Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2015) Volume 5, Issue 6
Several treatments have been proposed for the management of spasticity. The injection of botulinum toxin type A is considered the gold standard treatment and appears to be safe and effective. The combination between botulinum toxin type A (BTX-A) and physiotherapy (FKT) is thought to be able to enhance the effects. The aim of this study was to assess the effectiveness of the administration of botulinum toxin type A when combined with a specific rehabilitation protocol in subjects with focal spasticity. 44 subjects were randomly divided into two groups (A and B).
All subjects underwent ECO and EMG guided BTX-A injection. After the injection group A underwent a complex rehabilitation protocol with functional electrical stimulation, functional bandaging, manual therapy, cognitive sensory motor training and focal vibration on the treated muscle; group B made functional rehabilitation at home.
Both groups improved spasticity, pain and function in the first month after the inoculation (T1) but only in group A an improvement at the follow up performed in the subsequent 9 months was observed.
According to the results, it may be suggested that the inoculation of Botulinum toxin A should be properly placed within a specific rehabilitation program.
Keywords: Botulinum toxin; Spasticity; Collagen; Muscles; Therapy
In Italy, the number of subjects affected by a stroke who survived, with disabling outcomes, is about 913,000 people. About a third of them, one year after the acute event showed a high degree of disability, making them not independent in the common activities of daily living [1].
The development of focal spasticity is one of the problems that can further limit the functional recovery and may weigh heavily on the disability of the affected patients.
For the first time in 1980, Lance defined spasticity as a complex hyperkinetic syndrome characterized by an increase of the stretch reflex and a loss of motor control, consequence of the neuronal reorganization as a result of the damage or injury. It becomes clinically evident with increasing speed-dependent resistance to passive movement of a joint [2,3].
Recently, the SPASM group [4,5] elaborated a wider definition of spasticity describing it as a motor sensor disorder.
This disorder is determined by the upper motor neuron lesion that is characterized by a neuronal intermittent activation that clinically manifests with the sustained and involuntary muscles contraction.
Spasticity is characterized both by hyper excitability of the stretch reflex, and by the modifications of the passive biomechanical changing properties of muscle.
Recent studies have shown that the abnormal response of the stretch reflex is insufficient to explain the increase of muscle tone; the hypertonia is to be referred also to an alteration of collagen fibers, the loss of sarcomeres and modifications of the tendon tissue [6-8].
Although spasticity is determined by a damage of the central nervous system, the changes that occur in the peripheral nerves and muscles are essential in maintaining or worsening of the spasticity.
The prevalence of spasticity is related to the incidence of various diseases that affect the CNS.
In patients with stroke it is estimated between 17 and 38% [9,10], in patients with spinal cord injury it varies from 12 to 49%, in the traumatic brain injury it is between 25 and 34% [11,12], in multiple sclerosis this value can reach approximately 54% [13] and in infantile cerebral palsy about 50%.
Spasticity is due to reduced autonomy of movement, inability to take care of themselves independently, altered body image, inability to maintain good hygiene. The obvious consequences are pain and pressure ulcers. The management of spasticity and its complications is very expensive and there is an urgent need to identify the best, safe, effective and efficient treatment [14].
In Literature there are several treatments recognized to be appropriate for the control of spasticity, such as stretching exercises, mobilization exercises slowly and progressively involving joints, electrical stimulation and strengthening of the antagonistic muscles, orthoses, splints, antispasmodic drugs orally administered, injections of phenol and botulinum toxin for neuromuscular block, intrathecal baclofen, surgical arthrodesis and lengthening tendon [15].
The injection of botulinum toxin type A in spastic muscles is considered the gold standard for the treatment of focal spasticity as safe and effective.
Before the introduction of botulinum toxin in the 90s, the drug treatments were limited to the use of spasmolytic drugs and blocks nerve injection with phenol or alcohol.
