Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2015) Volume 3, Issue 3
Introduction: Gonadotropin-releasing hormone (GnRH) antagonist IVF protocols often induce a significant decrease in serum luteinizing hormone (LH) levels that may affect assisted reproductive technology cycle outcomes. However, supplementing all women undergoing antagonist cycles with recombinant LH does not improve clinical outcomes. The aim of this study was to assess the impact of LH supplementation specifically in those who had low intra-cycle LH levels.
Methods: In this retrospective cohort study, women undergoing IVF/ICSI antagonist cycles had blood tests for LH, oestradiol and progesterone on day 5 of stimulation and then every 1-2 days until the trigger injection leading to egg collection. One group followed the current standard protocol of no LH supplementation given. The other had LH supplementation in the form of either recombinant LH (Luveris; Merck Serono, Switzerland) or urinary human chorionic gonadotropin (hCG) (Pregnyl; MSD, USA) when any intra-cycle blood test showed LH < 1 mIU/.
Results: Between February 2010 and December 2011, 3 groups of women undergoing antagonist cycles were identified: (1) Cycles in which LH ≥ 1 (n = 81), (2) LH < 1 with no supplement given (n = 75) and (3) LH < 1 in which LH supplementation was given (n = 51). There were no significant differences in age, FSH starting dose, days of stimulation, number of embryos transferred, number of embryos frozen or endometrial thickness. Women given LH supplementation had significantly higher peak oestradiol levels. Live birth rates per cycle completed were (1) 43.2%, (2) 30.7% and (3) 45.1%. Women who had adequate LH or were supplemented during antagonist IVF cycles had a significantly better live birth rate (58/132) than women with low LH levels who were not given supplementation (24/75) (p < 0.05).
Conclusion: This study, though relatively small, demonstrated significantly higher live birth rates in women given LH supplementation in antagonist cycles in which their intra-cycle LH levels were very low. Our monitoring indicates this occurs in over half of antagonist cycles. While there is ongoing debate about the potential benefit of LH supplementation, we propose that it is most likely to be useful when cycles are individualized and given when LH levels are shown to be low. More studies to examine this hypothesis are needed.
<Keywords: GnRH antagonist; IVF; Luteinizing hormone supplementation; Live birth rates
Luteinizing hormone (LH) supplementation in IVF cycles has been a debated topic for many years [1-4]. Whilst follicle stimulating hormone (FSH) alone achieves adequate ovarian stimulation it is still possible that, in some circumstances, better results could be achieved with a combined approach [5]. Gonadotropin releasing hormone (GnRH) antagonist IVF cycles have become the cycle protocol of choice in most IVF units. The rapid and profound suppression of the hypothalamic-pituitary axis to prevent the endogenous LH surge reduces the duration and amount of exogenous gonadotropins required for stimulation [6], with lower rates of ovarian hyperstimulation syndrome [7] and excellent overall IVF outcomes [8]
At IVFAustralia, where LH levels are routinely assessed during all cycle monitoring blood tests, it has been observed that many women experience significant collapse of their LH levels when they start the antagonist. Low concentrations of LH can result in a reduction in ovarian oestradiol biosynthesis [6], a reduction in high-quality embryos for cryopreservation [7], reduced implantation and pregnancy rates [3,4,8], lower live birth rates [3,9], increased miscarriage rates [10] and disturbed endometrial maturation [11]. At the other extreme, elevated LH concentrations have been associated with poor fertilization, poor implantation and detrimental effects on pregnancy rates [5]. It has been hypothesized that there is a ‘therapeutic LH window’ which may produce best overall outcomes [10-13].
In apparent contradiction to these findings, recent reviews have concluded that there is no association between LH levels and pregnancy outcomes [3,14-17]. The utility of these findings can be questioned, as LH levels were assessed as quartiles rather than actual concentrations [15,17], and the measurement of LH was performed on only one day during stimulation [15]. Observations of LH levels in IVFAustralia indicate a highly variable response to the antagonist, both in timing and magnitude. Thus we hypothesize that it is still indeed possible for either excessive or insufficient expression of LH during GnRH antagonist administration to affect outcomes.
