Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Review Article - (2014) Volume 4, Issue 2
According to data of the World Health Organization, cardiovascular diseases belong to the leading causes of death worldwide. In addition, the ischemic heart disease is the number one cause of death. Chronic stable angina pectoris is the most frequent symptom or form of the ischemic heart disease. High heart rate appears to play an important role in its patophysiology, since it takes part in the development of the endothelial dysfunction at the atherosclerosis’ onset. Current pharmacotherapy of the stable angina pectoris is limited. The development of ivabradine, which is a selective and specific inhibitor of the If current in the sinus node, enabled new possibilities in its management. Ivabradine’s antianginal properties were tested in many randomised, placebo controlled clinical studies. Nowadays, it is indicated as a second-line therapy for patients, who cannot be treated with betablockers because it would be unsuitable or insufficient with respect to reaching adequate heart rate. The aim of this review is to provide information about the development and mechanism of action of ivabradine, discuss about its possible pleiotropic effects, provide an information about clinical trials with ivabradine, and describe current status of ivabradine in clinical practice. Supported by grant VEGA number 1/0858/11.
Keywords: Ivabradine; If current; Heart rate; Pleiotropic effects; Clinical trials; Indications
Cardiovascular diseases belong to the leading causes of death worldwide. In addition, the ischemic heart disease is the number one cause of death. Chronic stable angina pectoris is the most frequent symptom or form of the ischemic heart disease. High heart rate appears to play an important role in its patophysiology, since it takes part in the development of the endothelial dysfunction at the atherosclerosis’ onset. Current pharmacotherapy of the stable angina pectoris is limited. The development of ivabradine, which is a selective and specific inhibitor of the If current in the sinus node, enabled new possibilities in its management and also in the management ofpatients with chronic heart failure.
The development and mechanism of action of ivabradine
Ivabradine is the first selective and specific inhibitor of the sinus node If current. If current was firstly described by Brown et al. in 1979, in the isolated sinus node tissue. Due to the particular characteristics of the If current - activation by hyperpolarization of the cell membrane during diastole (depolarization current -50 mV) and nonselective transport of the sodium and potassium cations, it was named funny current. It is activated by sympathicus and blocked by acetylcholine [1]. Its discovery gave to the scientists the opportunity of developing a drug with the pure heart rate reduction. Alinidine, a derivative of clonidine was the first inhibitor of the If current, but it was in appropiate because of its relative inotropic effect [2]. Further experiments also turned out unsuccessfully, as developed molecules were causing potentially fatal prolongation of the QT interval [3]. Next agents, which have been in clinical trials [for example zatebradine] showed no benefit for patients, and they also had unacceptable effect on the QTc interval [4].
Ivabradine as the new drug selectively reducing the heart rate dates back to the first half of the 1990s. It was firstly described by Thollon in 1994; subsequently Bois et al. documented its bradycardic effect on the rabbit´s sinoatrial cells. Initial in vitro studies with ivabradine confirmed its selectivity [5] and animal studies outlined its significant effect on the heart rate reduction without any other effects including influence of the contractility of myocardium of QTc interval [6].
Thus, ivabradine is selective and specific inhibitor of If current. It works through the G-trimer and adenyl cyclase system to form cAMP (Figure 1). Alpha subunit of the G protein in inactive status contains guanosine diphosphate (GDP) and noncovalently bonded heterodimer subunits beta and gamma. Interaction with activated receptor, that binds the corresponding molecule (beta-blocker, ivabradine), catalyzes the exchange of GDP for guanosine triphosphate (GTP). The bond of GTP on G protein leads to the separation of the subunits beta and gamma from the subunit alpha, which binds to the effector, which is activated and starts effector mechanisms. Internal GTPase activity of the subunit alpha leads to the hydrolysis of GTP to GDP, and isolation of alpha subunit from the effector molecule. Inactivated subunit alpha is then connected with the beta and gamma subunits and it is returned into the resting phase. Alpha subunit and cAMP are interfering each other and they block opened If current during the spontaneous diastolic depolarisation by two mechanisms: extension of the duration of diastolic depolarization and increase of the threshold potential [7] (Table 1).
