Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2015) Volume 5, Issue 2
Intraductal Papillary Mucinous Neoplasms (IPMNs) are intraductal mucin-producing cystic neoplasms of the pancreas. Most of these neoplasms are benign but chances of malignant transformation need to be ruled out. These neoplasms have usually been reported from the Wirsung’s duct or its branches. IPMN arising from the the Santorini’s duct is a rare condition. Such tumors originating from the Santorini’s duct are usually associated with incomplete type of pancreatic divisum. IPMNs associated with complete pancreatic divisum have rarely been reported. Imaging techniques including CT scan and MRCP and fluid analysis enabled by SpyGlass pancreatoscopy are the key to diagnosis of IPMN. Treatment usually comprises surgical resection and prognosis depends on malignant changes and lymph node status.
<Keywords: Intraductal papillary mucinous Neoplasia, Santorini's duct, Pancreatic divisum, Pancreatoscopy, Pancreaticoduodenectomy
Intraductal Papillary Mucinous Neoplasms (IPMNs) are intraductal mucin-producing cystic neoplasms of the pancreas. While most IPMNs arise from Wirsung’s duct or its branches, those originating from the minor papillary duct or Santorini’s duct are rare and are usually associated with an incomplete type of pancreatic divisum. Most of these neoplasms are benign or of low-grade malignancy. IPMNs arising from the Santorini’s duct have a higher malignant potential.
A 65 years old non diabetic, normotensive woman presented with upper abdominal pain radiating to the back and a few episodes of non-bilious vomiting. On physical examination, there was tenderness in the epigastrium and left hypochondrium. Blood investigations showed elevated serum lipase (5 × ULN), while amylase level was normal. Other blood investigations including the blood count, liver function tests, blood sugar and renal function test were normal. Abdominal CT scan revealed a bulky head and uncinate process of pancreas, dilated and tortuous pancreatic duct (PD) and cystic lesions in the pancreatic head, the largest one measuring 20.1 × 20.0 mm2 that appeared to communicate with the PD. The rest of the pancreas was atrophic, with minimal peripancreatic fat stranding (Figure 1).
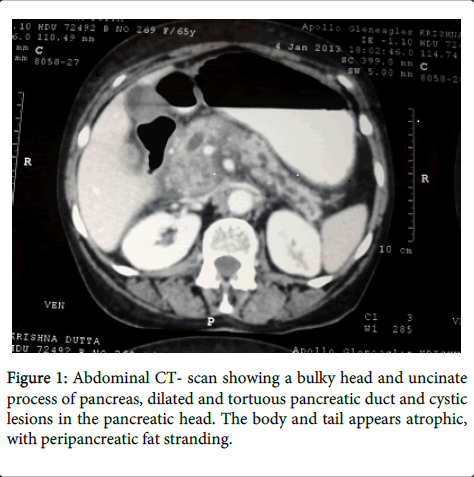
Figure 1: Abdominal CT- scan showing a bulky head and uncinate process of pancreas, dilated and tortuous pancreatic duct and cystic lesions in the pancreatic head. The body and tail appears atrophic, with peripancreatic fat stranding.
Magnetic Resonance Cholangiopancreatography (MRCP) showed an irregularly dilated PD (diameter of 10 mm) and side branches with multiple cystic lesions in pancreatic head, the largest one communicating with the PD with possibility of pancreatic divisum. Treatment for mild acute pancreatitis was started with nothing by mouth, intravenous fluids and analgesics. The patient was pain free and able to tolerate oral diet after five days of treatment. After complete symptomatic improvement, Endoscopic RetrogradeCholangiopancreatography (ERCP) was performed which showed patulous minor papilla covered with mucinous materials, dilated dorsal duct, and complete pancreatic divisum (Figure 2a and 2b).
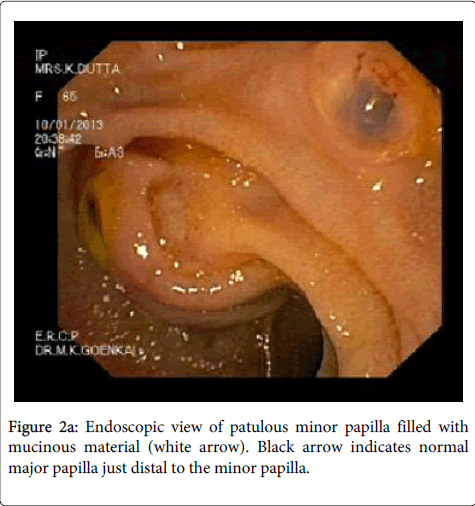
Figure 2a: Endoscopic view of patulous minor papilla filled with mucinous material (white arrow). Black arrow indicates normal major papilla just distal to the minor papilla.
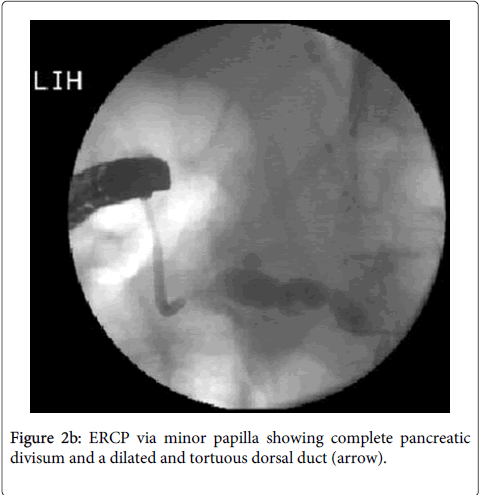
Figure 2b: ERCP via minor papilla showing complete pancreatic divisum and a dilated and tortuous dorsal duct (arrow).
SpyGlass pancreatoscopy showed a dilated and mucin filled dorsal duct. No villous projection was seen (Figure 3).