Trials of LH supplementation in IVF cycles have so far shown little or no improvement in pregnancy outcomes [2,4,18-20]. However, these trials randomized patients to LH supplementation prior to the start of a cycle, without consideration of the individual dynamic hormone changes that occur during stimulation. According to the “therapeutic LH window” hypothesis, any potential benefits of supplementing women with low LH levels may be counter-balanced by a detriment to supplementing those with normal or even high levels. Furthermore, the majority of these studies used the agonist protocol [5] in which endogenous LH levels are not as profoundly suppressed as in antagonist protocols [21]. Studies investigating the role of LH supplementation in antagonist protocols have also failed to identify a beneficial effect overall [22-24]. It has been claimed that there may be benefit in certain subgroups such as older women and poor responders (possibly due to the low bioactivity of LH in those subgroups) [25], although a recent randomized control trial in women over 35 did not show benefit with supplementation [20]. In the latter study, LH levels at baseline and during stimulation were not assessed, and supplementation was given in the form of Pergoveris (Merck Serono, USA) which would have produced highly variable doses of LH depending on the dose of FSH given.
The concept of variable LH levels and responses was illustrated in a trial by Propst et al. [26]. They compared 113 women given FSH stimulation alone with 126 women given FSH supplemented with urinary human chorionic gonadotropin (hCG) (Pregnyl) as a form of LH activity. Initial analysis demonstrated no difference in outcomes. However when only those who had LH levels
We hypothesized that very low LH levels during IVF antagonist cycles do adversely affect outcome, and that supplementation targeted to those women would improve success rates. The aim of this study was to compare 2 clinical approaches – to give LH supplementation or not based on intra-cycle LH monitoring.
Study design
This single centre retrospective cohort study was conducted from February 2010 until December 2011. All women undergoing antagonist cycles under the care of two clinicians practising in the same location within IVFAustralia were enrolled. Cycles were performed and monitored through IVFAustralia as per routine protocols. One clinician (clinician with LH supplementation), however, gave LH supplementation whenever LH levels fell below 1 IU/mL at any time after initiation of GnRH antagonist and before the administration of the hCG trigger, while the other clinician (clinician with no LH supplementation) did not. The 2 clinicians worked in the same location over the same time period, and used the same IVFAustralia monitoring, scanning, clinical and laboratory protocols and facilities. Patients were retrospectively stratified into 3 independent groups based on trough levels of serum LH concentrations and use of exogenous LH supplementation. Group 1 consisted of cycles in which trough LH levels remained ≥ 1 IU/mL, group 2 consisted of cycles in which trough LH levels fell to <1 IU/mL with no supplement given, and group 3 consisted of cycles in which trough LH levels fell to <1 IU/mL and LH supplementation was given.
Patients
230 antagonist cycles were identified. 23 were excluded from analysis for incomplete or missing data (15 cycles), no eggs collected (2 cycles), no embryo transferred (2 cycles), and violation of the group allocation criteria (1 cycle). The remaining 207 cycles were allocated to the 3 groups as shown in Figure 1.
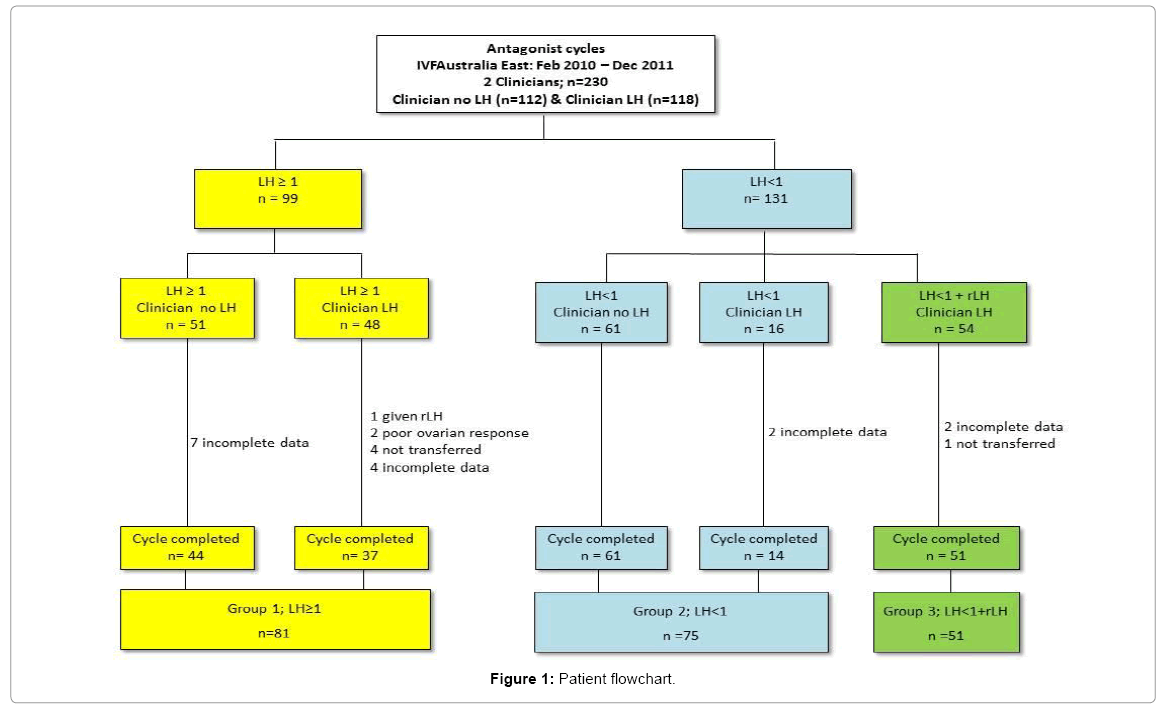
Figure 1: Patient flowchart.
