Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2016) Volume 6, Issue 2
Purpose: Long-term (3-5 years) results following inguinal hernia repair in a large series of patients using a novel technique-the ONSTEP approach-are presented. In particular, the recurrence rate, long-term complications and patient satisfaction with the procedure are discussed.
Methods: Adult patients underwent ONSTEP inguinal hernia repair using a PolySoft™ hernia patch. All procedures were performed by one of two surgeons. Patients were followed up for 3-5 years for recurrences and complications, including chronic and residual pain. Patients were also asked to rate their satisfaction with the procedure.
Results: Data were available from 398 hernia repair procedures in 314 patients at the 3-5-year follow-up. The overall recurrence rate was 2.0% (8/398). Additionally, there were 14 cases (3.5%; 14/398) of residual pain and 5 cases (1.3%; 5/398) of wound infection. No patients experienced chronic pain and there were no cases of mesh infection. Patient satisfaction with the ONSTEP procedure was high, with 94.9% of patients rating it as excellent, very good or good.
Conclusions: ONSTEP inguinal hernia repair produced consistent results in the long term, and was associated with a low recurrence rate, only minor complications and no chronic pain. The procedure offers an alternative approach to both Lichtenstein and laparoscopic repair.
Keywords: Inguinal hernia repair; Open hernia repair; ONSTEP hernia repair; Chronic pain; Residual pain; Recurrence
The ideal surgical technique for inguinal hernia repair is still open to debate. Current options are open repair, which involves opening the abdominal wall and repairing the hernia with sutures or a surgical mesh, and laparoscopic repair, in which the hernia defect is repaired through small incisions with a surgical mesh without the need to open the abdominal wall [1]. Lichtenstein repair [2] is the most commonly used open procedure, despite the fact that it causes chronic post-operative pain in a large proportion (15-40%) of patients [3]. Laparoscopic procedures are associated with a reduced rate of post-operative pain compared to open repair [4-7], but they take longer to learn and are more expensive to perform [8-12].
The two main approaches to laparoscopic inguinal hernia repair are the transabdominal preperitoneal (TAPP) approach, where the hernia is repaired via the peritoneal cavity, and the totally extraperitoneal (TEP) approach, where the hernia is repaired via the preperitoneal plane without entering the peritoneal cavity [1]. As the TEP approach does not involve entering the peritoneal cavity, it is less likely to cause damage to the intra-abdominal organs [11] and less likely to cause acute or chronic pain than open repair [13-15].
A novel technique for inguinal hernia repair has been developed at the Hospitals Sousa Martins and São João in Portugal. This technique, known as ONSTEP repair, is an open variation of totally extraperitoneal laparoscopic repair, and involves the placement of a hernia patch in the preperitoneal space during open surgery [16]. The procedure was used in 693 surgeries in 609 hernia patients at the authors’ institutions, and data at 1-year follow-up showed that it produced consistent results with low overall complication and recurrence rates [16]. The present study follows on from the previous 1-year study, reporting long-term (3-5 years) results after ONSTEP inguinal hernia repair in a large series of patients. In particular, it focuses on complications, such as chronic and residual pain, the hernia recurrence rate, and patient satisfaction with the procedure. It involves 450 patients (535 procedures) of the 609 patients (693 procedures) of the initial study, for whom the 3-5 year follow-up was available.
Study population and ethics
Adult patients (≥ 18 years of age) underwent ONSTEP inguinal hernia repair at one of two institutions in Portugal: the Sousa Martins Hospital, Guarda, and the São João Hospital, Porto. All procedures were performed by the two authors over a 5-year period (2007-2011). All patients were rated as American Society of Anaesthesiologists (ASA) grade I, II or III. The study was approved by the Ethics Committee of the Unit of Healthcare of Guarda.
Surgical technique
ONSTEP inguinal hernia repair was performed under local (plus sedation), locoregional or general anaesthesia using a PolySoft™ hernia patch (Davol Inc., Cranston, Rhode Island, USA). This is a self-expanding, non-absorbable sterile mesh consisting of polypropylene monofilaments knitted together to form a strong, porous support material. An interrupted memory recoil ‘ring’ consisting of extruded monofilament polyethylene terephthalate (PET) polymer runs around the edge of the patch to add stability and facilitate placement. The patch is shaped to cover all potential hernia defects and is available in two sizes (Figure 1).