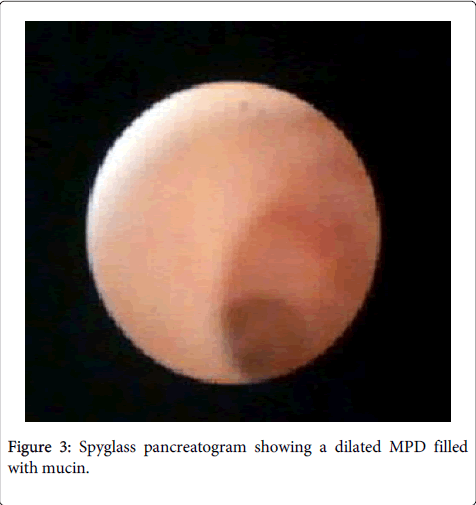
Figure 3: Spyglass pancreatogram showing a dilated MPD filled with mucin.
PD fluid was aspirated for investigations. Fluid analysis revealed a high level of amylase (10171 units per liter) and CEA (1800 micrograms per liter). Nature of the disease, modalities of treatment and prognosis was explained to the patient. The patient was too afraid of surgery and its potential complications, therefore the surgical treatment was denied.
IPMNs were first reported by Ohhasi et al. in 1982. While most IPMNs arise from Wirsung’s duct (major papillary duct) or its branches, those arising from the minor papillary duct or Santorini’s duct are rare [1]. Such tumors originating from the Santorini’s duct are usually associated with an incomplete type of pancreatic divisum [2,3]. Finding a major papilla IPMN is not so uncommon even in our region (Figure 4). However, this report described a rare case of IPMN arising from minor papilla in an unusual background of complete pancreatic divisum.
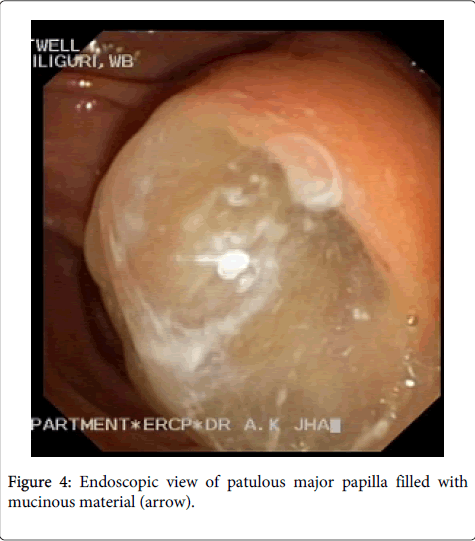
Figure 4: Endoscopic view of patulous major papilla filled with mucinous material (arrow).
Pancreatic divisum is due to failure of ventral and dorsal ducts to fuse, usually around the first 8 weeks of intrauterine life. A common separate pancreatic duct system is called a complete pancreatic divisum while incomplete pancreatic divisum is a small branch between ventral and dorsal pancreatic ducts with incomplete communication. The relationship between pancreas divisum and pancreatic cancers including IPMNs is still not established. Some authors believe that pancreatic duct obstruction caused by a relative stenosis of the minor papilla would leads to stasis and a prolonged exposure to carcinogens [3,4]. As per a study, the prevalence of pancreatic cancer in pancreatic divisum was significantly higher as compared to fused pancreas (P = 0.008; OR, 2.24) [5]. The prevalence of the pancreatic tumors in the pancreatic divisum patients was: 10% for pancreatic cancer, 5.1% for IPMN, and 2.5% for other pancreatic tumors. In contrast, the prevalence of pancreatic tumors in the patients without pancreas divisum was: 4.8% for pancreatic cancer, 2.6% for IPMN, and 1.1% for other pancreatic tumors [5].
IPMN can be invasive or non-invasive in nature and most commonly manifested by abdominal pain, nausea or vomiting. Sometimes the presenting features might include jaundice, weight loss and/or acute pancreatitis. Diagnosis is usually made by CT scan, MRCP and endoscopic ultrasound (EUS). These investigations usually reveal dilatation of Main Pancreatic Duct (MPD) or one of the branches. Fine needle aspiration cytology can be used to confirm the diagnosis. Recently, pancreatoscopy has been shown as a promising technique in the evaluation of IPMN. The characteristic panceatoscopic findings include a papillary tumor with ‘fish-egg’ like appearance, granular mucosa, or mucin [6]. Pancreatoscopy is also useful in differentiating filling defects seen on ERCP and taking biopsy for histopathology. In a study by Nagayoshi et al., biopsies with SpyGlass pancreatoscopy have showed 25% sensitivity and 100% specificity for detecting malignancy. However, SpyGlass pancreatoscopy with irrigation cytology had 100% sensitivity and 100% specificity for detecting malignancy [7].
Most of these neoplasms are benign or of low-grade malignancy. IPMN carries a significant risk of malignant transformation. IPMNs arising from the Santorini’s duct have a higher malignant potential. Since IPMN carries a higher rate of malignant transformation, surgical resection is usually the treatment of choice. Surgical options may include a pancreaticoduodenectomy, total pancreatectomy, distal pancreatectomy, and central pancreatic resection. It is usually preferable to resect only the areas of dysplasia since a total pancreatectomy carries a higher rate of morbidity [8]. The prognosis of IPMN depends on malignant changes and lymph node status mainly. In a study by Sohn et al., the 5-year survival after resection for patients having IPMNs without invasive cancer was 77%, compared with 43% in those patients with an invasive component (P < 0.0001). Five year survival after IPMN resection without malignancy is about 85%, while it is 80% in IPMN with malignancy without lymph node spread and 0% with malignancy with lymph node spread [9].