Protocol
The antagonist IVF protocol at IVFAustralia involved starting FSH stimulation on day 2-3 after the start of menses. All patients received recombinant FSH with either Gonal-F (Merck Serono, Australia) or Puregon (MSD, Australia) with starting dose decided by their clinician. In most cases the dose was constant throughout, but dose adjustment was sometimes made on clinical criteria. Cycle monitoring was performed from day 5 and thereafter every 1-2 days by serum oestradiol, LH and progesterone levels, and pelvic ultrasound scan. An LH value <1 mIU/ml – lower case l for all at any time after initiation of GnRH antagonist and before the administration of hCG trigger qualified the patient to have low LH (Group 2 and Group 3). The cutoff for low LH was chosen as it is the defining concentration for the diagnosis for World Health Organization (WHO) type I anovulation [27]. The LH assay at IVFAustralia was assessed against the WHO second international standard 80/552 and had an assay sensitivity of 0.07 IU/L. The intra- and inter-assay coefficients of variation (CVs) for LH were <5.6% and <7.2% in the range of concentrations measured in this study.
Patients in group 3 received a daily injection of 75 IU recombinant LH (Luveris; Merck Serono, Switzerland) or 150 IU chorionic gonadotropin (Pregnyl; MSD, USA) every 3 days. The LH supplementation was continued concomitantly with FSH until the trigger injection prior to egg collection.
The trigger injection of 250 μg of hCG (Ovidrel; Merck Serono, Switzerland) was given when at least three follicles were greater or equal to 17 mm in diameter, and oocyte retrieval was performed 36 h later. Embryos were frozen and transferred at day 5. The luteal phase was supported by vaginal progesterone pessaries 400 mg/day (Utrogestan; Besins International, France).
Objectives and outcomes
The objective of this study was to assess the ovarian response in LH deficient patients undergoing antagonist cycles, comparing stimulation with recombinant FSH combined with LH supplementation (Luveris or Pregnyl) to recombinant FSH alone. The primary outcome of the study was live birth rates. Secondary outcomes were peak oestradiol levels, number of eggs collected, number of embryos transferred and frozen and endometrial thickness. Data were collected from patient records using the online IVFAustralia database and patient notes.
The study was approved by the Research and Development Committee of IVFAustralia.
Statistical analysis
Due to the retrospective nature of this study, a power analysis was not performed. All statistical analyses were performed using SPSS 20 statistical package for Windows (SPSS, Inc). Results are expressed as mean +/- standard deviation. Exploratory analysis was initially performed to determine normality of the data. Chi-square tests, Student’s t-tests, Fisher’s exact tests and one-way analysis of variance (ANOVA) were used where appropriate. A p-value <0.05 was considered statistically significant.