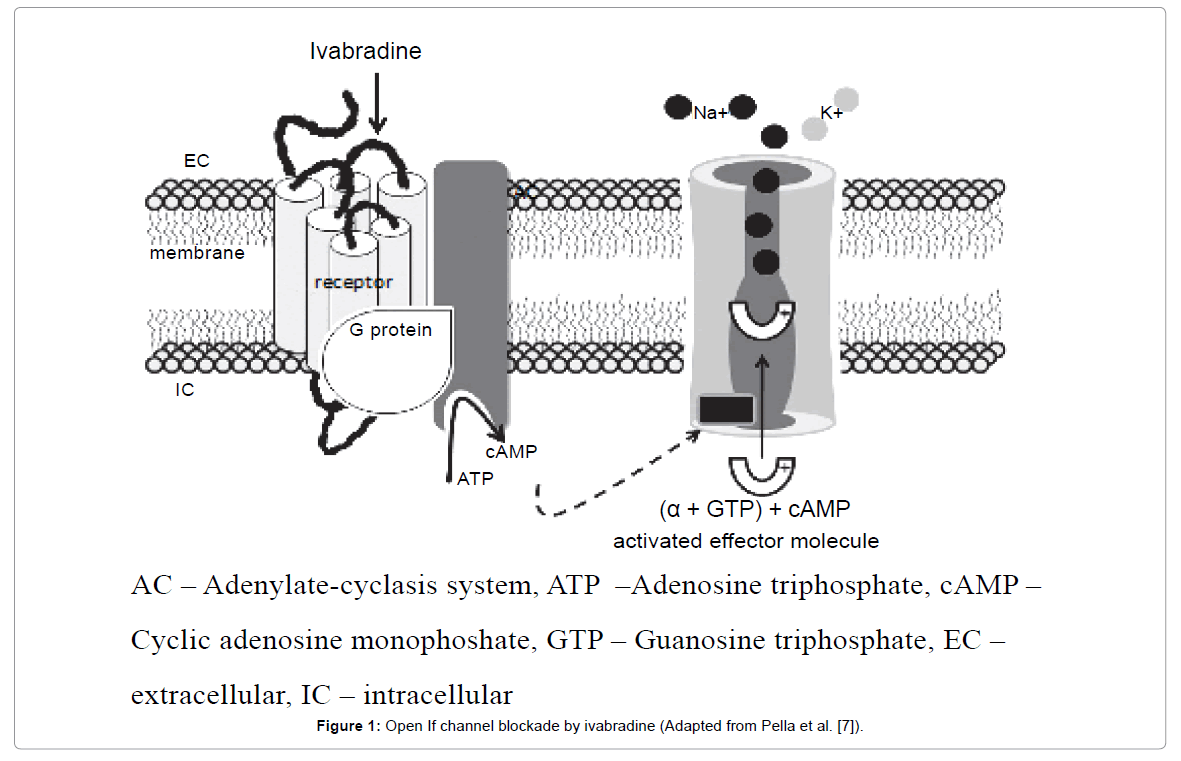
Figure 1: Open If channel blockade by ivabradine (Adapted from Pella et al. [7]).
