Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2014) Volume 3, Issue 4
Aim: To develop a decision support technology that can be used by the primary health care providers to take appropriate decisions while rendering health services to Mothers in antenatal Period, Mothers in Postnatal Period, Children below the age of 5 years.
Materials and Methods: “Integrated Management of Childhood and Neonatal Illness” was chosen for prototyping for implementation as it was readily available. The developed software prototype was given to the protocol development unit and field trial unit for the initial feedback. We tested our decision support system (DSS) for maternal and childcare in two phases. The first phase involved live testing of the DSS in the urban hospital and in second phase it was given to Village Health workers (VHWs) in two rural Primary Health Centers.
Result: We achieved nearly nil mismatches in the 0-2 months category and maternal care. The software for 2months-5years category found some mismatch in diagnosis. Apart from “acute severe malnutrition”; other disease classification found Kappa value to be above 0.9
Conclusion: Village Health worker together with clinical Decision Support System as one unit perform almost as good as a clinician in primary health care. The Decision Support System model may prove to be a highly replicable model.
<In much of the developing world, access to quality health care is limited and people depend on providers who have limited training or supervision [1]. Globally, rural population is served by only 38% of the total nursing workforce and by less than a quarter of the total physician work force [2,3]. Access to well-trained and motivated health workers is critical to achieve Millennium Development Goals [4]. Further, evidence suggests that overburden health workers are overwhelmed [5,6] and almost one fourth of time of primary care health workers was spent in non-clinical work (including documentation) in Jordan and West Bengal, India [7].
It is possible that the burdened work force may have an impact on the quality of delivery of health services. In fact, evidence from West Bengal suggests that excessive documentation led to lower DPT booster coverage [8].
Computers and software technology have been demonstrated to improve both quality and quantity of services delivered at the primary care level. However, we have limited data to indicate how the reduced time for documentation can help in improving the functioning of the female health workers in delivering the primary health care services [9].
The increasing availability of low-cost computer technology has the potential to improve health care decisions for individuals and populations. Evaluation of new technologies can be difficult, often requiring a multi-disciplinary approach [10], and are rarely tested in resource-poor environments. In developed countries, decision support technologies have consistently been shown to have a positive impact on both the process of health care and patient outcomes [11]. The few studies from developing countries have shown that they are safe and potentially useful [12].
Since most of the primary health services are oriented towards improving maternal and child health, we proposed to develop a decision support technology and test its feasibility in improving the quality of delivery of maternal and child health services at the primary health care level. This was done by providing it to the female health workers in the form of a gadget with software to aid them in decisionmaking and documentation.
Our primary objective was to develop a decision support technology that can be used by the primary health care providers to take appropriate decisions while rendering health services to
• Mothers in antenatal Period
• Mothers in Postnatal Period
• Children below the age of 5 years
The permission from head of institution and clearance from Institutional Ethics Committee were obtained. The study was carried out from March to December 2010.
Product development strategy
The main challenge faced by the team was to create effective communication channel to successfully handle multi-disciplinary nature of the project. Three units were constituted as follows
• Protocol development unit
• Technological development unit
• Field trial unit
“IMNCI protocol for 0-2 months” was chosen for prototyping for implementation as it was readily available and minimum guidance was required from the advisory committee. The developed software prototype was given to the protocol development unit and field trial unit for the initial feedback. Once the general requirements were gathered, a detailed analysis of scope of the development was laid out for the review of core committee.
It was found out the maternal care protocol development involved more layers complexities as its international standard protocol is not available and required 2 months for protocol development.
Protocol development
We studied various work done worldwide related to decision support system focused on maternal and child health.