A total of 207 IVF cycles between February 2010 and December 2011 were analysed. 81 cycles had trough LH ≥ 1 (group 1) and 126 cycles had LH < 1 (groups 2 and 3). Of the women with trough LH < 1, 51 received LH supplementation (group 3) and 75 did not (group 2). The three study groups were comparable for age, FSH starting dose, number of embryos transferred, number of embryos frozen and endometrial thickness (Table 1). Group 1 had slightly shorter mean duration of FSH stimulation. Patients who were supplemented with LH (group 3) had significantly higher peak serum oestradiol levels compared to patients who did not receive supplementation (group 2). Patients with elevated LH levels (group 1) had significantly fewer eggs collected compared to both other groups, although there were no differences in numbers of embryos transferred or frozen. Live birth rates per cycle were 43.2% (group 1), 30.7% (group 2) and 45.1% (group 3).
| Group 1 LH≥1 n =81 |
Group 2 LH<1 n=75 |
Group 3 LH<1+LH supplement (n=51) |
|
|---|---|---|---|
| Age | 36.5 (4.5) |
36 (5.2) |
35.5 (5.2) |
| FSH starting dose | 215.3 (117.4) |
213.3 (109.2) |
180.9 (110.2) |
| Days of stimulation | 11.4 (2.2) |
12.3*1 (2.3) |
12.1 (2.2) |
| Peak oestradiol | 6600 (3818.9) |
5785 (2918) |
7616*2 (5596.5) |
| Eggs collected | 8.9 (5.1) |
11.4*1 (7.0) |
12.6*3 (7.8) |
| Embryos transferred | 1.18 (0.4) |
1.2 (0.4) |
1.4 (0.5) |
| Embryos frozen | 1.1 (1.6) |
1.4 (2.1) |
1.1 (1.4) |
| Endometrial thickness | 10 (2.1) |
10.5 (1.9) |
9.8 (2) |
| Clinical Pregnancy rate | 44.4% (36/81) |
32% (24/75) |
49% (25/51) |
| Live birth rate | 43.2% (35/81) |
30.7% (23/75) |
45.1% (23/51) |
Results expressed as mean (standard deviation) unless otherwise shown.
*one-way ANOVA. The post hoc Fisher least-significant-difference method tested for differences between group
*1p<0.05 for difference between groups 1 and 2
*2p<0.05 for difference between groups 2 and 3
*3p<0.05 for difference between groups 1 and 3
Table 1: Overall cycle details and outcomes.
A comparison between the clinician with no LH supplementation (105 cycles) and the clinician with LH supplementation (102 cycles) is shown in Table 2. Overall there were no significant differences in age, FSH starting dose, days of stimulation, number of eggs collected, number of embryos transferred, number of embryos frozen or endometrial thickness. The live birth rate for the clinician with LH supplementation was 42% compared to 36% for the clinician with no LH supplementation. In a subgroup analysis of those cycles with LH levels ≥ 1 (group 1: identical management for both clinicians), live birth rates were 38% for clinician with LH supplementation and 48% for clinician with no LH supplementation.
| Total | Group 1 (LH≥1) |
Group 2 (LH<1) |
Group 3 (LH supp) |
||||
|---|---|---|---|---|---|---|---|
| Clinician | no LH n=105 |
LH n=102 |
no LH n= 44 |
LH n=37 |
no LH n=61 |
LH n=14 |
LH n=51 |
| Age | 35.5 (4.9) |
36.7 (4.2) |
35.2 (4.2) |
38 (4.5) |
35.7 (5.5) |
37.1 (4.1) |
35.5 (3.74) |
| FSH starting dose | 204.2 (104.8) |
208 (121.6) |
196* (103.4) |
237.9* (130) |
210 (106.3) |
227.7 (124.2) |
180.9 (110.2) |
| Days of stimulation | 11.8 (2.23) |
11.9 (2.3) |
11.4 (2.36) |
11.4 (2.12) |
12.2 (2.08) |
12.5 (3.1) |
12.1 (2.22) |
| Peak oestradiol | 6027.6 (3046) |
7098 (4915) |
6590.5 (3470.5) |
6611.9 (4245.3) |
5621.7 (2655.3) |
6498.86 (3905.5) |
7616 (5596.5) |
| Eggs collected | 10 (5.7) |
11.4 (7.6) |
8.7 (4.9) |
9.1 (5.5) |
11 (6.13) |
13.3 (10) |
12.6 (7.8) |
| Embryos transferred |
1.2 (0.36) |
1.3 (0.5) |
1.1 (0.32) |
1.3 (0.5) |
1.18 (0.39) |
1.36 (0.5) |
1.35 (0.48) |
| Embryos frozen | 1.2 (1.8) |
1.2 (1.7) |
1.1 (1.56) |
1.1 (1.7) |
1.34 (2.01) |
1.8 (2.6) |
1.12 (1.42) |
| Endometrial thickness | 10.6 (1.9) |
9.7 (2.0) |
10.45 (2.3) |
9.54 (1.8) |
10.7 (1.6) |
9.9 (2.7) |
9.8 (2) |
| Clinical Pregnancy rate | 38% (40/105) |
44% (45/102) |
50% (22/44) |
37.8% (14/37) |
29.5% (18/61) |
42.9% (6/14) |
49% (25/51) |
| Live birth rate | 36% (38/105) |
42% (43/102) |
47.7% (21/44) |
37.8% (14/37) |
27.9% (17/61) |
42.9% (6/14) |
45.1% (23/51) |
Results expressed as mean (standard deviation) unless otherwise shown.
