Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2015) Volume 5, Issue 2
Effective interventions have been developed to promote STI/HIV protective behaviors among populations most vulnerable to infection, including African-American adolescent females. However, intervention effects show marked and rapid decay following cessation of the intervention. Consequently, the maintenance of protective behaviors for extended periods of time has become a priority for researchers and health professionals. The objective of this report is to describe the use of a supplemental treatment trial design of a behavioral STI/HIV prevention maintenance intervention, which includes a primary treatment (i.e., intervention workshop) followed by an additional treatment (i.e., calls) designed to maintain the effects of the primary treatment. The treatment was tested in a randomized controlled trial among 701 African-American adolescent females, ages 14-20, over a 36-month follow-up period. Upon completion of an evidence-based intervention (primary treatment), participants randomly assigned to the
experimental condition received brief, telephone-delivered counseling sessions (supplemental treatment) reinforcing intervention content every 8 weeks over the 36-month follow-up period. Participants randomly assigned to the comparison condition after the primary treatment received time-match health and wellness calls. Experimental condition participants had significantly fewer incident chlamydial infections, and reported higher proportion condom use and fewer instances of sex while intoxicated by alcohol or drugs. Supplemental treatment trials are not frequently used in STI/HIV prevention but may be a promising approach for evaluating behavior change maintenance.
Keywords: STI; HIV; Sexual risk; African-American females; Adolescents; Supplemental treatment; Randomized controlled trial; Intervention.
Significant disparities in sexually transmitted infections (STIs) and HIV/AIDS exist between African-Americans and other racial/ethnic groups in the United States. African-Americans comprise12% of the population, but accounted for 44% of new HIV infections in 2010 [1]. In 2010, HIV infection rates were 20 times higher for African- American women compared to White women [1]. Additionally, African-American adolescent females also experience markedly elevated rates of gonorrhea and chlamydia [2], co-factors that increase HIV transmission dynamics in females [3-5]. Consequently, preventing new STI/HIV infections among African-American adolescent females has garnered much attention among researchers and healthcare professionals.
In response to the observed disparities in STIs and HIV, efficacious interventions targeting African-American adolescent females have been developed and identified as effective in reducing STI/HIV risk [6,7]. Behavioral interventions, such as SISTA [8], SiLHE [9], HORIZONS [10], Enhanced Negotiation [11], and Sister to Sister [12], among others, have demonstrated effectiveness in promoting the adoption of STI/HIV preventive behaviors and have been widely disseminated [13]. While efficacious, evidence indicates that intervention effects decay rapidly following cessation of the intervention [14,15].
For behavior change to be meaningful it must be durable. Thus, it is critical that intervention effects are maintained to achieve lasting reductions in risk of STI/HIV infection. To date, there is a paucity of research examining maintenance interventions designed to sustain STI/HIV preventive skills acquired through group-based prevention interventions over protracted time periods after participation. One research design that may lend itself well to studying the maintenance of intervention effects is the supplemental treatment trial design. The distinguishing factor between a randomized controlled supplemental treatment trial and a typical randomized controlled trial is that instead of receiving only a primary treatment participant receive a primary treatment followed by a different (supplemental) treatment to maintain the primary treatment’s effects [16]. The rationale for this type of design is that a supplemental treatment(s) may prevent the resurgence of factors that contribute to the recurrence of a disease after it has been resolved by a primary treatment. Supplemental treatment trials are commonly used in cancer research. Following surgery to excise cancer cells some patients may receive additional treatments, referred to as supplemental or adjuvant therapy, to reduce the risk of recurrence. Supplemental treatment trials have been conducted to test treatment efficacy; some suggest supplemental (adjuvant) treatments have been efficacious, specifically in reducing breast cancer recurrence [17,18].