These interventions, although effective in the control of spasticity, were associated with numerous side effects [16,17]. The clinical effects of Botulinum toxin inoculation become evident after 4-7 days and last for 3-4 months.
Myopathies, Myastenia gravis, neuropathies, late trauma represent a relative contraindication.
The adverse events most frequently reported are: local skin reaction and fatigue, dysphagia, respiratory distress, autonomic dysfunction, skin rash and brachial neuritis. The peak of the adverse effect becomes evident after 2-4 weeks.
In the last decade a series of randomized controlled clinical trials have supported the superiority in terms of efficacy and safety, of botulinum toxin compared to traditional spasmolytic drugs in the treatment of focal spasticity.
Several authors have shown that botulinum toxin is able to reduce muscle tone and increase the ROM of joints by changes in the rheological properties of the muscle.
The need for further studies comes by the high economic impact and the transient effects of botulinum toxin.
Many authors [18] emphasize the combination of treatment with botulinum toxin type A (BTX-A) and physiotherapy treatments (FKT) to implement the algorithm of treating spastic hypertonia and increase the effectiveness of the toxin.
Therefore, the primary aim of this pilot study was to compare the effectiveness of the administration of botulinum toxin type A with the administration of botulinum toxin type A combined with a specific rehabilitation protocol post inoculation in patients with focal spasticity of the upper limb in stroke outcomes.
Confrontation was conducted in terms of
• reduction of focal spasticity of the upper limbs
• increase in ROM of the affected joints
• increase of muscle function
• increase of activity dayling living (ADL)
A secondary aim of this study was to evaluate whether the association of a specific rehabilitation protocol associated with administration of botulinum toxin could increase the time between two successive administrations of botulinum toxin resulting thus in savings on annual expenses for the drug and reduction of the risk of an antibody reaction.
The randomized pilot study was approved by the local ethics committee in accordance with the Helsinki Declaration of 1964. All subjects involved in the study have been informed about the procedure and the aim of the research and signed the informed consent.
The study was conducted by the Department of Physical Medicine and Rehabilitation of the '"G. D'Annunzio" University of Chieti and the Department of Neurophysiology of the "S.Spirito" Hospital of Pescara.
The inclusion criteria were
• patients with focal spasticity of the upper limb in outcomes of ischemic stroke >6months
• patients aged between 18 and 75 years
• Modified Ashworth Scale ≥ 1+
• Score ≥ 2 Scale Tardieu
• Last botulinum toxin treatment and specific rehabilitation>3 months
The exclusion criteria were
• fixed contractures and/or bone deformities of the affected joints
• cognitive disorders which limited the ability to understand and respond to questions and specific tasks
• Comorbidity with degenerative diseases of the central nervous system
• Diseases of the peripheral nervous system
• myopathies
• Comorbidity with an unfavorable prognosis disease within 6 months
We enrolled 61 patients with focal spasticity of the upper limbs in ischemic stroke outcomes in the Department of Neurophysiology of the "S. Spirit "Hospital of Pescara, between the months of November 2012 and the month of March 2013.
Among the patients enrolled in the study, 17 patients were excluded.
The 44 patients, finally included, were randomly divided into two groups (Group A and Group B) (Figure 1).
