Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Protocols - (2013) Volume 3, Issue 6
In their natural state within the body, normal cells use cellular respiration as their main source of ATP and energy. Carbohydrate deprived cells easily depend on the resulting ketone bodies for an alternative energy source. This natural evolutionary adaptation to starvation allows for survival of normal cells during times of fasting or famine. Cancer cells in contrast are defective in this respect, lacking the ability to utilize ketone bodies for energy and depend heavily on glycolysis for survival. The pancreas senses increased carbohydrate intake resulting in increased insulin secretion. Normal growth throughout the body depends on insulin, which by itself is also a potent growth factor which binds to cell membrane insulin receptors and stimulates mitosis via signal transduction and DNA synthesis, resulting in less
apoptosis or tumor cell death. Consequentially, carbohydrate restriction will increase tumor cell destruction. We are conducting a pilot study to examine the safety and tolerability of the ketogenic diet KD in patients with advanced cancer within the Veteran Affairs Pittsburgh Healthcare System (VAPHS) oncology patient population.
We plan to recruit 10-20 patients with advanced or metastatic cancer from the VAPHS outpatient Medical Oncology clinic. These recruits may have no previous chemotherapy, may have progressed on chemotherapy, or may be on chemotherapy break. They must possess a performance status of at least Karnofsky Score 1 and measurable solid disease detectable on Positron Emission Tomography PETComputerized Tomography CT imaging [1].
Patients with documented brain metastasis are excluded, however those with primary brain tumors are allowed. The reason for this was to exclude patients with short life expectancy (less than 12 weeks) however primary brain tumors were included because of previous positive cases responding to low carbohydrate diets. Because primary brain tumors depend heavily on glucose they are theoretically expected to respond well to the diet [2-4], whereas sparse data exist for metastatic brain tumors of other histology. Other exclusions are significant cardiac, renal or neurologic comorbidities, or an active state of malnutrition. Our trial registered on the ClinicalTrials.gov website (trial ID NCT 11416468) after approval from our internal Institutional Review Board.
A 3-day trial of the diet under detailed individualized guidance of the dietician will occur. Preferably the candidate must be highly motivated, and must have strong family support. Patients who already had baseline scans within 30 days prior to starting the diet did not need a scan. If possible, it is best to screen the tumors before diet initiation. The three-day diet trial might significantly influence the PET/CT data. A surgical biopsy specimen taken before diet initiation might also be good. Seyfried et al. found in their preliminary trial in the Dominican Republic that the restricted ketogenic diet could change tumor pathology over the short term. It is best therefore to get images and pathology before implementation of diet therapy. If after the trial the patient reports good compliance, a screening PET/CT scan will be obtained as a baseline to document that the tumors are F-18 Fluoro- Deoxy-Glucose (FDG) avid and serum ketones drawn to show that the body has indeed entered a state of ketosis Serum ketone measurements would also need to be obtained before diet initiation, if possible. If no ketosis is seen initially, subsequent evaluations done on a monthly basis will monitor compliance and if 2 successive tests show absence of ketosis, the candidate will face possible removal from the trial. Refined starches and food with high sugar or starch content will be highly discouraged and food portions will be measured daily in accordance with the dietician’s weekly advice.
A low carbohydrate (<20 g/day) diet will be prescribed for the initial 4 weeks of induction. Patients are encouraged to eat high protein foods such as meat, poultry, eggs, cheese and avoid carbohydrate rich food containing sugars, pasta, rice and starchy vegetables such as potatoes or sweet fruits but their total calories were measured carefully based on their ideal body mass index. After 4 weeks the diet may be advanced to as much as 40 g/day as long as the patient remains in at least a state of trace ketosis and their caloric limit is achieved.