Supplemental treatment trials have been utilized less often in behavioral and social science research. Yet, the underlying rationale for this approach suggests the intervention design may prove useful for STI/HIV prevention research. In the context of behavioral interventions, it is common for individuals who have acquired new skills to regress back to previous behaviors over time [14,15,19,20]. According to the Transtheoretical Model [21,22], individuals cycle through several stages of change to successfully adopt new behaviors. In order to sustain behavior change, an individual must progress from the initiation of a new behavior (action stage) to a maintenance stage in which the emphasis is relapse prevention, and ideally to a termination stage where regression to previous behavior is highly unlikely. Reinforcing the knowledge and skills that produced the initial behavior change may help sustain the new behavior until it replaces the old one. Consequently, supplemental treatments for STI/HIV prevention interventions may aid the maintenance of desired behaviors, such as correct and consistent condom use, through repeated opportunities to reinforce knowledge and skills. Therefore, the purpose of this report is to describe the use of a supplemental treatment trial design to examine whether brief, targeted phonecounseling (supplemental treatment) would sustain the effects of an evidence-based STI/HIV prevention intervention for African- American adolescent females (primary treatment) over a 36-month follow-up period More specifically, the primary objective of the report is to describe how a supplemental treatment trial design is a useful study design for investigating long-term behavior maintenance.
Study design
The researchers utilized a 2-arm randomized controlled supplemental treatment trial design to test maintenance of intervention effects over a 36-month period (Figure 1). In a supplemental treatment trial, participants receive a primary treatment followed by a different (supplemental) treatment to maintain the primary treatment’s effects [16]. In the present study, all participants received the primary treatment, HORIZONS, which was an efficacious, group- delivered, CDC-defined evidence-based STI/HIV intervention designed for African-American adolescent females [10]. Following implementation of HORIZONS, the supplemental treatment for participants in the experimental condition was a newlydeveloped Prevention Maintenance Intervention (PMI) that consisted of brief, tailored phone counseling administered every 8 weeks over 36 months (18 total phone contacts). Comparison condition participants received a time- and dose-equivalent phone-counseling placebo General Health Promotion (GHP) intervention designed to reduce the likelihood that effects of the PMI were attributable to differences in exposure to staff contact.
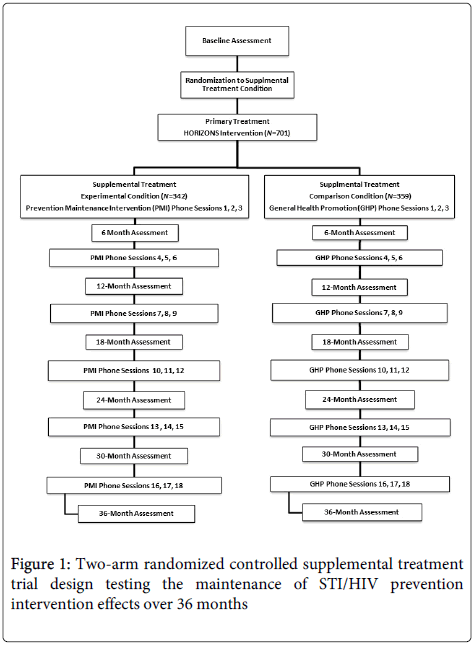
Figure 1: Two-arm randomized controlled supplemental treatment trial design testing the maintenance of STI/HIV prevention intervention effects over 36 months
Each participant was randomly assigned to the experimental (PMI) or comparison (GHP) condition by a member of the assessment staff upon completion of the baseline assessment. To promote unbiased randomization, concealment of allocation techniques were used [23]. Prior to the start of the study, a computer algorithm was used to generate a random allocation sequence. Slips of colored paper representing either the experimental or comparison condition were placed in small, sealed envelopes and numbered according to the sequence. After completing the baseline assessment, participants were given the next envelope in the sequence and asked to open it. The participant showed the slip to the assessment staff member who then recorded the participants study condition in the randomization log.
Participants
Participants were 701 African-American females, 14-20 years old at baseline assessment. Adolescents were eligible if they self-identified as African-American, were between 14 and 20 years old, and had vaginal sex without a condom at least once in the past 6 months. Those who were married, pregnant, or trying to become pregnant were not eligible to participate. Eligible participants were scheduled to return to the clinic on a designated day to complete the consenting process, baseline assessment and group-based intervention workshops (primary treatment). Of the eligible adolescents, 94% (N=701) were enrolled, completed baseline assessments, and were randomized to a study condition.