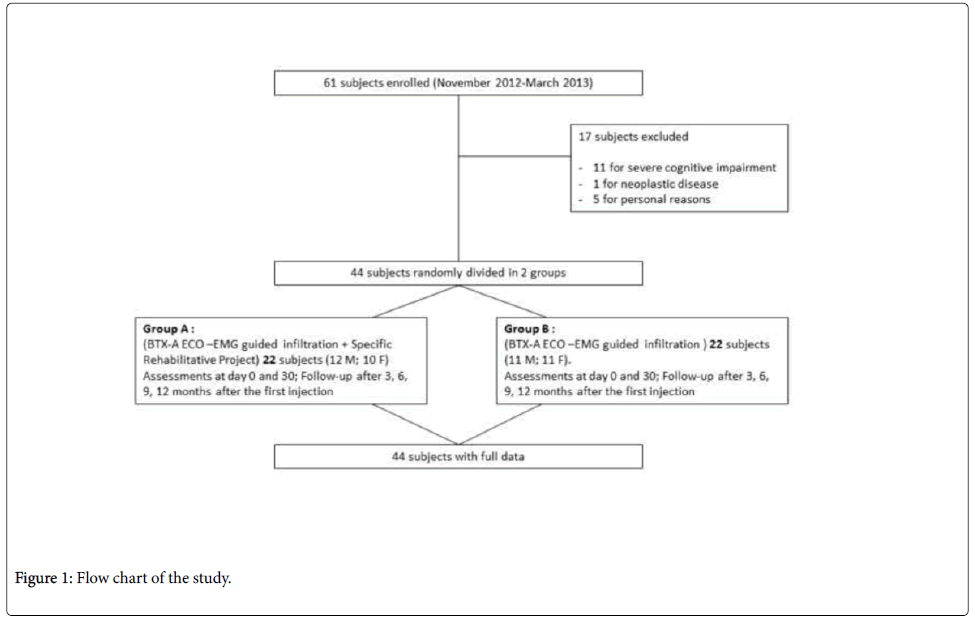
Figure 1: Flow chart of the study.
All the patients enrolled in the study had been admitted in day-hospital in the Department of Neurophysiology of the Hospital "S. Spirito" of Pescara.
For each patient the medical records containing the personal information, family history, and comprehensive anamnesis and specific functional evaluation board for spasticity was compiled.
The passive ROM of the joints of the upper limbs were measured with a goniometer and muscle strength of the muscles treated with botulinum toxin were measured with the MRC (Medical Research Council) scale.
Each subject was evaluated by: rating scales specific for spasticity (Modified Ashworth Scale, Scale Tardieu to V3, test Bahkta), measurement of ROM joints involved, Visual Analog Scale for Pain (VAS) of the muscles involved, Functional Independence Measure (FIM®).
All patients underwent venous blood sampling for the study of basic blood chemistry profile and they underwent ECO and EMG guided BTX-A (BOTOX®-Allergan) injection in spastic muscles of the upper limbs. The total dose average of 400-600 U was divided between the affected muscles related to the muscle mass.
Each vial of 100 IU of BTX-A was diluted in 2 ml sterile saline solution to 9%. The dose of drug to be administered was prepared in a 1 cm, 3 sterile plastic syringe with needle from 24th-27th G and 25-40 mm in length.
The subjects enrolled in the study were randomly divided into two groups (Group A and Group B) and reassessed to 30 (T1), 90 (T2), 180 (T3), 270 (T4) days and 360 days (T5) after the first injection.
Group A consisted of 22 patients (12 M and 10 F, mean age 48aa) who performed
• ECO and EMG guided BTX-A (BOTOX® -Allergan) injection in spastic muscles according to the International Guidelines ("Spasticity in adults: managment using botulinum toxin" -January 2009);
• on the second and third day post injection, patients underwent functional electrical stimulation at a frequency of 5 Hz for 30 minutes per session;
• functional bandaging from the 7th until the 14th day after injection;
• from the 14th day after injection manual therapy, cognitive therapy, sensory motor training (Perfetti's technique) and mechano-focused sound vibration at a frequency of 120 Hz applied to the spastic muscle (2 sessions per week for 3 months in total) have been performed.
The group B (control) consisted of 22 patients (11M 11F, mean age 53aa) who had ECO and EMG guided BTX-A (BOTOX® -Allergan) injection in spastic muscles according to the International Guidelines ("Spasticity in adults: managment using botulinum toxin" -January 2009), and functional rehabilitation at home in a number of 40 sessions distributed over a year time.
Data analysis
Statistical analysis was carried out with System One-way ANOVA; the minimum level of significance was set to p<0.05.