| Trial | Indication | Design | Objective | Treatments | Conclusions |
|---|---|---|---|---|---|
| INITIATIVE Tardif et al. [15] | Chronic stable angina pectoris, sinus rhythm | Randomized Double blinded Multicentric | To compare the anti-anginal and anti-ischaemic effects of ivabradine and the beta-blocker atenolol. | ivabradine 5 mg b.i.d. for 4 weeks and then either 7.5 or 10 mg b.i.d. for 12 weeks or atenolol 50 mg od for 4 weeks and then 100 mg od for 12 weeks | Ivabradine is as effective as atenolol in patients with stable angina. |
| ASSOCIATE Tardif et al. [16] | Chronic stable angina pectoris, sinus rhythm | Randomized Double blinded Multicentric Placebo-controlled | To evaluate the anti-anginal and anti-ischaemic efficacy of ivabradine in patients with chronic stable angina pectoris receiving beta-blocker therapy. | atenolol 50 mg/day + ivabradine 5 mg b.i.d. for 2 months, increased to 7.5 mg b.i.d. for a further 2 months, or atenolol 50 mg/day +placebo | The combination of ivabradine 7.5 mg b.i.d. and atenolol at the commonly used dosage in clinical practice in patients with chronic stable angina pectoris produced additional efficacy with no untoward effect on safety or tolerability. |
| BEAUTIFUL Fox et al. [17] | Coronary artery disease and a left-ventricular ejection fraction of less than 40%, sinus rhythm | Randomized Double blinded Multicentric Placebo-controlled | To test whether lowering the heart rate with ivabradine reduces cardiovascular death and morbidity. | ivabradine 5 mg b.i.d. ( if resting heart rate of ≥60 b.p.m. 2 weeks after the inclusion visit - 7.5 mg b.i.d.) or matching placebo | Reduction in heart rate with ivabradine does not improve cardiac outcomes in all patients with stable coronary artery disease and left-ventricular systolic dysfunction, but could be used to reduce the incidence of coronary artery disease outcomes in a subgroup of patients who have heart rates of 70b.p.m .or greater. |
| SHIFT Swedberg et al. [20] | Symptomatic heart failure and a left-ventricular ejection fraction of 35% or lower, sinus rhythm with heart rate ≥ 70 b.p.m | Randomized Double blinded Multicentric Placebo- controlled | To assess the effect of heart-rate reduction by the selective sinus-node inhibitor ivabradine on outcomes in heart failure. | ivabradine titrated to a maximum of 7.5 mg b.i.d. or matching placebo | Results support the importance of heart-rate reduction with ivabradine for improvement of clinical outcomes in heart failure and confirm the important role of heart rate in the pathophysiology of this disorder. |
| SIGNIFY Ferrari [21] | Stable coronary artery disease and an LV ejection fraction >40%, in sinus rhythm, with a baseline resting heart rate of ≥70 b.p.m. | Randomized Double blinded Multicentric Placebo- controlled | The primary end point is a composite of cardiovascular death or nonfatal myocardial infarction. | ivabradine 7.5 mg b.i.d. or matching placebo | The study is expected to end in 2014. |
Table 1: Clinical trials with ivabradine.
Decrease of the heart rate by this mechanism is dose _ dependent. Interestingly, effect of ivabradine is more significant in patients with a higher baseline heart rate, because If current can be blocked only when it is opened - and it is opening more frequently when the heart rate is higher. This effect can reduce the risk of severe bradycardia at rest, for example during the night. Ivabradine has minimal or no effect on myocardial contractility, blood pressure, intracardiac conduction and ventricular repolarisation. At the treatment dose, ivabradine has no effect on electrocardiographic PR or QT (QTc) interval. When compared with beta-blocker atenolol, ivabradine depresses myocardial relaxation to a lesser extent both at rest and exercise [8].
Pleiotropic actions of ivabradine
The selectivity of a selective bradycardic agent refers to reducing heart rate and as such to a selective reduction of the If current in the sinus node. However, under certain circumstances, such as ischaemia or heart failure, the normally low expression of hyperpolarizationactivated cyclic nucleotide-gated channels [which carry the If current] outside the sinus node is increased [9]. Such left ventricular If-carrying channels can also contribute to calcium currents and possibly to calcium overload. Potentially, then, part of the observed beneficial effects of ivabradine could be independent of heart rate reduction and be exerted directly on left ventricular myocardium [10].