Human subjects protection
Due to the sensitive nature of the research, measures were implemented to protect the study participants. Recruiters were instructed to highlight confidentiality and assure participants that their responses to the eligibility screening questions would not be shared with their parents or the clinic staff. Eligible participants completed the consent process when they returned to the clinic for baseline data collection and intervention workshops. Upon arrival, staff members reviewed the consent form with participants and answered any questions before they provided written consent to participate in the study. Participants were not required to provide parental consent for the study because they were already confidentially seeking sexual health services at their respective clinic. All study protocols were approved by Emory University’s Institutional Review Board.
Recruitment and retention
Adolescents were recruited during a 2-year period (June 2005 to June 2007) from three clinics in Atlanta, Georgia that provided sexual health services for free or on a sliding scale. Individuals were approached in the clinic waiting area by an African-American female recruiter, informed about the study, and invited to be screened for eligibility. During the 5-10 minute screening process participants received a more detailed overview of the study and answered questions regarding demographic information and sexual behavior during the past 6 months to determine eligibility. Recruiters were trained to elicit information using strategies to reduce the potential impact of social desirability bias and recall bias in participants’ responses. Specifically, recruiters were taught to create rapport with individuals, communicate in a nonjudgmental manner, consider both verbal (i.e., use of certain words or phrases) and nonverbal (i.e., facial expressions) communication, and encourage participants to answer honestly. In addition, recruiters utilized a simplified version of the Timeline Followback (TLFB) method [24] (i.e., using a calendar to specify the 6- month (180 day) range and highlight holidays and special events) to help participants estimate the frequency of vaginal sex without a condom 6 months (180 days) prior to being screened. Lastly, recruiters provided participants with a definition of vaginal sex (i.e., when a male inserts his penis into your vagina) and probed for condom use errors (i.e., condom broke or was not used the entire time) among individuals reporting 100% condom use to reduce misclassification.
To bolster retention, participants received post cards and phone calls beginning two weeks prior to their follow-up assessments. Participants were also given items with the project logo and phone number (i.e., pens and key chains) and encouraged to update their contact information as needed. In addition, upon enrolment and at each follow-up assessment, participants updated their contact information and provided contact information for other individuals through whom they could be reached if their contact information changed. Study staff did not provide the additional contact person with any information about the participant’s involvement in the research study.
Compensation
Participants received monetary compensation to offset costs associated with their participation such as travel, childcare, or lost wages. Participants received $75.00 for completing the baseline assessment and intervention group session, $20.00 for completing each of the 6-, 12-, 18-, 24-, 30- and 36-month follow-up assessments, and $10.00 for each of the 18 individual phone sessions. Payments were made to participants upon completion of their research visit.
Treatment descriptions
During intervention development, both the HORIZONS intervention session and PMI/comparison phone sessions were pilot tested with adolescents recruited from the study clinics to assess feasibility and acceptability.
The primary treatment, HORIZONS, was a group-based intervention with didactic and interactive features designed for African-American adolescent females based on the Theory of Gender and Power and Social Cognitive Theory. The goal was to enhance STI/ HIV-preventive attitudes, practice sexual negotiation and refusal skills, and promote safer sex norms. The researchers chose HORIZONS since the efficacy was evaluated in a randomized controlled trial in 2009, with findings demonstrating significant reductions in chlamydial infections and sexual risk behaviors over a 12-month follow-up with the same target population [10].
In the current study, HORIZONS was modified from a two-day (eight total hours) to a one-day (six total hours) session led by two trained African-American female health educators. The one-day intervention maintained the core elements from the two-day HORIZONS, including ethnic and gender pride, role models, sexual health decision-making, HIV/STI knowledge, healthy and unhealthy relationships, and safer sex negotiation. The intervention activities directly addressing the primary behavioral outcomes (proportion condom use and frequency of sex while intoxicated) included practicing condom application skills, understanding personal risk factors, practicing healthy communication skills, and using scenarios to role-play refusing unsafe sex and negotiating safer sex. All participants received the HORIZONS workshop (primary treatment) before being randomly assigned to the supplemental treatment group (PMI) or comparison phone sessions.