Figure 1: The PolySoft™ hernia patch.
The ONSTEP inguinal hernia repair procedure has been described in detail previously [16]. Briefly, a 4 cm horizontal incision was made in the lower abdomen, and dissection to the level of the internal oblique aponeurosis was performed, followed by development of the operative tissue plane under the external oblique aponeurosis, in order to allow the disruption of the fascia transversalis. Blunt dissection with gauze was then used to create space for insertion of the hernia patch into a part intramuscular part preperitoneal position in the space of Retzius behind the pubic bone (Figure 2).This is a sutureless and tension-free technique which avoids nerve lesions for the nerve exposure to dissection and entrapment is reduced to a minimum. In women, the technique was modified slightly to allow the hernia patch to be placed completely in the preperitoneal space: the preperitoneal dissection was extended laterally, the round ligament lifted and parietalised, and the hernia patch placed completely in the preperitoneal space covering the internal ring from the inside and posteriorly. In all cases, the skin incision was closed using the surgeon’s preferred technique. All procedures were performed on an ambulatory basis.
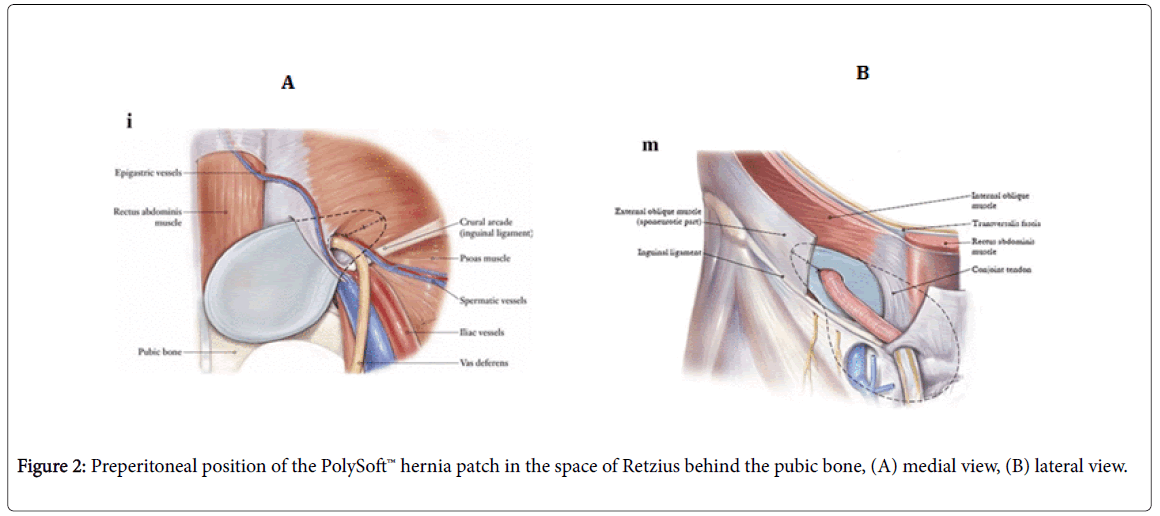
Figure 2: Preperitoneal position of the PolySoft™ hernia patch in the space of Retzius behind the pubic bone, (A) medial view, (B) lateral view.
Follow-up
Patients attended a follow-up visit between 1 and 2 months after surgery, and further follow-up consultation at 1 year. A telephone contact was done by doctors of both Hospitals at 3-5 years after surgery. The patients were asked for any complaints and answered the same protocol used for the evaluation of the results of the first year (Figure 3). If the patients mentioned any complaint they were asked to come to a consultation so that a correct evaluation could be done and a new protocol was filled (Figure 4). Complications, including chronic and residual pain, were noted, as was hernia recurrence. Chronic pain, defined a priori as any pain above 0 on a visual analogue scale (VAS) at or beyond 3 months postoperatively [17], was measured on a VAS scale of 0 to 10, where 0 = no pain, 1-2 = mild pain, 3-5 = moderate pain, 6-8 = severe pain and 9-10 = intolerable pain. Residual pain, defined as pain or discomfort due to the sensation of a foreign body and caused by the pointed distal margin of the ring of the hernia patch, was measured on a similar scale. In addition, patients were asked to rate their satisfaction with the ONSTEP procedure on a scale of 1 to 5, where 1 = poor, 2 = reasonable, 3 = good, 4 = very good and 5 = excellent.
