 50% success rate.
Rehm and Roerecke found a reduction of 20 grams of pure alcohol intake per day in heavy drinkers, who consume more than 48 grams of pure alcohol per day, lowered yearly mortality risk to approximately 1% in Europe [20]. Thus, it was assumed that successful reduction of 20 grams of pure alcohol in 254,210 high-risk drinkers per year would save the lives of 2,542 people in Japan. Considering the case of 40-yearold Japanese man (university graduate) with an annual salary of 6 million yen according to 2012 Basic Survey on Wage Structure [24], preventing potential loss of 25 more years of employment could save 0.15 billion yen per person or 381.3 billion yen per year. Moreover, given that the national tax revenue from selling alcohol in 2012 was approximately 1.35 trillion yen [4], if the 0.2% of high-risk drinkers refrained from buying alcohol, the decreased tax revenue was estimated at approximately 2.7 billion yen. Thus, a successful reduction of highrisk drinkers in line with the second term goal of Health Japan 21 on alcohol would save at least 363.1 billion yen per year, after subtracting 15.5 billion and 2.7 billion yen.
Major cost components included in the observed COI studies were medical treatment and drug costs, premature mortality costs, absenteeism, and presenteeism due to inappropriate consumption of alcohol. This is in line with the study which estimated costs of alcohol in Canada in 2002; “indirect costs or productivity losses were the largest cost category (61%), followed by health care (22%) and law enforcement costs (14%)” [25]. In addition to these direct and indirect costs, England and Sweden also included intangible costs, thus a great variation was seen in the proportions of direct, indirect, and intangible costs. In Japan, direct and indirect cost proportions were 20% and 80%, based on 1987 data. The calculation with 2012 data in this study suggested approximately 1.5 times higher direct costs related to alcohol in Japan. This was understandable given the increased Japanese population who suffer from diseases attributable to alcohol over the past 25 years. Although the indirect costs could not be estimated with new data, if the same proportions of direct and indirect costs are applied, the total costs of alcohol abuse in Japan are estimated to be approximately 9.9 trillion yen.
In this study, AAFs for major diseases attributable to alcohol in Japanese population were newly applied to estimate the associated medical costs, and AAFs for digestive disorders for Japan were estimated based on the AAFs in England. If genetic variations in alcohol metabolism were considered, the estimated AAFs for Japan may have been somewhat underestimated. Moreover, given that AAFs are expected to change each year based on the actual level of drinking, some overestimation or underestimation is noted. The calculation of indirect costs in Japan, like other countries, often faces methodological challenges due to limited data. This is not unique to the study on alcohol. For example, a recent study which estimated the costs of schizophrenia in Japan states “no reliable data in Japan are available with regard to absenteeism, presenteeism, treatment-related time off work, unwanted job changes, loss of opportunities for promotion and education, and loss of unpaid production while ill” [26], thus the study included only unemployment costs in the morbidity costs. For the quality improvement of future COI studies in Japan, a use of health-related QOL scales such as widely used WPAI-GH (Work Productivity and Activity Impairment Questionnaire: General Health) is recommended.
Regarding the calculation of productivity loss due to premature mortality, a scenario of 40 year-old Japanese man who works until he reaches the retirement age of 65 years old was used. In a case of 40-yearold Japanese woman, the amount is considered approximately 20% lower. Furthermore, the calculation did not consider an unemployment rate nor incremental increase of salary over the period; thus, both overestimation and underestimation are considered to some extent.
In the comparative analysis of COI among 7 countries, costs as percent GDP adjusted by purchasing power parity (PPP) were not calculated because the amount itself was not the main focus of this study, though the study which reviewed cost drivers associated with alcohol abuse, heavy drinking, and alcohol dependence in high-income countries reported that “the cost due to heavy drinking and/or alcohol dependence as percent GDP (PPP) was estimated to be 0.96%” [27]. Similarly, a discount rate of 2% recommended in a cost-effectiveness or long-term analysis according to the “Guideline for economic evaluation of healthcare technologies in Japan” was not applied [28]. Moreover, morbidity costs and unrelated medical and non-medical costs impacted by reduced drinking were not estimated. If the morbidity costs impacted by reduced drinking had been estimated, the total amount possibly saved would have been greater, thus the estimation of morbidity costs based on a Markov model may be interesting for the future research. There are general limitations in the COI studies on alcohol. As described in the International guidelines for estimating the costs of substance abuse [29], even if the patients successfully reduced drinking, “there would still be morbidity and mortality effects from the physiological damage of” past drinking, due to time lag between the change of drinking behaviors and its clinical outcomes. The difficulty is that the length of time-lag often varies, depending on the types of diseases attributable to alcohol. Another limitation is causality. It is almost impossible to determine whether or not a person lost job or work productivity truly due to alcohol. The same is true for a crime or car accident. A person may have committed a crime anyway regardless of alcohol consumption, or a person may have caused a car accident due to concomitant diseases not associated with alcohol or due to adverse drug reactions or illegal drug use. Despite these limitations often seen, it is still worth estimating related costs with available data than doing nothing, as also described in the international guidelines for the estimation of the avoidable costs of substance abuse by Collins et al. [30], because it will provide some evidence for making better decisions on healthcare budget and resource use.
The overall methodologies of COI studies on alcohol in Japan were similar to those in the other developed countries, but proportions of direct costs varied greatly from 14% to 83.1%, when intangible costs were not considered. In Japan, direct medical costs based on 2012 government statistical data were estimated as 1.8 trillion yen. Regarding the indirect costs estimation, further collection of data on work productivity by using reliable QOL scales was considered important in Japan. In addition, it was considered that data on car accidents, injuries, and crimes attributable to alcohol would require more realistic estimation, given causality. Despite the methodological challenges due to limited data, an updated estimation of costs attributable to alcohol in Japan in this study was considered valuable for both clinicians and health policy-makers in Japan.
Furthermore, the estimation of costs impacted, or possibly saved by promoting reduced drinking to high-risk drinkers suggested significantly decreased medical care and social costs in Japan. It was estimated that achieving the second term goal of Health Japan 21 (a reduction of 1.7% male and 1.2% female high-risk drinkers in Japan by 2022) would save 363.1 billion yen per year, despite additional costs for conducting brief interventions as well as decreased tax revenue from purchasing alcohol beverages. Therefore, this study highlighted the importance of further expanding brief interventions to high-risk drinkers in a clinical setting in Japan.
The author thanks Professor Shunya Ikeda and Professor Masaki Muto at International University of Health and Welfare for providing useful advice in the study planning and preparation of the article.