The supplemental treatment was the phone-counseling prevention maintenance intervention (PMI). The PMI was a health-educator administered phone contact, lasting between 10 and 15 minutes, tailored to each participant, and occurring three times during the 6 months between each follow-up assessment. Health educators used a scripted algorithm first confirm participants’ sexual health goals (abstinence, condom use, or neither) written at the end of the group workshop. Then, Health Educators assessed participants’ barriers to maintaining their sexual health choice (abstinence or condom use); barriers included negative attitudes about condoms, low condom use skill efficacy/knowledge, and partner- or relationship-specific barriers. Health Educators presented multiple strategies to increase condom use or abstinence (i.e. abstaining from sex, initiating condom use, maintaining consistent condom use, STD testing, sexual partner communication), to increase the likelihood participants identified at least one option to help them successfully achieve and maintain their sexual health goal [25]. For the General Health Promotion comparison condition, the phone sessions focused on nutrition and physical activity goals set by the participant and barriers they encountered toward achieving their goals. These calls were time-matched to the PMI calls and occurred on the same schedule (18 total calls).
Health Educators’ training included initial HORIZONS workshop training (two days), PMI call training (one day), and bi-monthly meetings with Lead Health Educators to debrief workshop and call sessions, discuss facilitation challenges, and share project updates. Additionally, the Lead Health Educators provided individualized support to Health Educators completing PMI calls. Protocol for completing PMI calls included: determining the best time to reach participants (i.e., varying the time and days of the week), making at least five call attempts in the allotted two-week window, and methods for contacting non-responsive participants (i.e., texting, using social media, and discretely contacting additional contacts provided by participants as a reference.
Data collection
Prior to randomization, participants completed a baseline assessment which included a self-collected vaginal swab specimen for STI testing and a computer survey assessing demographic and behavioral information. Participants returned and completed followup assessments at 6-,12-, 18-, 24-, 30- and 36-months after participation in the primary treatment, HORIZONS.
Biospecimen collection staff used an anatomical model to instruct participants regarding procedures to obtain the self-collected vaginal swab specimens [26]. Specimens were assayed for two bacterial pathogens, C. trachomatis and N. gonorrhoeae using the BDProbeTec ET C. trachomatis and N. gonorrhoeae Amplified DNA assay (Becton Dickinson and Company, Sparks, MD) [27]. Nucleic amplification technology (NAAT) is not routinely used for STI detection. Although these assays are more expensive, they were used for this study because they are less invasive and more sensitive and specific than culturebased tests. Participants with a positive test were notified within approximately 5 days of testing and provided directly observed singledose antimicrobial treatment, risk-reduction counseling per CDC recommendations, and encouraged to refer sex partners for treatment. The Fulton County Health Department was notified of these reportable STIs.
Following biospecimen collection, participants completed a 60- minute computer survey assessing several domains including sociodemographics, sexual behavior, substance use, attitudes and outcome expectancies, psychosocial variables, HIV/STI knowledge, and peer norms. Several measures were implemented to improve the validity of self-reported data. In an effort to facilitate more accurate recall, behaviors were assessed for 3-month (90 day) and 6-month (180 day) intervals prior to the assessment using a Timeline Followback (TLFB) approach [24]. Assessment staff gave participants a calendar, defined the recall time period for them, and reminded them to consider whether the time frame included any holidays, special occasions, or events during which their behavior may have been atypical. For example, a participant completing her assessment in April would be instructed to consider her behavior for the past 6 months, which would include November through April. She should carefully consider any occasions that occurred within that time period (i.e., spring break) during which substance use or sexual behavior, for example, may have differed from typical behavior patterns when calculating behavior frequencies. Further, the survey was administered via audio computer assisted self-interview (ACASI) technology to decrease social desirability bias for the reporting of sensitive information, such as sexual behavior [28], as well as to address potential literacy issues [29].
Outcome Measures
Biological and behavioral outcomes were primary outcome measures [30]. Biological outcomes included incident (new) infections of Chlamydia or gonorrhea as confirmed by laboratory testing during the 36-month study period. STI biological markers were used as a complementary measure of sexual risk due to potential issues regarding the reliability and validity of self-reported condom use [31,32]. Biomarkers provide a more objective and quantifiable measure of high risk behavior. Before electing to use STIs as outcomes a number of factors were carefully weighed. For instance, STIs would not be feasible or appropriate in studies with a short-term follow-up or in a very low-risk population, such as those with a low prevalence of STIs or those with no sexual experience or low frequency of sex. However, data from the efficacy study of the primary treatment, HORIZONS, indicated that young women attending the clinic have high rates of risky sexual behavior and an annualized STI re-infection rate of 25%; thus, the use of biological markers was deemed appropriate.