*Pearson chi squared test; p < 0.05 (Group1: A versus B)
Table 2: Cycle details and outcomes by treating clinician.
When women with adequate or supplemented LH levels were combined (groups 1 and 3) there was a significant improvement in live birth rate (44%) compared with women with low LH who were not supplemented (group 2) (31%) (Table 3). Peak serum oestradiol was also significantly higher in women with adequate LH or receiving LH supplementation but there were no other significant differences between the groups.
| Groups 1 and 3 LH≥1 andLH<1+LH supplementation (n= 132) |
Group 2 LH<1 (n=75) |
|
|---|---|---|
| Age | 36.1 (4.25) |
36 (5.2) |
| FSH starting dose | 202 (115.5) |
213 (109.2) |
| Days of stimulation | 11.7 (2.3) |
12.3 (2.3) |
| Peak oestradiol | 6992.7° (4594.2) |
5785.4° (2918) |
| Eggs collected | 10.3 (6.6) |
11.4 (7) |
| Embryos transferred | 1.2 (0.4) |
1.2 (0.4) |
| Embryos frozen | 1.1 (1.6) |
1.4 (2.1) |
| Endometrial thickness | 9.9 (2) |
10.5 (1.9) |
| Clinical Pregnancy rate | 46.2%* (61/132) |
32%* (24/75) |
| Live birth rate | 44%* (58/132) |
30.6%* (23/75) |
Results expressed as mean (standard deviation) unless otherwise shown.
°t test for equality of means; p < 0.05
*Fisher’s exact test (1 tailed); p < 0.05
Table 3: Cycle details and outcomes by LH level.
The trough LH level was assessed by dividing women with low LH levels into those < 0.5 IU/mL and 0.6-1 IU/ml (Table 4). LH supplementation improved livebirth rates in both groups, although the improvement only reached statistical significance in the < 0.5 IU/mL group.
| LH≤0.5 | LH 0.6-1 | |||
|---|---|---|---|---|
| Group 2 No supplement n=48 |
Group 3 LH supplement n=31 |
Group 2 No supplement n=27 |
Group 3 LH supplement n=20 |
|
| Age | 36.8 (5.1) |
35.1 (3.6) |
34.5 (5.3) |
36.3 (3.9) |
| FSH starting dose | 231* (119) |
155* (78) |
181.9 (82.4) |
220.6 (140) |
| Days of stimulation | 12.4 (2.2) |
12 (2.1) |
12 (2.5) |
12.3 (2.5) |
| Peak oestradiol | 5157* (2377.2) |
8493* (6738) |
6902.6 (3463.3) |
6256.3 (2745) |
| Eggs collected | 11.5 (6.6) |
12.3 (8.5) |
11.4 (7.8) |
13.23 (6.8) |
| Embryos transferred |
1.3 (0.4) |
1.3 (0.5) |
1.1 (0.4) |
1.4 (0.5) |
| Embryos frozen | 1.4 (2.3) |
1.1 (1.4) |
1.4 (1.8) |
1.1 (1.5) |
| Endometrial thickness | 10.4 (1.7) |
9.8 (2.1) |
10.7 (2.3) |
9.9 (1.8) |
| Clinical Pregnancy rate | 15/48° 31.3% |
15/31° 48.4% |
9/27 33.3% |
10/20 50% |
| Live birth rate | 14/48° 29.2% |
14/31° 45.2% |
9/27 33.3% |
8/20 40% |
Results expressed as mean (standard deviation) unless otherwise shown
*t test for equality of the means; p < 0.05 (LH ≤ 0.5 Group 2 vs. Group3)
°Levene’s test for equality of variances (independent samples test); p < 0.05 (LH
≤ 0.5 Group 2 vs. Group3)
Table 4: Cycle details and outcomes comparing low and very low LH levels.