In an established pig model of regional myocardial ischaemia/ reperfusion, ivabradine improved regional blood flow and contractile function proportionately, and this beneficial effect was entirely reversed by atrial pacing. Also, ivabradine when given either before or after the onset of ischaemia reduced infarct size, but this beneficial effect was only partially reversed by atrial pacing. Ivabradine when given just before reperfusion also reduced infarct size and this beneficial effect persisted and was not reversed by atrial pacing. Apparently, the reduction in infarct size by ivabradine is only partially mediated by heart rate reduction during myocardial ischaemia, but to a significant extent also by an yet undefined beneficial action on reperfusion injury. Unfortunately, no data have been reported so far on the potential persistance of ivabradine´s beneficial effects on post-myocardial infarction remodelling when heart rate is not reduced [11].
In the context of atherosclerosis and vascular disease in more general, the functional role of If-carrying channels and potential targets of ivabradine remain to be elucidated. Particular studies have reported effects of ivabradine on vascular function. In dyslipidaemic mice, the impairment of acetylcholine-induced, endothelium-dependent vasodilatation of cerebral and renal arteries was restored by ivabradine, but not by metoprolol at equal heart rate reduction, suggesting that ivabradine´s action was not related to heart rate reduction [12]. Again in dyslipidaemic mice, cholinergic endothelium-dependent vasodilatation was restored by ivabradine, and vascular NADPH oxidase activity and free radical production as well as atherosclerotic lesion formation were reduced. In this particular study, a direct effect of ivabradine on vascular function and free radical formation was not observed and thus ivabradine´s action was related to attenuation of vascular shear stress along with heart rate reduction [13].
There is evidence for heart rate -independent pleiotropic effects of ivabradine on infarct size, whereas pleiotropic effects on other important end points [remodelling, vascular function] remain to be further analysed [14].
The INITIATIVE study (International Trial of the Antianginal effects if Ivabradine Compared to Atenolol) involved 939 patients with chronic stable angina pectoris randomized into ivabradine 5 mg bid for 4 weeks followed by either 7.5 or 10 mg bid for 12 weeks or atenolol 50 mg od for 4 weeks then 100 mg od for 12 weeks. All patients underwent exercise stress tests at the time of randomization and after 4 and 16 weeks of therapy. Total exercise duration at the end of the 4 weeks did not show significant difference in ivabradine and atenolol groups. The number of angina attacks was decreased by two-thirds with both ivabradine and atenolol. The study concluded that ivabradine is as effective as atenolol in patients with stable angina [15] (Table 1).
The aim of the ASSOCIATE study was to evaluate the anti-anginal ant anti-ischaemic efficacy of the selective If current inhibitor ivabradine in patients with chronic stable angina pectoris receiving beta-blocker therapy. In this double-blinded trial, 889 patients with stable angina receiving atenolol 50 mg/day were randomized to receive ivabradine 5 mg bid for 2 months, increased to 7.5 mg bid for a further 2 months, or placebo. Patients underwent treadmill exercise tests at the trough of drug activity using the standard Bruce protocol for randomisation and at 2 and 4 months. Total treadmill exercise test duration after 4 months increased by 24.3 ± 65.3 s in the ivabradine group, compared with 7.7 ± 63.8 with placebo (P<0.001). Ivabradine was superior to placebo for all exercise test criteria at 4 months (P<0,001 for all) and 2 months (P-values between < 0,001 and 0,018). Ivabradine in combination with atenolol was well tolerated. Only 1.1% patients withdrew owing to sinus bradycardia in the ivabradine group the combination of ivabradine 7.5 mg bid and atenolol at the commonly used dosage in clinical practice in patients with chronic stable angina pectoris produced additional efficacy with no untoward effect on safety or tolerability [16].