For children upto 5years of age, Integrated Management of childhood Illness (IMCI) [13,14] protocol, is taken as gold standard worldwide. Integrated Management of Childhood Illness is a systematic approach to children’s health which focuses on the whole child. It focuses on both curative care (case management and health system support) and prevention of disease (with improved community practices). Case management includes medical algorithms to inspect a simple set of signs and symptoms for diarrhoea, fever, cough, measles and ear ache. The investigation for child with diarrhoea includes assessing for presence of blood in stool, restlessness, sunken eye, whether eager to drink water and noting down the time taken after pinching a fold of skin over abdomen. Flow charts describe how to use the result of the signs and symptoms to classify the illness and give suitabletreatment according to age and weight. Classifications are categorized as Pink (Danger sign which needs referral to higher facility center), Yellow (Outpatient Health Facility) and Green (Appropriate Home Management). This health system support, guides the Village Health Worker to assess the child for malnutrition and intervention required for underweight children. There are many protocols and calculations to be kept in the mind of health worker when providing care. With our decision support protocol, we have tried to reduce the burden of memorization of protocol and calculation, rather shifting focus on eliciting the symptoms correctly. An example for the same is described below taking diarrhoea question set for 2m-5yr. Protocol for identification and management of diarrhoea is shown in Figure 1.
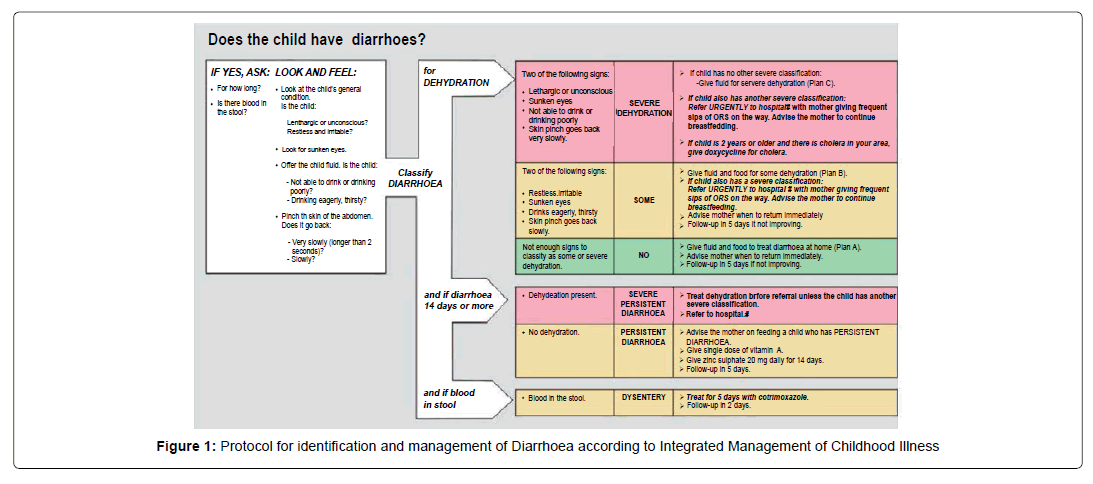
Figure 1: Protocol for identification and management of Diarrhoea according to Integrated Management of Childhood Illness
First the questions are asked to list down the symptoms / complaints. Depending on the answers of questions a tree based structure is devised to further investigate a particular complaint. In this example when a complaint of diarrhoea is registered the following questions are asked one after the other. Details of the questions to be asked for a child 2 month-5 year is shown in Figure 2.
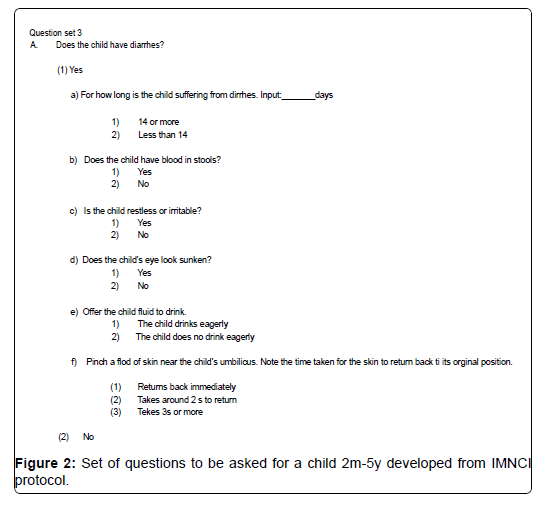
Figure 2: Set of questions to be asked for a child 2m-5y developed from IMNCI protocol.
The same questions were translated to Tamil and typed using “Google transliteration” for avoiding Unicode formatting issue, which is commonly encountered in case of custom fonts like Baamini, Latha etc. Detail process of translation of question in to local languages is shown in Figure 3.