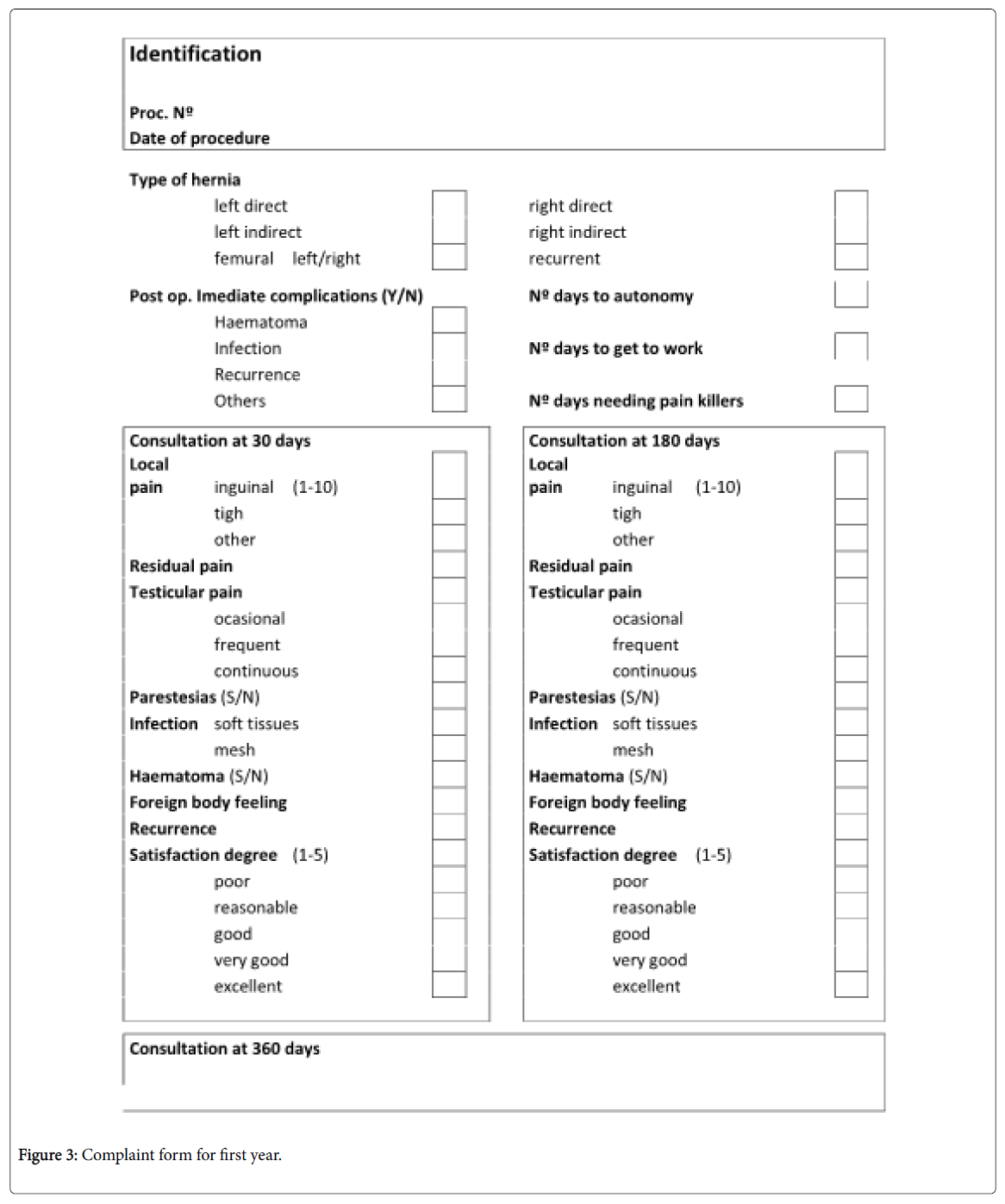
Figure 3: Complaint form for first year.