The above initiation diet is more of an Atkins Diet (AD) than a ketogenic. The KD differs from the AD in containing lower total protein and higher fat. The KD usually contains a Fat/carbohydrate + protein ratio of 3:1 or 4:1. We prefer to initiate the diet therapy with a 48 hr “water only” therapeutic fast but did not require this for fear that it will discourage patients from enrolling. The water only fast helps patients make the transition from a high carbohydrate diet to a KD. This will enhance the use of ketone bodies for energy when the ketogenic diet is initiated. Also, we felt that a modified Atkins type of ketogenic diet would be more acceptable to patients and decrease dropouts. KD diets should never be consumed in unrestricted amounts. The best effects are seen with blood ketone levels in the 3-5 mmol range. We have not seen therapeutic efficacy in cancer patients with only trace increases in ketones. Seyfried et al., have developed a new Glucose/Ketone (G/K) Index to assess therapeutic efficacy of the KD. They find that a G/K index of 1.0 or below predicts good efficacy for most people.
Baseline physical exam, serum ketones, complete blood count with differential, urinalysis, and a comprehensive metabolic and lipid profile will be done at baseline and at least monthly. PET/CT imaging will be performed at baseline, 4, 8 and then every 2 months till 16 weeks total while in the trial.
The EORTC QLQ-C30 (version 3) questionnaire addresses lifestyle and health issues and is completed at study entry, Week 4, 8, 12 and 16. This questionnaire addresses the domains of social and physical functioning [5].
Major concerns with the use of this type of dietary intervention lie in the possibility of unwanted weight loss in an already fragile cancer patient population. We have discussed the weight loss issue with many physician groups. There are at least three main causes of weight loss, two of which are pathological. Some cancer patients will lose weight because of cancer cachexia. This is a pathological weight loss due to the influence of the tumor on energy stores in muscle tissue. Cachexia is a type of pathological starvation and is very unhealthy. Some cancer patients will lose weight from the toxic effects of chemotherapy. This is also considered a type of pathological weight loss due to the poisonous effects of radiation or chemotherapy. The weight loss associated with the restricted ketogenic Diet (KD-R) is considered healthy weight loss. Elevated ketones will enhance the metabolic efficiency of most normal cells within the body. There are numerous examples of the health benefits from KD weight loss. We would therefore not be concerned with weight loss while patients are on the KD. Most of the KD patients we know of lose weight initially, but then the weight stabilizes at a new healthy level.
The impact of the diet on the lipid profile is also another concern. This is a concern only if the patient eats too much of the KD. Blood lipid profiles become very healthy when the KD is consumed in restricted amounts. We have seen this in both mice and humans.
Increased incidence of gout and kidney stones are known long term side effects. This is also associated with excessive consumption or with KDs that are nutritionally imbalanced). Anyone experiencing a weight loss of more than 10-12% will be evaluated closely for possible termination from the study. Because of the short duration of the trial it is unlikely that formation of kidney stones will occur. Symptomatic hyperuricemia and hyperlipidemia will be managed with medication i.e., Allopurinol and statins as needed. It is also necessary to increase salt content when blood ketones enter the therapeutic zone (3-6 mmol). This will offset electrolyte loss from urination.
Warburg et al., in 1956 postulated that cancer is caused by an irreversible damage to cellular respiration, which in turn drives cells to depend on glycolysis as their major source of energy even in oxygen rich conditions. He described tumors as being lactate rich and highly dependent on glucose [6]. Unlike normal cells, cancer cells, through the accumulation of mutations and gene rearrangements lost the flexibility to adapt to stress. This results in an inability to use ketones for energy. A calorically restricted diet will stress tumors into cell destruction and death by decreasing glucose and increasing ketone body levels. Most human tumors take up more glucose than their surrounding normal tissues. By using positron emission tomography with F-18 Fluorodeoxy- glucose, FDG-PET scans are used to detect and monitor tumor response to chemotherapy or radiation. The ketogenic diet has been in use for decades in the treatment of refractory epilepsy for which it appears to be safe as well as very effective. A previous pilot study showed tolerability of a similar diet in 10 human cancer subjects for up to 4 weeks, while another study involving 16 patients showed 5 patients completing up to 12 weeks on the diet [7,8].