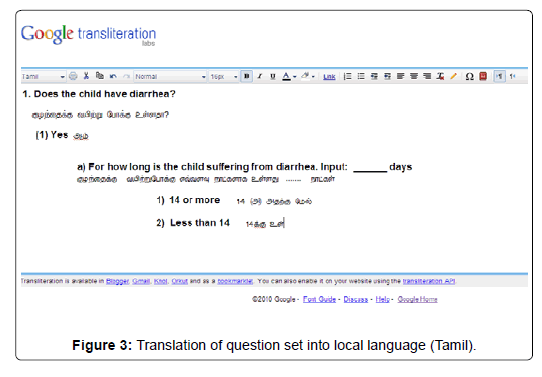
Figure 3: Translation of question set into local language (Tamil).
Then depending on the signs and symptoms entered; a logic based tableusing ‘AND’, ‘OR’ and ‘NOT’ is made to arrive at the diagnosis. Each diagnosis is classified into green, yellow and pink depending on the level of priority required for intervention. The logic used for arriving at the classification of dehydration is shown in Figure 4. Our developed decision support for child care management includes
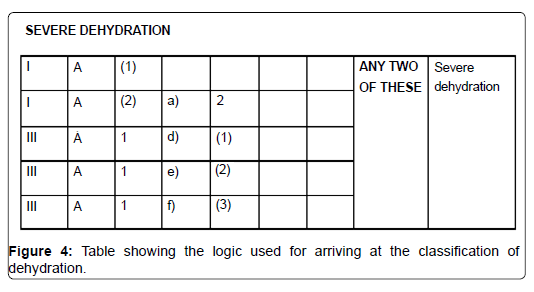
Figure 4: Table showing the logic used for arriving at the classification of dehydration.
1.Case management for first visits (not follow up visit)
2.For both 0-2 months and 2mo-5year
3.Assessment for malnutrition using age-weight chart
4.Breast feeding instructions
Maternal care protocol was developed on the similar logic as described above in the childcare. We developed it using the references of following materials.
1. Antenatal, intranatal, postnatal care protocol for VHN, National rural health mission.
2. Guidelines for pregnancy care and management of common obstetric complications by medical officers, Ministry of Health and Family Welfare (MoHFW)
3. Guidelines for gestational diabetes mellitus, MoHFW
4. Integrated management of pregnancy and childbirth. Pregnancy, childbirth, postpartum and new born care: World Health Organization (WHO).
We colour coded the risk classifications as pink, yellow and green for easy guidance for Village health worker. Apart from risk classification protocol was suitably designed for tracking of the mother throughout the pregnancy period in different trimesters. Once the registration was made, the parameters such as blood pressure, weight, Oral Glucose Tolerance Test, Expected date of delivery etc. were stored and in the follow-up visits suitablealerts or classification, if any is made by assessing the change of the above parameters.
Pretesting the protocol
IMNCI protocol was converted into a “tree model” of questions and answers session suitablefor software implementation. After initial rapid prototyping for hardware and a small part of software, we developed a comprehensive decision support system for both maternal care and childcare.
Quality checking was done in two steps. First, it was made sure the software developed is according the protocol given to technical team and this was done by protocol development team in collaboration with technical team in mechanical fashion. In the second step, the decision system software was tested in the outpatient (OP) department of Stanley medical college, Chennai. The process was handled by a team, who were not involved in protocol development to minimize the experimenter’s bias in quality checking. Each case of maternal health and childcare were interviewed in parallel; one with the decision support system and the other the usual procedure. Results from the both were documented and compared to find the differences, if any. This process helped out to find out both technical and procedural errors in protocol development and software development side.
Technology development
Though we initially envisioned developing a dedicated handheld for the purpose, limitation of resources and long term-sustainability i.e. maintenances cost in small scale we went for off-the shelf handheld devices and JAVA enabled mobile phones. We observed mobile phones with screen size more than 2.5 inch is found to be best suited for this kind of intervention owing to low maintenance and upfront cost. We used both handheld device and mobile phone for the purpose of study and improved the user interface with iterations with the feedback from the field. Functional process of Technology Development Unit is shown in Figure 5. Details for evolution of the technology developed for Decision Support System shown in Figure 6.