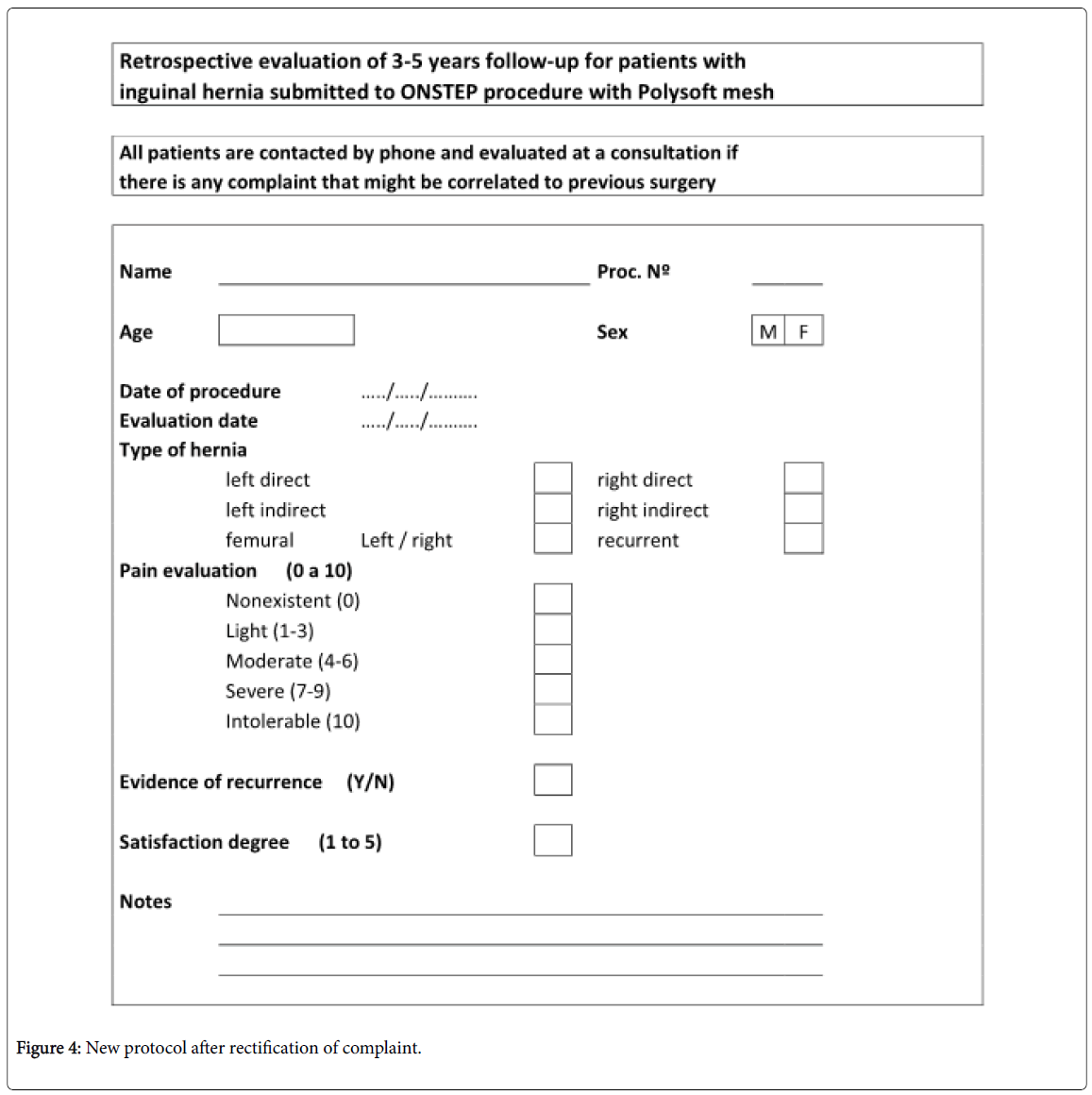
Figure 4: New protocol after rectification of complaint.