In group A
At T0, the hemiplegic shoulder joint ROM average was equal to 86° in flexion, 82° in abduction, 20° in external rotation, 18.1° in internal rotation . The average of the hemiplegic elbow joint ROM was equal to 24.5° in extension, 72° in flexion. The average of the hemiplegic wrist joint ROM was 35°in pronation, 37° in supination, 29° in extension, 42° in flexion.
Average value of spasticity measured by the Ashworth scale amounted to 2.2 for the shoulder, to 2.6 for the elbow, to 2.4 for the wrist.
Average score of Tardieu scale was equal to 2 for the shoulder (85°), the elbow (90°) and to the wrist (42.5°).
Average score of Bahkta test in hemiplegic hand was equal to 2.75. Average score MRC was equal to 1.6 on the muscles treated; the average value of subjective pain was equal to 3.6 VAS.
The average score on the FIM scale was equal to 86; subjective pain level average was to 3.6 on the VAS scale; average score of FIM Scale was 86.
In group B
At T0 the hemiplegic shoulder joint ROM average was equal to 84.7° in flexion, 80.9° in abduction, 20° in external rotation , 17.7°in internal rotation, elbow joint ROM average was equal to 24.1° in extension, 71.5° in flexion, wrist joint ROM average was 34° in pronation, 36.6° supination, 28.8° in extension, 41.4° in flexion.
Average value of spasticity measured by the Ashworth scale amounted to 2.5 for shoulder, 2.5 for elbow, 2.7 for wrist.
Average score of Tardieu scale was 2 for shoulder (82°), elbow (84°) and wrist (38.7°).
Average score of Bahkta test in hemiplegic hand was equal to 2.56. Average score MRC was 1.6; subjective pain level average was 3.7 on the VAS scale; average score of FIM Scale was 85.6.
After 30 days from injection of botulinum toxin (T1)
In group A: Hemiplegic shoulder joint ROM average was 102.4° in flexion, 114° abduction, 33° in external rotation, 18° in internal rotation, elbow joint ROM average was 33° in extension, 114° in flexion, wrist joint ROM average was 55° in pronation, 56° in supination, 43° in extension, 58° in flexion.
Average value of spasticity measured by the Ashworth scale was 1.5 for the shoulder, elbow and wrist.
Average score for the Tardieu scale was 1 of the shoulder (92°), elbow (115°) and wrist (58°). Average score of the Bahkta test for hemiplegic hand was 3. The average score in the test of strength MRC was 2.8 on the muscles treated; subjective pain level average was 1.4 on the VAS scale; the average score of the FIM scale was 100.4.
In group B: Hemiplegic shoulder joint ROM average was 101.8° in flexion, 95.9° in abduction, external rotation in 23°, 18° internal rotation, elbow joint ROM was 44.9° in extension, 97.7° in flexion, ROM of the wrist joint average of 35° pronation, supination 34.5°, 34° in extension, 67.2° in flexion.
Average value of spasticity measured by the Ashworth scale was 2 for the shoulder, 1.5 for the elbow, 2 for the wrist.
Average score of Tardieu scale was 2 for shoulder (108.3°), elbow (95.5°) and wrist (57.4°).
Average score of the test Bahkta for the hemiplegic hand was 2.68. Average score in the test of strength MRC was 1.8 on the treated muscle; subjective pain level average of 1.4 on the VAS scale; the average score of the FIM scale was 93.2.
90 days after the first inoculation (T2), the date of the second inoculation
In group A: hemiplegic shoulder joint ROM average was 122° in flexion, 126° abduction, 38° in external rotation, 34° in internal rotation, elbow joint ROM average was of 37° in extension, 127° in flexion, wrist joint average ROM was 58° in pronation, 59° in supination, 58° in extension, 61.2° in flexion.
Average value of spasticity measured by the Ashworth scale was 1 to for the shoulder, elbow and wrist. Average score of Tardieu scale was 1 for the shoulder (120°), elbow (120°) and wrist (58°).