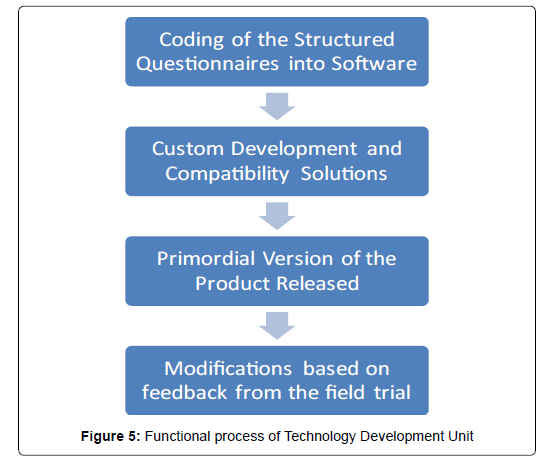
Figure 5: Functional process of Technology Development Unit
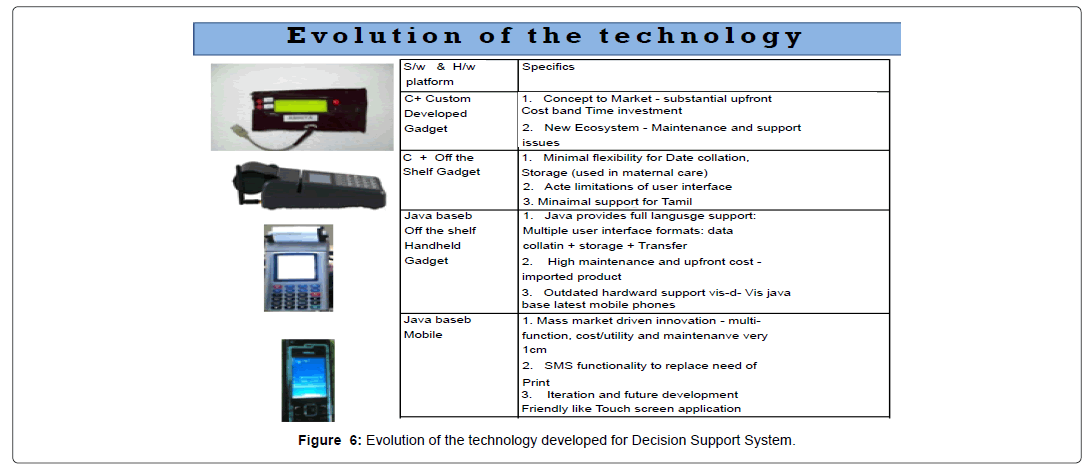
Figure 6: Evolution of the technology developed for Decision Support System.
• The devices were customized to be used by a treating physician / Medical Officer (M.O.) or a Village Health Nurse (VHN) or Staff Nurse at Primary Health Center (PHC) or at the patient’s door step.
• Software was developed for use on a custom built handheld, a symbian and a JAVA based Point-of-Sale device, a JAVA based mobile phone
• The Software were uni-code compatible and were made available in the local vernacular language- Tamil.
• After cycles of iterative debugging, the Software was run 500 times on hypothetical pediatric and antenatal case scenarios (predefined by the expert panel) by 10 certified physicians over 2 weeks time and inconsistencies were reported for revision.
• The pilot run of the software was carried in the out-patient Dept (OPD) of Institute of Social pediatrics, Government Stanley Hospital and Antenatal OPD, Govt. RSRM Hospital.
Simulation
Example of protocol for assessment of acute respiratory infection of 2 month to 5 year is described in Figure 7. Figure 8 shows the print generated by DSS.