The ketogenic diet, a diet low in carbohydrates but high in fats and (moderate) protein, is widely used in the treatment of epilepsy and is considered safe in the long term. There is increasing evidence to suggest that this dietary approach may be beneficial to control of tumor growth and progression.
Tumor cell lines of colon, breast, gastric and prostate cancer, and both animal and human cancer subjects showed tumor stability or shrinkage on low carbohydrate diets or conditions of low glucose/ glutamine [7-11]. In- vitro exposure of tumor cells to glycolytic inhibitors also decreased cell proliferation and survival, as well as increased cell necrosis [12-14]. The exposure of tumor cells to D-beta -hydroxybutyrate inhibited cell proliferation but not cell viability in transformed (Raji) lymphoblast cell lines [15]. We have new evidence showing that ketone esters can be toxic to metastatic cancer cells.
Melanoma mice models placed on a ketone producing diet decreased their number of lung metastases by two thirds [15]. Genetically engineered mouse models of breast cancer, fed low CHO diets were compared to mice fed western diets. The low CHO fed mice exceeded their normal life span with disappearance or shrinkage of their tumors disappear while nearly all but one mouse on the western diet died early [16]. Human brain cancer case studies exhibited tumor stability and regression while on the diet [2,3].
While weight loss in already compromised cancer patients is a concern, studies in obesity patients showed that weight loss with a low carbohydrate diet occurred within the first 6 months but tapered off with the difference being insignificant at one year. In a comparison study between the low fat, energy restricted diets versus the low carbohydrate non energy restricted diet, weight loss was comparable and the levels of high density lipoprotein cholesterol were higher and triglyceride levels were lower in the low carbohydrate ketogenic diet group which was favorable hence at least comparable [17].
Cancer cells are highly dependent on glycolysis as their key source of energy, even under an aerobic environment. Dysregulation of glycolytic enzymes such as Hexokinase 2 (HK2), Lactate Dehydrogenase-A (LDH-A), Phosphofructokinase (PFK) and Pyruvate Kinase-M2 (PK-M2) as well as certain defects within the enzymes of the Tricarboxylic Acid Cycle (TCA) lead to decreased ATP production via decreased oxidative phosphorylation and up-regulation of glycolysis. Proapoptotic factors Bax and Bad are inhibited and Hypoxia Inducible Factor 1-alpha (HIF-1alpha) is up-regulated resulting in less cell death. High carbohydrate intake and elevated blood glucose lead to increased free Insulin growth factor -1 and insulin, which by activating the insulin growth factor-1R/Phosphatidylinositol 3-kinase/ Ak-thymoma/mammalian target of rapamycin (IGF1R-IR/PI3K/Akt/mTOR) intracellular signaling pathway, inhibit apoptosis and promote cell growth and proliferation (Figure 1).