Patients and surgical data
From the initial population of 609 patients (693 surgeries) that were evaluated in the study already published in Hernia (2013) it was decided to exclude the years of 2005 and 2006 for difficulties on communication with the patients. A total of 450 patients underwent 535 ONSTEP hernia repair procedures (bilateral repair was counted as two procedures). Data from the 1-year follow-up have already been reported [16]. Data from the 3-5-year follow-up were available from 314 patients (69.8%) and 398 procedures (74.4%). The majority of procedures (68.2%) involved unilateral repair. Patient characteristics and surgical data are summarised in table 1. A total of 114 patients were impossible to contact mostly because of the emigration that arouse Portugal since the economic crisis of 2009 and 22 patients have died for other reasons non concerning the hernia repair procedure they were submitted (Table 1). No anesthetic complications and no surgical deaths were reported. All patients were discharged within 2-23 hours of surgery.
| Characteristic | Value |
|---|---|
| Total number of patients undergoing surgery | 450 |
| Total number of hernia repair procedures | 535 |
| Long-term follow-up | |
| Number of patients who had dieda | 22 |
| Number of patients who were uncontactable | 114 |
| Number of patients with follow-up data, n (%) | 314 (69.8%) |
| Male/female, n (%) | 270/44 (86.0%/14.0%) |
| Mean age (± SD; years)AAA | 59.33 (±7.0) |
| Age range (years) | 18-86 |
| Number of hernia repair procedures (male/female)b | 398 (348/50) |
| Type of hernia repair, n (%) | |
| Bilateral | 84 (26.8%) |
| Unilateral | 214 (68.2%) |
| Femoral | 16 (5.1%) |
| Time to discharge (range in hours) | 2-23 |
Table 1: Characteristics and surgical data for 314 patients undergoing 398 ONSTEP hernia repair procedures. aIn all cases, the cause of death was unrelated to the hernia repair procedure; bBilateral hernia repair was counted as two procedures.
Recurrence
At the 3-5-year follow-up, from 398 procedures, eight patients (five women, three men) had experienced hernia recurrence, giving an overall long-term recurrence rate of 2.0% (95% Confidence Interval: 0.6% to 3.4%) and a recurrence rate of 0.9% for men (3/348).
Complications
All the complications were found and solved in the first year after surgery. At long-term follow-up, there were no cases of chronic pain, 14 cases (3.5%) of residual pain (95% Confidence Interval: 1.7% to 5.3%) and 5 cases (1.3%) of wound infection were found (95% Confidence Interval: 0.2% to 2.4%) (Table 2). There were no cases of mesh infection. Six patients with residual pain (1.5%) had undergone removal of the memory recoil ring around the edge of the mesh to relieve the pain. The remaining eight patients with residual pain did not require further treatment.
| Complication | Number of procedures (%) |
|---|---|
| Chronic pain | 0 (0.0%) |
| Residual pain | 14 (3.5%) |
| Wound infection | 5 (1.3%) |
| Ring removal | 6 (1.5%) |
| Recurrence | 8 (2.0%) |
Table 2: Long-term complications following 398 ONSTEP hernia repair procedures.
The residual pain, more common in skinner patients, results from the stiffness or kinking of the memory recoil ring and can be diminished with a good deployment of the mesh that can be obtained with the right dissection in the external/lateral part very easily. The ring removal should be done by a very short incision focused on the tip, under local anesthesia, never before the fourth month after surgery, and solves the pain immediately after the removal of the ring. There is no need of removing the patch, only the recoil ring. The new ONFLEX mesh, already available, avoids this problem.
Patient satisfaction
Patient satisfaction with the ONSTEP hernia repair procedure was high, with 81.5% of patients rating the repair as ‘excellent’ and 11.5% rating it as ‘very good’. Overall, 94.9% of patients rated the procedure as excellent, very good or good (Figure 5).
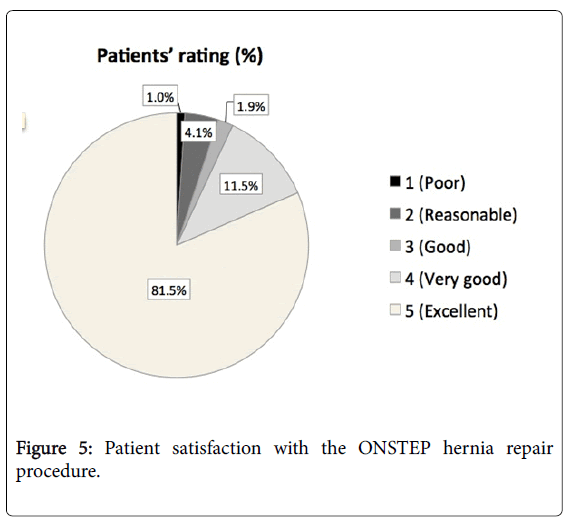
Figure 5: Patient satisfaction with the ONSTEP hernia repair procedure.