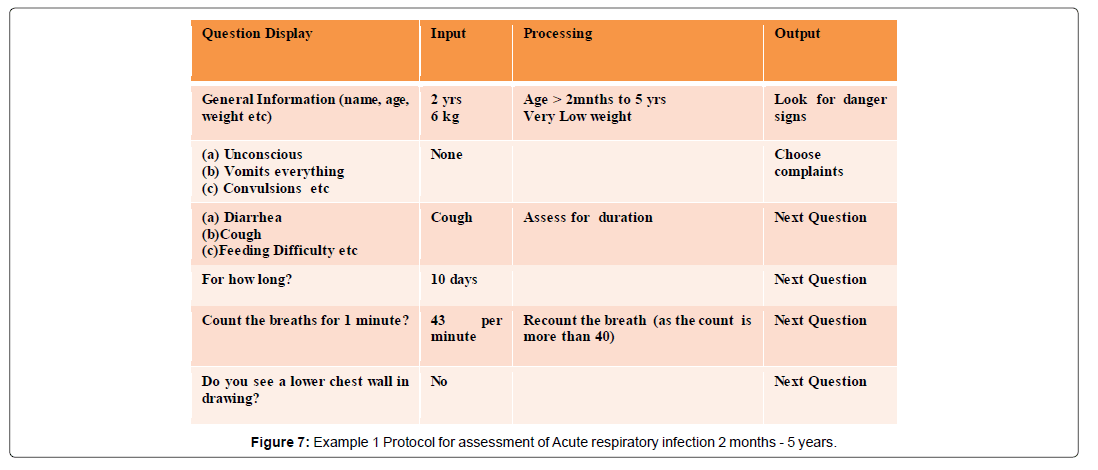
Figure 7: Example 1 Protocol for assessment of Acute respiratory infection 2 months - 5 years.
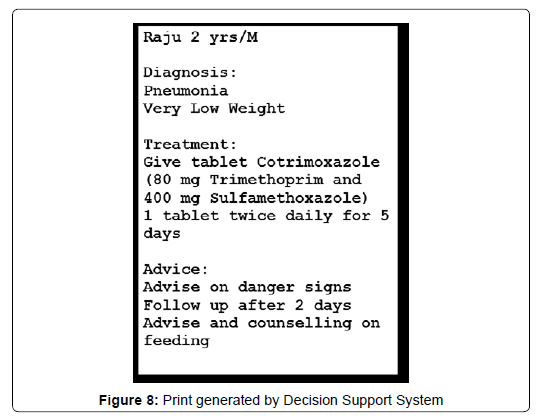
Figure 8: Print generated by Decision Support System
First phase: After obtaining informed consent form the participants, we tested our Decision Support System (DSS) for maternal and childcare in two phases. The first phase involved live testing of the DSS in the urban hospital and in second phase it was given to Village Health Workers (VHWs) in rural Primary Health Centers, for which it was originally made. Objective in the first phase was to validate the protocol from live cases by juxtaposing the diagnosis and treatment of both with and without decision support. In first phase, antenatal care of maternal protocol was tested by four house surgeons, in the Outpatient Department (OPD) of obstetrics and gynaecology at Government Raja Sir Ramaswamy Mudaliar (RSRM) lying-in hospital, Chennai and Post natal care in the inpatient obstetric ward of RSRM, Chennai. The decision support for childcare for 2 months-5 years was tested in Institute of Social Paediatrics and 0-2 months in neonatology OPD.
We intentionally chose the house surgeons for the field trial who were not part of the core team to get an unbiased result of field trial.
First we demonstrated the software to four house surgeons and ran 20 simulation cases. Before going to the field it was important to validate our decision support software by doing clinical trial by matching the diagnosis and treatment of the software with that of a trained physician who were experts in their respective fields of Pediatrics and Obstetrics and Gynaecology. The samples consisted of 527 cases in maternal care this was calculated based on the prevalence of high risk pregnancy such as anemia and 344 cases in childcare base on the sensitivity of the IMNCI protocol. These were recorded in maternal and paediatric ward of Stanley medical college to validate our protocol and making the changes as suitable. Special care was taken to see that the intervention did not compromise the regular treatment received by patients.
Second phase: We chose two rural Primary Health Centers (PHC), Neemam and Thirunindravur nearby Chennai for the Second Phase field trial. Nemam is a village, south of Chennai and Thirunindravur is a town panchayat in Thiruvallur district of Tamil Nadu, situated at a radius of 32 Km from Chennai.
The objective of the field trial was to gauge the attitude of village health worker towards technological intervention. We asked two sets of questions, pre intervention and post intervention to assess the change in their attitude. In the second phase of trial in rural PHC, we first conducted interviews with nine village health workers to understand their previous experience with using mobile phone or any electronic gadget, experience with IMCI and/or maternal protocol and preconceptions about technological interventions, if any.