Of the patients receiving supplemental LH (group 3), 20 cases were given urinary HCG (Pregnyl), with a pregnancy rate of 55% while 31 cases were given recombinant LH (Luveris) with a pregnancy rate of 38.7%. Although there were no statistically significant differences between these groups, women taking pregnyl were younger, had lower FSH starting doses, higher peak oestradiol levels and had more embryos transferred and frozen.
Using daily dosing of luveris as a measure, the variation of duration of treatment with LH supplementation is shown in figure 2. With an overall median of FSH stimulation of 12 days, the median for women receiving Luveris was for 5 days. However, there was a significant range of Luveris use of 1-9 days.
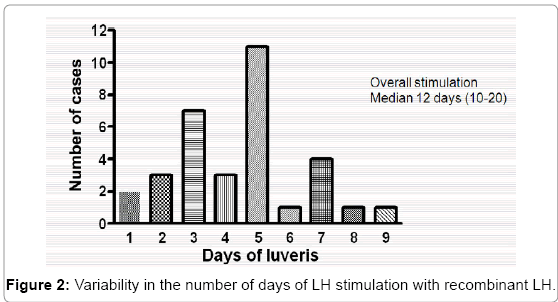
Figure 2: Variability in the number of days of LH stimulation with recombinant LH.
This study supports the hypothesis that exogenous LH supplementation in the form of HCG (Pregnyl) or recombinant LH (luveris) improves both clinical pregnancy rates and live birth rates in a specific subset of women undergoing antagonist IVF cycles with low intra-cycle levels of serum LH. The effect was only significant when LH ≤ 0.5. To our knowledge, this protocol for LH supplementation has not been reported before. The principle of targeting supplementary LH to those with low LH levels is consistent with a previous study [26] and may explain the apparent benefit in subgroups of IVF patients (poor responders [28] and older women [29]) who may experience a more profound LH fall during the administration of the antagonist.
Women with low intra-cycle LH levels (not supplemented) had lower peak oestradiol levels, reduced clinical pregnancy rates and reduced live birth rates when compared to those with adequate LH levels (whether endogenous LH or supplemented LH). This supports previous suggestions of impaired adequate oestradiol synthesis and decreased fertilisation rates in profound suppression of peripheral LH activity [30-33]. Furthermore, our results suggest that this negative impact can be overcome through supplementing these women with LH, as shown by a trend towards increasing serum oestradiol, clinical pregnancy rates and live birth rates in the supplemented cycles. However, this trend was only significant in the subset of cycles with LH ≤ 0.5.
This study also supports the concept of a potential LH threshold below which IVF success rates are adversely affected [12,13]. It is well established through treatment of patients with hypogonadotropic hypogonadism that small amounts of LH are necessary to promote adequate oestradiol secretion and to allow the follicle to luteinise when exposed to HCG. It is not known if LH acts to increase the quality of the oocytes or acts on the endometrium to increase the likelihood of implantation. Nevertheless, the use of LH supplementation in ART has been thought non-essential in achieving successful outcomes, and has not been routinely used in IVF cycles. This is thought to be due to adequate resting levels of LH despite pituitary downregulation [34]. Most current evidence suggests that supplementation of LH does not affect pregnancy rates [3-5,14-16,18,19]. However these studies did not specifically target women with evidence of deficient LH levels, the main group of interest in our study. A standardised approach to supplementing all women with LH would not take into account the ‘therapeutic LH window’. Currently we do not know why some women experience more profound suppression of their LH levels from the antagonist than others. Women randomized to receive treatment based on pre-stimulation LH levels would fail to account for the individualised response. The unpredictable timing of the fall in LH levels makes it impossible to identify a specific day within the cycle which can accurately identify trough LH levels. The variation was illustrated in Figure 2, where Luveris administration started when LH < 1 varied between 1 and 9 days. Regular intra-cycle LH monitoring would be necessary to identify patients whose LH levels are suppressed by the antagonist.
There is no universal agreement on the lower level of LH concentrations which define the LH threshold. Although our data indicates the most significant adverse effects occur at an LH threshold of ≤ 0.5, cycles with modestly low LH levels (<1) also demonstrated adverse outcomes. Prior studies have indicated the lower limit of the LH threshold to be between 0.5 and 1.2 [9,33,35], which is in agreement with our findings.