BEAUTIFUL (The morbidity-mortality evaluation of the If inhibitor ivabradine in patients with coronary artery disease and leftventricular dysfuction) was an international, multicenter, randomized, double-blind, placebo-controlled 2-arm trial in 781 centers worldwide. The study was designed to demonstrate the superiority of Ivabradine over placebo in the reduction of cardiovascular mortality, hospital admission for acute myocardial infarction, and hospital admission for new-onset or worsening heart failure [primary composite end point]. The study population includes patients who are likely to benefit from the heart rate–lowering effect of Ivabradine (stable coronary artery disease patients with sinus rhythm and left ventricular systolic dysfunction) and who are at high risk of experiencing a cardiovascular event. The background cardiovascular treatment should be considered as an optimal standard of care, and may include a beta-blocker, statin, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker, and antiplatelet drugs. During the inclusion visit, patients had a baseline evaluation. Eligible patients were randomized to 1 of the 2 treatment arms, namely, double-blind Ivabradine, or placebo. The starting dose of Ivabradine was 5 mg (or matching placebo) twice daily in all patients. Patients receiving 5 mg twice daily (or matching placebo) 2 weeks after the inclusion visit with resting heart rate of ≥ 60 bpm will receive the target dose of 7.5 mg twice daily (or matching placebo).
A total of 10 917 coronary patients with left ventricular dysfunction were recruited in 781 centers in 33 countries, and were followed up for a median duration of 19 months and a maximum duration of 35 months. Although the primary composite end point of the study did not reach statistical significance, the results have provided answers to some very important questions in the management of coronary artery disease patients. The BEAUTIFUL study is the first prospective study to demonstrate that coronary patients with a baseline heart rate ≥70 bpm have a significantly higher risk of cardiovascular events, independently of other comorbidities or treatments. BEAUTIFUL has also shown that in these coronary patients with a heart rate more than 70 bpm, ivabradine significantly reduces the risk of coronary events by 22% (P=0.023), fatal and nonfatal myocardial infarction by 36% (P=0.001) and coronary revascularization by 30% (P=0.016) [17].
The subgroup analysis of the effect of ivabradine in BEAUTIFUL trial patients whose limiting symptom at baseline was angina pectoris was also performed. A total of 1507 patients with angina were included in this BEAUTIFUL subgroup analysis. Of these, 734 patients were treated with ivabradine, while 773 received placebo. Nearly all patients were additionally receiving conventional treatment aimed at protecting against cardiovascular events, with approximately nine out of every 10 patients on β-blockers. The benefit of ivabradine was even more striking in angina patients with high resting heart rate (≥70 beats per minute), where ivabradine significantly reduced the primary end point of cardiovascular death, hospitalization for myocardial infarction, and heart failure by 31%, the risk of hospitalization for myocardial infarction by 73% and the need for coronary revascularization by 59%. These findings set ivabradine apart as an antianginal agent that has been documented to be able to increase cardiovascular benefits in patients with angina [18].
The SHIFT study (Systolic Heart failure treatment with If inhibitor ivabradine Trial) was designed to specifically evaluate whether ivabradine improves cardiovascular outcomes, symptoms, and quality of life when added to current guideline-based therapy in patients with heart failure and systolic dysfunction. The study was designed to demonstrate the benefits of ivabradine, on the top of optimal guidelinebased treatment, on cardiovascular events such as cardiovascular death or hospitalization for worsening heart failure. The study population included patients with stable symptomatic chronic heart failure (NYHA class II, III, or IV in stable condition for > 4 weeks) and a prior hospitalization for worsening heart failure within the previous 12 months. Left-ventricular systolic dysfunction defined by an ejection fraction < 35% was required. Ivabradine or placebo was given on the top of background cardiovascular therapy optimised in accordance with current guidelines. It could include an angiotensin-converting enzyme inhibitor and/or angiotensin II receptor blocker, a β-blocker, a diuretic, and an aldosterone antagonist. During the inclusion visit, patients had a baseline evaluation. Eligible patients were randomized to either ivabradine or placebo treatment. The primary endpoint was the composite of cardiovascular death or hospital admission for worsening chronic heart failure. The starting dose of ivabradine was 5 mg (or matching placebo) twice daily in all patients. 14 days after the inclusion visit, patients with resting rate of ≥ 60 bpm received the target dose of 7.5 mg twice daily or matching placebo. If the resting heart rate was < 50 bpm or patient was experiencing signs or symptoms of bradycardia, the dose was reduced to 2.5 mg twice daily. If resting heart rate was between 50 and 60 bpm, the dose was maintained at 5 mg twice daily. The dose could be adjusted at each follow-up visit according to similar criteria. Changes in functional capacity were assessed by NYHA classification, and changes in symptoms of heart failure were assessed by global assessment questionnaires [19].