This study shows that the novel ONSTEP procedure for inguinal hernia repair produces consistent results in the long-term, with a low recurrence rate, only minor complications and no cases of chronic pain. In a previous series of 693 surgeries in 609 patients followed up for 1 year [16], we showed that the procedure was simple and reliable, and was associated with very low complication and recurrence rates (1.0% and 0.6%, respectively) at this time. In addition, there were no cases of chronic pain and only a few cases of residual pain (0.6% of patients at 6 months, no cases at 1 year). These results were maintained in the current study, if the longer term (3-5 years) is taken into account, with a recurrence rate of 2.0%, no cases of chronic pain and only a few cases (3.5%) of residual pain. The current study also showed that patient satisfaction with the ONSTEP procedure was high, with 95% of patients rating the procedure as excellent, very good or good.
Chronic pain is a serious long-term complication after mesh repair of inguinal hernia. A pooled proportion meta-analysis in a systematic review showed that the incidence of chronic pain after such surgery is 11% [18]. Thus, the lack of any cases of chronic pain in our series of patients should be taken in consideration. In the systematic review, chronic pain was less likely with use of a lightweight high porosity mesh than with use of a heavyweight low porosity mesh (odds ratio 0.61; 95% confidence interval 0.43-0.88). This was attributed to a reduced inflammatory response, reduced scar tissue and greater movement of the abdominal wall with the lightweight mesh. Thus, the 0% incidence of chronic pain in the current study may have been due to the small amount of dissection, the avoidance of nerve dissection, use of a tension-free technique and the lightweight properties of the PolySoft mesh.
Other possible long-term complications with preperitoneal mesh repair include residual pain, and wound or mesh infection. In our series of patients, the most common complications were residual pain and wound infection; no cases of mesh infection were observed. As in our previous report [16], some cases of residual pain (6/14; 42.9%) were cured by removal of the memory recoil ring from the hernia patch, while the pain resolved with no further intervention in the remaining eight patients with residual pain. With the new patch equipped with a reabsorbable memory-ring the problem of residual pain might be solved.
Clinical experience with the ONSTEP technique has also been reported outside of the authors’ institutions in a study of 80 patients undergoing inguinal hernia repair by one of four surgeons in the general surgical department at a Danish hospital [19]. In this study, patients were followed up for a median of 4 months (range 1-13 months). The results showed that 80.3% of patients had no substantial pain-related impairment of daily function, 94.8% were asymptomatic, and 95.5% reported no pain or pain that was easily ignored. All complications were managed conservatively and/or with watchful waiting. It was concluded that the ONSTEP approach is a safe technique for inguinal hernia repair, with no serious postoperative complications and a level of postoperative pain equal to or less than that observed with Lichtenstein repair. The results from the above study [18] were not as promising as those achieved in our series of patients, but this may have been due to the fact that many of the ONSTEP procedures in the Danish study were used for teaching the technique. In addition, a fixed follow-up date was used, thus patients were assessed anywhere between 1 and 13 months after surgery, giving a mix of short- and longer-term results [19,20].
Finally, the recurrence rate in our study was comparable to the recurrence rates reported in the literature for laparoscopic TEP, which range from 0% to around 9% [11,21-28]. Comparison with our 1 year follow-up study indicates that the rate of recurrence decreases with time.
ONSTEP inguinal hernia repair produced consistent results in the long term and was associated with a low recurrence rate and only minor complications, including low levels of residual pain and no evidence of chronic pain. The ONSTEP procedure may offer an alternative approach to both Lichtenstein and laparoscopic inguinal hernia repair. The results from two randomised trials comparing the ONSTEP technique with these procedures are awaited.
The authors would like to acknowledge Ignis Vitae Ltd. for medical writing assistance and Ivan Freud for the illustrations in figure 2, supported by a grant from CR Bard.
Author declares no conflict of interest.