Average score of the test Bahkta for the hemiplegic hand was 3.5 Average score in the test of strength MRC was 2.8 on the treated muscle; subjective pain level average was 1.2 on the VAS scale; average score of the FIM scale was 105.5.
In group B: hemiplegic shoulder joint ROM average was 93.6° in flexion, 92.7° in abduction, 22° in external rotation, 18° in internal rotation, in elbow joint ROM average was 38.9° in extension, 86.1° in flexion, wrist joint ROM average was 35° in pronation, 33.5° in supination, 34° in extension, 52.9° in flexion.
Average value of spasticity measured by the Ashworth scale was 2.3 for the shoulder, 1.9 for the elbow, 2.2 for the wrist.
Average score of Tardieu scale was 1.9 for shoulder (91.8°), elbow (90°) and wrist (49.5°).
Average score of the test Bahkta for the hemiplegic hand was 2.73 . Average score in the test of strength MRC was 1.7 on the treated muscle; subjective pain level average was 1.8 on the VAS scale; average score of the FIM scale was 94.2.
At follow up, 6 months after the first injection (T3)
In group A: hemiplegic shoulder joint ROM average was 128.3° in flexion, 127.5°in abduction, 38.7° in external rotation, 34.4° in internal rotation, elbow joint ROM average was 38.2° in extension, 131.3° in flexion, wrist joint ROM average was 58.5° in pronation, 59.3° in supination, 58.2° in extension, 62.7° in flexion.
Average value of spasticity measured by the Ashworth scale was 1 for shoulder and wrist, 0.7 for the elbow.
Average score of Tardieu scale was 1 for the shoulder (127.5°), elbow (123°) and wrist (58.4°).
Average score of the test Bahkta for the hemiplegic hand was 3.6.
Average score in the test of strength MRC was 2.8 on the treated muscle; subjective pain level average of 1.1 on the VAS scale; average score of the FIM scale was 106.3.
At follow up, 9 months after the first inoculation (T4)
In group A: hemiplegic shoulder joint ROM average was 133.2° in flexion, 129.1° in abduction, 39.7° in external rotation, 35.1° in internal rotation, elbow joint ROM average was 39.4° in extension, 133.8° in flexion; wrist joint ROM average was 59.5° in pronation, supination 59.4°, 59° in extension, 64.9° in flexion.
Average value of spasticity measured by the Ashworth scale was 1 for shoulder and wrist and it was 0.2 at the elbow.
Average score of Tardieu scale was 1 for shoulder (135°), elbow (130°) and wrist (60°).
Average score of the test Bahkta for the hemiplegic hand was 3.7.
Average score in the test of strength MRC was 3 on the treated muscle; subjective pain level average of 0.7 on the VAS scale; average score of the FIM scale was 108.4.
In group B: hemiplegic shoulder joint ROM average was 95.2° in flexion, 93.6° in abduction, 22.8° in external rotation, 18.9° in internal rotation, the elbow joint ROM average was 39.3° in extension, 86.5° in flexion, wrist joint ROM average was 35.4° in pronation, 34° in supination, 34.7° in extension, 53.4° in flexion.
Average value of spasticity measured by the Ashworth scale was 2 to the shoulder, 1.6 to the elbow, 1.9 to the wrist.
Average score of Tardieu scale was 1.8 on the shoulder (92°), elbow (90°) and wrist (49.5°).
Average score of the test Bahkta for the hemiplegic hand was 2.82.
Average score in the test of strength MRC was 1.8 on the treated muscle; subjective pain level average of 1.4 on the VAS scale; average score of the FIM scale was 95.8.