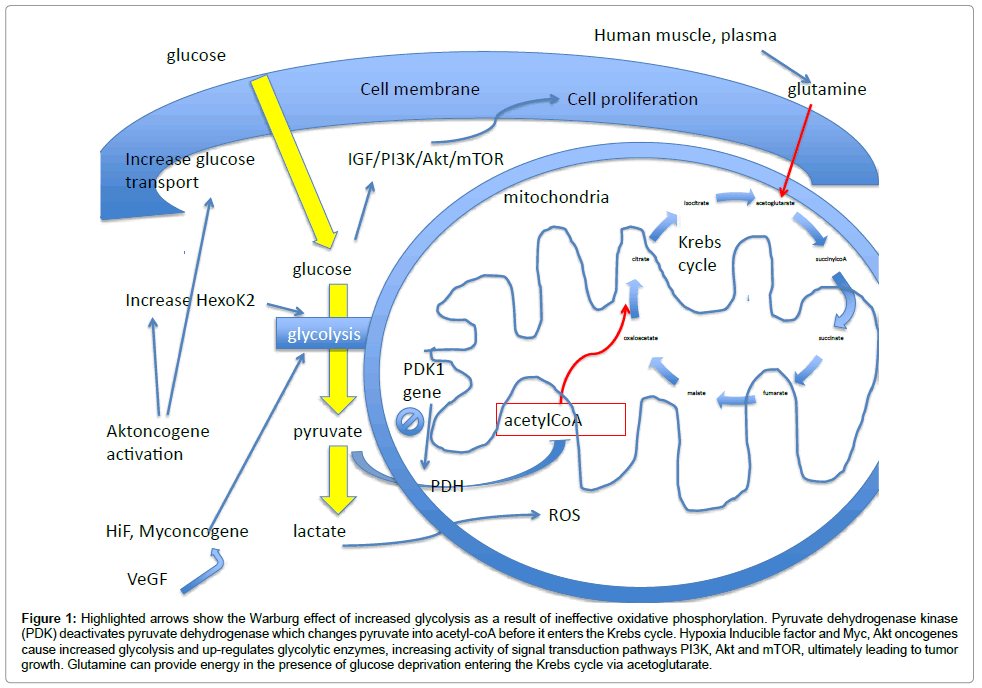
Figure 1: Highlighted arrows show the Warburg effect of increased glycolysis as a result of ineffective oxidative phosphorylation. Pyruvate dehydrogenase kinase (PDK) deactivates pyruvate dehydrogenase which changes pyruvate into acetyl-coA before it enters the Krebs cycle. Hypoxia Inducible factor and Myc, Akt oncogenes cause increased glycolysis and up-regulates glycolytic enzymes, increasing activity of signal transduction pathways PI3K, Akt and mTOR, ultimately leading to tumor growth. Glutamine can provide energy in the presence of glucose deprivation entering the Krebs cycle via acetoglutarate.
In pancreatic cancer, hypoxia increases HIF-1 alpha levels thereby causing hedgehog-mediated tumor-stromal interactions, stromal fibroblast activity and fibrous tissue deposition. Tumors become more aggressive and desmoplastic [18].
Acid-mediated tumor invasion hypothesis proposes that during increased glycolysis and increased lactic acid secretion, the concentration of H+ within poorly perfused tumors increases (pH drops to acidic levels) and produces a gradient of H+ ions which then flow from the tumor onto normal adjacent cells. This increased acidic microenvironment decreases extracellular pH and induces death of adjacent normal cells, angiogenesis, extracellular matrix degradation, and tumor invasion [16].
Ketone bodies have been described as being able to reverse gene expression patterns and reactive oxygen species levels, to alter insulin binding and to block glycolysis at the phosphofructokinase level, but few published data exist in humans regarding the use of a dietary approach to glycolytic control in cancer patients [7,8,19]. With this background, glycolytic inhibition by way of pharmacologic agents plus dietary manipulation has promise in the metabolic approach to cancer control.
Human studies so far have proven tolerability of this diet while maintaining tumor stability in cancer patients from 4 weeks till a maximum of 12 weeks. Fine et al., completed his 10 patient study within a single institution whereas the study by Schmidt et al., gathered data from 16 patients distributed over multiple sites. Both documented small heterogeneous populations of cancers (colorectal, pancreatic, thyroid, esophageal, breast and utero-ovarian) tumors [2,7,8]. Rieger et al., studied 19 glioma patients and reported up to 13 weeks with a median progression free survival of 5 weeks [3]. Our trial seeks to test the safety and feasibility of continuing this diet in a broader spectrum of solid FDG-positive malignancies (including prostate, melanoma, sarcoma, hepatobiliary tumors), recruit up to 20 subjects and attempt to extend this study to patients who can tolerate the diet for up to 16 weeks and beyond.