We observed fewer eggs retrieved in cycles with adequate LH levels compared to cycles with low LH levels, consistent with other studies [26]. This reduction in oocyte retrieval did not affect embryo yield or quality, as there was no impact on the number of embryos frozen or transferred, and live birth rates actually improved. One explanation could be that LH may result in fewer but more reproductively competent oocytes through stimulation of the LH receptor. Eggs retrieved from cycles with LH supplementation are also shown to be of higher quality with improved fertilisation, implantation and pregnancy rates [36].
LH has been implicated in regulating the endometrium with subsequent improvements in implantation. The LH receptor has been identified in the endometrium, and increases during the implantation window [26]. Our data failed to find a difference in endometrial thickness between groups by LH levels, thus we are unable to comment on the effect of LH on the endometrium.
This study used two different forms of LH supplementation, 75 IU daily of luveris (recombinant LH) and 150 IU every 3 days of Pregnyl (hCG). The choice of LH supplementation was based largely on availability and patient affordability. Both LH and hCG have the same alpha subunit, and both bind to and activate the LH/hCG receptor. However, the beta subunit of hCG has a different structure and glycosylation pattern resulting in a sixfold affinity for the LH/hCG receptor and a longer half-life [29]. In terms of bioequivalence, 10 IU of hCG are roughly equivalent to 75 IU of LH. By giving an equivalent of 50 IU daily dose of hCG, it is 5 times more than LH dose. The “suboptimal” LH dose could partially explain the lower live birth rate in the patients receiving luveris over pregnyl (39% vs 55%). Moreover, the half-life of luveris might not be sufficient to cover 24 hours, resulting in insufficient LH activity supplementation. However, although the numbers are small, the pregnyl group was slightly younger (34.9 years vs. 36.1 years) and had slightly higher numbers of embryos transferred (1.5 v 1.2).
A significant strength of this study is the use of the clinically relevant endpoint of live birth rates as a primary outcome. The majority of research in this area does not provide live birth rates, rather using follicular development [28], implantation rates [21], clinical pregnancy rates [26] or pregnancy rates beyond 12 weeks [2] as primary outcomes. Nevertheless this study does have significant limitations and interpretation requires a degree of caution. It was a small retrospective study and the groups were not randomised. Treatment with the LH supplementary protocol was based on whether the patients came from one referring clinician or another. Comparison between clinicians is particularly problematic. Bias in this study was minimised by both clinicians working in the same rooms, using the same IVFAustralia protocols for monitoring, and using the same IVFAustralia laboratory. Indeed it was shown that there was, overall, no difference between groups of patients recruited by the clinicians in terms of patient age, starting FSH dose, number of eggs collected, number of embryos transferred and frozen, and pregnancy outcomes. A more direct comparison was possible in women with LH ≥ 1 throughout the cycle (no LH supplement given by either clinician) and although clinician with LH supplementation gave a slightly higher starting FSH dose, all other variables were not significantly different. Of note, the clinician with no LH supplementation had live birth rates of 48% compared to the clinician with LH supplementation of 38% within the LH ≥ 1 cohort. This difference is important because the clinician with LH supplementation had patients allocated to the LH supplement group, while the clinician with no LH supplementation did not. As LH supplementation in low LH cycles appeared to be particularly beneficial, there is no evidence that the outcome was influenced by clinician-specific factors and success rates.
A recent literature review suggested that only 10-12% of IVF cycles lack adequate endogenous LH concentrations after pituitary downregulation [1]. The current study, using frequent LH intracycle LH assessment, showed that a deficient level of LH occurs in as many as 50% of antagonist cycles. There is therefore a large group of women who may benefit from LH supplementation. Our study, whilst limited in its design and size, does raise the possibility that LH supplementation in IVF antagonist cycles may be beneficial if targeted towards the right patients. IVF success rates are high, but certainly not high enough for women who often have to undergo significant physical, emotional and financial stress of repeated cycles. This study indicates potentially improved success rates with a more individualised approach of using intra-cycle LH monitoring to determine whether to give LH supplementation or not. Whilst creating a truly randomised trial in this context is more difficult, it would provide a clearer answer than the current ‘all or none’ treatment trials of LH supplementation performed so far.
GS and GH have been sponsored for educational events by both Merck Serono (Luveris) and MSD (Pregnyl). Luveris was supplied for no charge to the patients, but Merck Serono played no part in the design, implementation or analysis of the study.