Next, we observed the VHWs providing healthcare as they usually do in order to understand their clinical practices. Then, we introduced the software by training each VHW to run through the software with a standard case and explaining the usage of key and navigation which involved a 3 hour training session. The VHWs were given some practical time to adapt to the software and they were able to train each other to understand the navigation within 20 minutes all major doubts were addressed in the training session. From here we observed a series of trials in which the VHWs used the decision support to classify and treat the illness or asses risk in maternal check-up under the supervision of professional doctor who ensured safe care. Data analysis was done using OpenEpi, Version 2, open source calculator.
All the cases interviewed during field trial were documented in a pre-specified form and results are summarized below. 527 cases in maternal care and 344 cases in childcare were recorded for the purpose of study. Profile of the maternal and child care cases shown in Table 1. To assess the accuracy of the classification and treatment suggested by our decision support system we used a binary classification test by comparing it with the diagnosis of a trained physician. In the absence of a neutral observer to serve as a gold standard, we have taken the decision by the trained physician to serve as gold standard for our study. Different cases in maternal care check-up are given in Table 2.
| Catergory | Male | Female |
|---|---|---|
| Antenatal | 424 | |
| Postnatal | 103 | |
| 0-2months | 42 | 42 |
| 2months-5years | 143 | 117 |
Table 1: Profile of the Maternal and child care cases
| Classification | Number of cases encountered | ||
| High risk pregnancy | Systemic Illness | 141 | 225 |
| Anthropometric risk | 8 | ||
| BOH | 59 | ||
| Maternal age | 17 | ||
| Hyperemesis | 8 | ||
| Morning sickness | 12 | ||
| Anemia | Severe | 24 | 38 |
| Moderate | 14 | ||
| Possible Candida infection | 20 | ||
| Pre-eclampsia | 21 | ||
| Gestational hypertension | 9 | ||
| Physiological edema | 7 | ||
| Weight gain less than gestational age | 10 | ||
| Respiratory illness | 10 | ||
| Abnormal fetal development | 15 | ||
Table 2: Classification of the various cases in maternal care check-up disease wise.
Due to the comprehensive debugging and protocol development procedure we achieved nearly nil mismatches in the 0-2 months and maternal care. The software for 2 months-5 year found some mismatch for which the result of analysis is shown in Table 3. Apart from “acute severe malnutrition”; other disease classification found Kappa value to be above 0.9 which signifies accuracy of diagnosis of decision support [15]. Classification of diseases according to IMNCI is shown in Table 4. The maternal care and 0-2 months protocol found almost nil mismatch; though it might be a result of less data. The objective of the field trial was to gauge the attitude of village health worker towards technological intervention. We asked two sets of questions, pre intervention and post intervention that had major part in common, to 9 village health workers to assess the change in their attitude if any. The results are summarized below. It was observed that despite the fact none of the health-workers had used mobile for delivering health services before apart from voice consultation for follow-up and their presumption of it to be tough, 80% of them believed adoption by other health-workers would not be a challenge post intervention. There was 100% agreement among health workers about the benefits in
| Classification | Decision Support Technology Assessment | Physician Assessment | Kappa* | Sensitivity* (%) | Specificity* (%) | Positive Predictive Value (%) | Negative Predictive Value(%) | Diagnostic Accuracy | |
| Yes | No | ||||||||
| Acute Respiratory Infection | Yes | 214 | 3 | 0.931 | 99.07 | 93.18 | 98.62 | 95.35 | 98.08 |
| No | 2 | 41 | |||||||
| Acute Diarrheal Disease | Yes | 26 | 2 | 0.939 | 96.3 | 99.14 | 92.86 | 99.57 | 98.85 |
| No | 1 | 231 | |||||||
| Acute Febrile Illness | Yes | 37 | 3 | 0.939 | 97.37 | 98.65 | 92.5 | 99.55 | 98.46 |
| No | 1 | 219 | |||||||
| Acute Severe Malnutrition | Yes | 18 | 11 | 0.843 | 100 | 97.07 | 75 | 100 | 97.31 |
| No | 0 | 188 | |||||||
Table 3: Agreement of the Decision Support with the Physician in making diagnosis for the common diseases encountered in children between 2 Months to 5 Years (*The v Wilson score method is followed [14])
| Classifications | Diseases |
|---|---|
| Acute Respiratory Infection | Severe Pneumonia, No Pneumonia, No Pneumonia: Cough and cold |
| Acute Diarrheal Disease | Dehydration(Some, Severe), Persistent Diarrhoea, Dysentery |
| Acute Febrile Illness | Very Severe Febrile disease, Malaria, Measles and Complicated Measles |
| Acute Severe Malnutrition | Persistent Diarrhoea, Severe Malnutrition, Very low weight, Low weight |
Table 4: Classification of diseases according to IMNCI
1.Tracking of quantitative parameters like weight, height, Hb, BP.