In the SHIFT study, ivabradine significantly reduced the risk of the primary composite endpoint of hospitalization for worsening heart failure or cardiovascular death by 18% (P<0.0001) compared with placebo. These benefits were observed after 3 months of treatment. SHIFT also showed that administration of ivabradine to heart failure patients significantly reduced the risk of death from heart failure by 26% (P=0.014) and hospitalization for heart failure by 26% (P<0.0001). The improvements in outcomes were observed throughout all prespecified subgroups: female and male, with or without beta-blockers at randomization, patients below and over 65 years of age, with heart failure of ischemic or non-ischemic etiology, NYHA class II or class III, IV, with or without diabetes, and with or without hypertension. SHIFT was conducted in 677 centers in 37 countries and included 6505 heart failure patients for a median duration of 22.9 months and up to 41.7 months. SHIFT is the largest morbidity-mortality study of treatment of heart failure. Adding ivabradine, the specific heart rate-lowering agent, to standard therapies significantly improved morbidity and mortality in heart failure patients with a low ejection fraction and heart rate ≥70 bpm, and in sinus rhythm. The benefit of ivabradine in these patients is such that only 26 patients need to be treated for 1 year in order to avoid one primary event (cardiovascular death or hospitalization for worsening heart failure). Ivabradine was safe and well tolerated with serious adverse events occurring more frequently in the placebo group than in the ivabradine group. Over 75% of patients achieved the target dose of 7.5 mg twice daily. This analysis raised the possibility that ivabradine may be helpful to reduce major cardiovascular events in patients with stable coronary artery disease and left ventricular systolic dysfunction who present with limiting angina [20].
Ivabradine has been proven to effectively prevent myocardial ischaemia and treat symptoms in patients with chronic stable angina pectoris. The BEAUTIFUL trial sheds new light on the role of heart rate control in cardiovascular disease and shows that ivabradine in patients with heart rate above 70 bpm prevents coronary outcomes. These are particularly important data because they have been obtained on top of the best possible preventive therapy, including β-blockers. BEAUTIFUL has also led to a series of stimulating hypotheses that constitute the rationale for another trial called SIGNIFY, which enrolled patients with coronary artery disease and normal left ventricular function with a resting HR of ≥70 b.p.m. The primary endpoint will take into consideration only coronary artery disease outcomes, i.e. cardiovascular mortality and hospitalization for myocardial infarction. So SIGNIFY will be a logical extension of BEAUTIFUL. The results of this trial will really be important not only clinically, but also for understanding the role of heart rate in the pathophysiology of ischaemic heart disease. It is in fact possible that heart rate reduction may carry a different meaning according to the underlying pathophysiology. The study is expected to end in 2014 [21].