Primary behavioral outcomes measured at each 6-month (180 day) follow-up assessment were (1) proportion of condom use and (2) number of occasions when participants had sex while intoxicated by alcohol or drugs. The proportion of condom use was assessed for the past 3 months (90 days) and full 6-month (180 day) period since the last assessment. For each time period, the proportion of condom use was calculated by dividing the number of times participants reported using condoms (“Out of the xx times you've had vaginal sex, in the past 6 months (180 days)/3 months (90 days), how many times did you use a condom?”) by the number of times they reported having vaginal sex (“In the past 6 months (180 days)/3 months (90 days), how many times have you had vaginal sex?”). The frequency of engaging in sex while intoxicated was assessed using a single item: “In the past 3 months (90 days), how many times did you have sex while high on alcohol or drugs?”
Statistical analysis
A power analysis indicated 700 participants were needed to conduct the statistical analyses. The power analysis was based on achieving 80% power for a two-tailed test at a 0.05 alpha level. A 20% reduction in incident Chlamydial infections over 36-months was used to estimate the treatment effect based on the results of the HORIZONS trial [10]. Since participants were assessed multiple times during the study, methods for handling repeated measures data were utilized [33]. An estimated 20% correlation was used to account for within-person measurements. The sample size estimate was also based on an 80% completion rate for each follow-up assessment.
An intent-to-treat approach was used for statistical analyses of STI and behavioral outcomes. Thus, participants were classified based on the treatment condition to which they were assigned despite their level of exposure to the intervention [15]. For example, a participant randomly assigned to the intervention condition who did not complete any phone calls was still classified as an intervention condition participant.
Preliminary analyses identified variables to include in statistical models evaluating intervention effects for the 36-month follow-up period. Variables were selected based on theoretical or empirical relevance, as well as those associated with outcome measures in bivariate analyses (p<10). Bivariate analyses included t-tests and chisquare tests.
Generalized estimating equation (GEE) models were utilized to evaluate the efficacy of the supplemental treatment (PMI calls). Within-subject correlations were accounted for using random effects estimates for each person and exchangeable correlations in GEE models [34]. Fitted models were adjusted to account for baseline measures and covariates, as well as study site and cohort, to generate adjusted risk ratios (95% confidence intervals) for the dichotomous STI outcomes and adjusted mean differences for the behavioral outcomes. Additionally, an estimated linear regression model was used to assess behavioral outcomes at 36-month follow-up assessment. Models were adjusted for baseline measures of each outcome, theoretically or empirically relevant variables, and sociodemographic variables that varied by study condition at baseline. Stata software was used to conduct statistical analyses (version 12; StataCorp, College Station, Texas).
Analyses revealed primary treatment effects were maintained using the supplemental treatment approach. Incident infections for Chlamydia were less frequent among individuals who received the supplemental treatment (telephone-delivered counseling) compared to those in the comparison condition during the 36-month follow-up period [94 (30.5%) versus 104 (32.7%); RR=0.50; 95%CI 0.28 to 0.88; p=0.017]. Differences in incident gonococcal infections approached significance as well [48 (15.6%) versus 54 (17%); RR=0.40; 95%CI 0.15 to 1.02; p=0.056] (Table 1).
| Sexually Transmitted Infections (STIs) | RR | 95% CI | p |
|---|---|---|---|
| Incident Chlamydial infections | 0.5 | 0.28, 0.88 | 0.017* |
| Incident gonococcal infections | 0.4 | 0.15, 1.02 | 0.056 |
| Protective Behaviors | Mean Difference | 95% CI | p |
| Higher proportion of condom use in the past 3 months | 0.08 | 0.06, 0.11 | 0.021* |
| Higher proportion of condom use in the past 6 months | 0.08 | 0.06, 0.10 | 0.036* |
| Frequency of sex while intoxicated | -0.61 | -0.98,-0.24 | 0.0001* |
Note: *Statistically significant at the .05 alpha level. Analyses were conducted using data from experimental (n=309) and control (n=318) participants who completed at least one follow-up.