2.Follow-up and tracking.
3.Reminders for missed immunization and risk-pregnancy cases.
4.Record keeping.
7 out of 9 village health-workers agreed that intervention will be useful for the followings;
1.Eliciting signs and symptoms.
2.Provisional diagnosis, treatment and referral.
The results of this study impinge upon us the challenges and opportunities for computer-assisted decision support technology especially in low-resource environments. Confidence in the software program by stakeholders is a key element in the wider application of decision support technology. A similar study done by David H Peters et al. In rural Tamil Nadu among 1557 consecutive patients taken from two busy outpatient clinics to compare assessments made by their decision support system and an independent panel of physicians, showed that in their study the sensitivity of the referral decision was high (80%) though the specificity was quite low (22%), with relatively low positive and negative predictive values (65and 38% respectively) and their software had a low level of Kappa agreement [9]. In our study the sensitivity was above 95%, specificity was above 93%, positive predictive value was above 90% except for acute severe malnutrition (75%), negative predictive value was also above 95%, diagnostic accuracy was above 97% and Kappa value was found to be above 0.9 which signifies accuracy of diagnosis of decision support. This might be due to the fact that our software was developed on the basis of existing known protocol such as the IMNCI and also due to the differences in the nature of the target population as we focussed entirely on maternal and child care.
The usage of handheld device and cellular phone by the fieldbased health workers enabled them to be mobile and freed them from the confines of their desks. This enabled the delivery of home based treatment and follow up visits at the grass root level, thereby potentially reducing the burden on the medical officer though this was beyond the scope of our study. The devices also made it possible for the field workers to make home visits which could be helpful for antenatal and postnatal mothers and saving them the need for travel unless absolutely necessary. The data from the handheld devices can also be transferred to desk top computers which in turn can be linked to central databases via the internet. Thus this peripheral door step technology can be linked to central computers for analysis and review by specialists at higher levels of healthcare.
We found that a typical Village Health Worker in the study population was open to technology and felt this could make a difference in what she did every day. It helped in the tracking of quantitative parameters like weight, height, Hb, BP, follow-up and tracking was easier, reminders for missed immunization and risk-pregnancy cases were enabled and record keeping was easier. The DSS assisted them in eliciting signs and symptoms, making easier provisional diagnosis, treatment and referral. The current study has its limitations both in terms of number of VHWs involved and days of the study. However, we believe, with a tangible decision support technology in our hands, we will be able to visualise things better and it should provide an essential kick start to the concept of popularizing decision support technology to aid the Village Health Workers functions- decision making, monitoring, follow up, record keeping. Much more remains to be explored.
Village Health worker together with clinical Decision Support System as one unit perform almost as good as a clinician in primary care, filtration and referral of emergencies with regard to Maternal and Child Health. The Decision Support System increases adherence to protocols and compliance to instructions, therefore the model may prove to be a highly replicable model.
We thank the Mission Director, National Rural Health Mission, Tamil Nadu for sharing our faith in the idea and encouraging us through out. The project would not have been possible without the financial support from National Rural Health Mission. We thank the Deputy Director, Ponamallee for making it easy for us to conduct the field trial in the PHCs of Nemam and Thirunindravur. We are thankful to the Professors of Obstretics and Gynecology, Govt RSRM Hospital and Professors of Pediatrics, Institute of Social Pediatrics for their advice and invaluable inputs. We thank our house surgeons and the village health nurses who helped in data collection. Last but not least we thank all the participants for their co-operation which was essential for this study to be fruitful.