Clarify registry
The CLARIFY registry (Prospective observational longitudinal registry of patients with stable coronary artery disease) is the first international and the largest registry, designed to increase knowledge and understanding of stable coronary artery disease (CAD). CLARIFY involves a minimum of 30,000 outpatients with stable coronary artery disease from around 40 countries worldwide, who are followed for 5 years and data are collected prospectively at annual visits at 12, 24, 36, 48 and 60 months. The database includes outpatients with CAD proven by a history of at least one of the following criteria: a documented myocardial infarction which occurred more than 3 months ago, a coronary stenosis blocking more than 50% of the artery, as proven by angiography, chest pain with evidence of heart muscle oxygen deprivation (myocardial ischemia) as proven by one of the following diagnostic tests – stress ECG, stress echocardiography, or myocardial imaging, a Coronary Artery Bypass Graft (CABG) or Percutaneous Coronary Intervention (PCI) procedure which was carried out more than 3 months ago. The main objectives of this registry in stable coronary artery disease outpatients are:
1. To characterize contemporary stable coronary artery disease outpatients and provide important data on: the demographic and clinical profile of the stable CAD outpatient population, current treatment in daily practice, adherence to guidelines and evidence-based practice, the changing patterns of stable CAD management during the registry follow-up, variations in management of CAD patients according to geography, type of physician, patient characteristics and to identify gaps between actual practice and evidence.
2. To determine long-term prognostic factors in this group of patients including the role of resting heart rate, with a view to developing risk prediction model. This information will help to improve the management of patients with CAD and the role of ivabradine in the treatment of these patients can be strengthened. First results of this registry were presented at the congress of the European Society of Cardiology in 2011. These results showed that despite a high rate of use of beta-blockers has one third of patients with coronary artery disease resting heart rate above 70/min. Higher heart rate is associated with higher prevalence and severity of angina pectoris. These findings suggest that there is the need for better control of angina pectoris symptoms by reducing the heart rate [22].
Although the beneficial effect of beta-blockers to reduce morbidity and mortality in patients after myocardial infarction and congestive heart failure was clearly proved, beta-blockers are not administered to all patients who would benefit from the treatment. According to the international surveys, only 50-60% of those for whom they are indicated are using them. There are several reasons. Beta-blockers are contraindicated for some of the patients (approximately 10%), for example, patients with bronchial asthma, hypotension, bradycardia, conduction disturbances or acute decompensation of chronic heart failure. In some patients with chronic heart failure, even with careful titration of the dose of beta-blocker, it can lead to a deterioration of hemodynamic status. Finally, doctors do not often administer betablockers to patients because they are afraid of the side effects, plus a substantial proportion of patients who receive a beta-blocker use it in insufficient doses [23]. In the study, which analyzed the tolerability of beta-blockers in patients with chronic heart failure in clinical practice, 14% of patients discontinued therapy because of their poor tolerance. The most common reasons for discontinuation were fatigue, hypotension, dizziness and shortness of breath. There was a trend toward higher mortality and a greater number of hospitalizations among patients who discontinued the treatment [24]. For abovementioned patients, ivabradine is a second-line therapy.
Ivabradine in patients with angina pectoris
Ivabradine is currently recommended as second-line treatment for patients with stable angina who are either intolerant of beta-blockade or in whom a rate-limiting calcium channel blockers fails to achieve adequate heart rate control, and in combination with a beta-blocker in patients inadequatly controlled with an optimal beta-blocker dose and whose heart rate is over 60 beats per minute [25]. In the guidelines of the European Society of Cardiology for the management of stable angina pectoris, ivabradine is recommended for second-line treatment in patients with the sinus rhythm, who are intolerant of beta-blockers (class of recommendation IIa, level of evidence B) [26]. Heart rate reduction with ivabradine is as effective as with beta-blockers. Ivabradine can also be safely combined with other anti-anginal agents, and addition of ivabradine to beta-blocker therapy further improves anti-ischemic efficacy and exercise capacity of patients with stable angina. Ivabradine is thus an effective anti-anginal agent, alone or in combination with beta-blockers [27].