Table 1: Differences between the experimental and control condition participants over 36 months
Supplemental treatment was also effective for sustaining protective behaviors. The mean (SD) number of telephone contacts received by participants was10.78 (5.44) in the experimental condition and 9.86 (5.22) in the comparison condition (p = .02). At follow-up, individuals assigned to supplemental treatment also reported a higher proportion of condom use in the last 3 months (mean difference=.08; 95%CI 0.06, 0.11; p=0.021) and 6 months (mean difference=.08; 95%CI 0.06, 0.10; p=0.036). Further, they reported having sex while intoxicated by alcohol and/or drugs less frequently than individuals in the comparison group (mean difference=-0.61; 95%CI -0.98,-0.24; p=0.0001) (Table 1). A more extensive description of the results is reported elsewhere [35].
In order to achieve significant, long-term decreases in STI/HIV disparities between African-Americans and other racial/ethnic groups in the United States it is critical that intervention effects are sustained over time. Since African-American adolescent females are at increased risk for infection, this vulnerable population remains a primary target for risk reduction intervention efforts. One approach that may be useful for promoting maintenance of desired protective behaviors that prevent STI/HIV transmission is the use of a supplemental treatment to sustain short-term effects from participation in a single session group-based STI/HIV prevention intervention. Although this approach is used most often in cancer research to evaluate the effectiveness of adjuvant (supplemental) treatments in preventing recurrence, the principle may also be applicable to individuals participating in a STI/HIV prevention intervention to prevent regression back to risky sexual behaviors over time.
Strengths of the supplemental treatment trial design used for our investigation include selecting HORIZONS as the primary treatment. Using an evidence-based intervention with previously demonstrated support for its efficacy in increasing condom use and reducing incident Chlamydial infections among a similar population is important for producing initial effects needed to conduct a maintenance study. Moreover, the use of a time-matched intervention for the comparison group helps eliminate bias associated with differential time spent with and attention given to participants. Therefore, alternative explanations, such as behavior maintenance being due to continued contact with the participant, not the reinforcement of intervention content, can ruled out. Additionally, the 36-month follow-up period permits the examination of behavior maintenance over a substantial period of time. This extended view can provide a more accurate assessment of participants’ risk trajectory. Other strengths include random assignment to supplemental treatment condition, as well as allocation concealment procedures for randomization, strategies to reduce social desirability and recall biases in eligibility screening and assessments, multifaceted retention efforts, and the use of STI biomarkers in addition to self-reports of sexual behavior.
Challenges associated with implementing a supplemental treatment trial also warrant discussion. First, identifying an effective primary treatment may be difficult. In some instances it may be necessary to adapt an intervention to fit the specific needs of the target population. If so, it would be advantageous to test the efficacy of the intervention before conducting an investigation of maintenance. Next, investigators should consider the availability of resources needed to execute the study, particularly for a lengthy follow-up period. Implementation may be time and labor intensive depending on the type of treatments (both primary and supplemental). Similarly, expertise required for staff members delivering the primary and supplemental treatments, as well as other staff members, is another important consideration.
It is important to note that substantial decreases in intervention efficacy over time are not unique to STI/HIV prevention. For example, maintenance of intervention effects has also been noted as a priority in recent reviews of interventions promoting physical activity, healthy eating, and smoking cessation [20,36-38]. Thus, for future research studies in STI/HIV prevention or other fields where healthy behaviors adopted during an intervention may deteriorate or cease after the intervention is completed it may be advantageous for investigators to consider utilizing a supplemental treatment trial design to test strategies for sustaining initial effects produced by an intervention for longer periods of time. For example, supplemental treatment trials may be used to explore whether utilizing technology to deliver messages that reinforce intervention content can prolong initial intervention effects when compared to other strategies (i.e., face-toface follow-up) or to no subsequent treatment. Evaluating the efficacy of different content and delivery modalities can help researchers and healthcare professionals identify the most efficient ways to maintain intervention effects. As a result, we may enhance our ability to make significant advances toward reducing risky sexual behavior among individuals and decreasing disparities between groups.
This research was funded through the National Institute of Mental Health: HIV Prevention Maintenance for African-American Teens (5R01 MH070537). Additional support was provided through the Emory Center for AIDS Research (P30 AI050409).