Ivabradine in patients with heart failure
Ivabradine in patients with symptomatic (NYHA class II-IV) systolic heart failure should be considered to reduce the risk of heart failure hospitalization in patients in sinus rhythm with an EF ≤ 35%, a heart rate remaining ≥ 70 b.p.m., and persisting symptoms (NYHA class II–IV) despite treatment with an evidence-based dose of betablocker [or maximum tolerated dose below that], ACE inhibitor or ARB (angiotensin receptor blocker), and an MRA [mineralocorticoid receptor antagonist] or ARB (class of recommendation IIa, level of evidence B). It may be considered to reduce the risk of heart failure hospitalization in patients in sinus rhythm with an EF≤ 35% and a heartrate ≥ 70 bpm. who are unable to tolerate a beta-blocker. Patients should also receive an ACE inhibitor (or ARB) and an MRA (or ARB) (class of recommendation IIb, level of evidence C) [28]. The results of the SHIFT study showed that in patients with a heart rate ≥70 b.p.m. already receiving guidelines-recommended therapy, use of ivabradine significantly reduced the risk of cardiovascular death and hospitalization for heart failure [primary endpoint]. Ivabradine also improves quality of life and reverses left ventricular remodeling. The prognostic benefits of ivabradine are particularly pronounced in highrisk patients [baseline HR ≥75 bpm], with a significant reduction in both cardiovascular death and all-cause mortality [20].
Limitations of treatment with ivabradine
Ivabradine is contraindicated in patients with a heart rate below 60 beats per minute or where there is evidence of significant conducting system disease (sinus node disease or complete heart block), severe hepatic insufficiency or acute myocardial infarction. The major side effects include transient headache, dizziness and luminous phemomena- a visual disturbance reported in 15 percent of patients due to cross-reactivity with Ih channels in the retina. Patients with luminous phenomena typically describe a transient enhanced brightness in a limited area of the visual field. However, less than 1 percent of patients discontinue therapy as a result [25] (Table 2).
| Mechanism of action Heart rate reduction by selective and specific inhibition of the sinus node If current. |
| Current indications Stable angina pectoris – second- line treatment in patients with the sinus rhythm, who are intolerant of beta-blockers, or with a contraindication to the use of beta-blockers, or in combination in patients inadequatly controlled with an optimal beta-blocker dose Chronic heart failure NYHA II-IV class in patients with systolic dysfunction in sinus rhythm and heart rate ≥ 70 b.p.m., in combination with standard therapy including beta-blocker or when beta-blocker therapy is not tolerated or contraindicated |
| Most common adverse effects luminous phenomena [phosphenes], transient headache, dizziness, bradycardia, AV 1st degree block , ventricular extrasystoles |
| Major contraindications hypersensitivity, resting heart rate below 60 b.p.m. prior to treatment, cardiogenic shock, acute myocardial infarction, severe hypotension [< 90/50 mmHg], severe hepatic insufficiency, sick sinus syndrome, sinoatrial block, unstable or acute heart failure, pacemakerdependent, unstable angina, AV block of 3rd degree |
Table 2: Ivabradine – basic data.
Ivabradine is the first selective and specific inhibitor of the sinus node If current. Ivabradine’s antianginal properties were tested in many randomised, placebo controlled clinical studies. Nowadays, it is indicated as a second-line therapy for patients, who cannot be treated with beta-blockers because it would be unsuitable or insufficient with respect to reaching adequate heart rate [26]. In May 2012 the new ESC guidelines for the diagnosis and management of heart failure included ivabradine by name in the main algorithm for the treatment of patients with chronic symptomatic systolic heart failure (NYHA functional class II–IV) and a heart rate ≥70 bpm [28]. Ivabradine is the first innovative drug after more than a decade to improve the prognosis, reduce hospitalizations, and to improve quality of life in heart failure patients [20]. There is evidence for heart rate - independent pleiotropic effects of ivabradine on infarct size, whereas pleiotropic effects on other important end points (remodelling, vascular function) remain to be further analysed [14].
Supported bygrant VEGA number 1/0858/11.