At follow-up, 12 months after the first inoculation (T5)
In group A: hemiplegic shoulder joint ROM average was 134.1° in flexion, 129.6° abduction, 40.3° in external rotation, 35.5° in internal rotation; elbow joint ROM average was 43° in extension, 135° in flexion; wrist joint ROM average was 60.1° in pronation, 60.2° in supination, 60° in extension, 65.4° in flexion. Average value of spasticity measured by the Ashworth scale was 1 to the shoulder, 0.5 to the wrist and 0.2 to elbow. Average score of Tardieu scale was 0.8 on the shoulder (135°), elbow (130°) and wrist (60°).
Average score of the test Bahkta for the hemiplegic hand was 3.9. Average score in the test of strength MRC was 3.2 on the treated muscle; subjective pain level average was 0.4 on the VAS scale; average score of the FIM scale was 109.5.
In group B: hemiplegic shoulder joint ROM average was 97.2° in flexion, 94.1° in abduction, 25° in external rotation , 19° in internal rotation; elbow joint ROM average was 39° in extension, 88° in flexion; wrist joint ROM average was 35° in pronation, 34° in supination, 37° in extension, 53.5° in flexion.
Average value of spasticity measured by the Ashworth scale was 1.8 for shoulder, 1 for elbow, 2 the wrist. Average score of Tardieu scale was 1.8 on the shoulder (92°), elbow (90°) and wrist (49.5°).
Average score of the test Bahkta for the hemiplegic hand was 2.8. Average score in the test of strength MRC was 1.9 on the treated muscle; subjective pain level average was 1.4 on the VAS scale; average score of the FIM scale 96 (Figures 2-20).
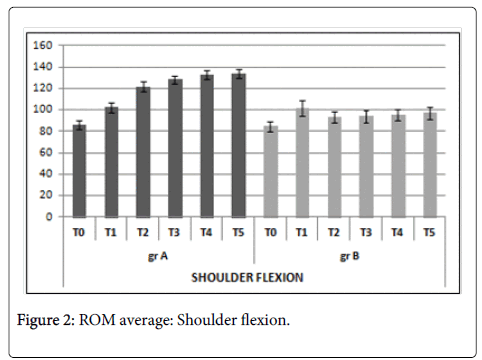
Figure 2: ROM average: Shoulder flexion.
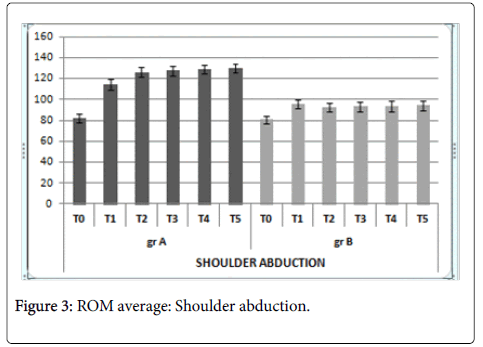
Figure 3: ROM average: Shoulder abduction.
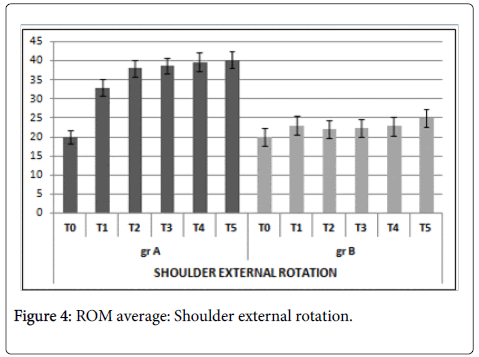
Figure 4: ROM average: Shoulder external rotation.
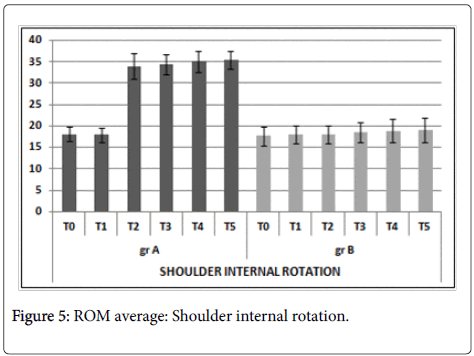
Figure 5: ROM average: Shoulder internal rotation.
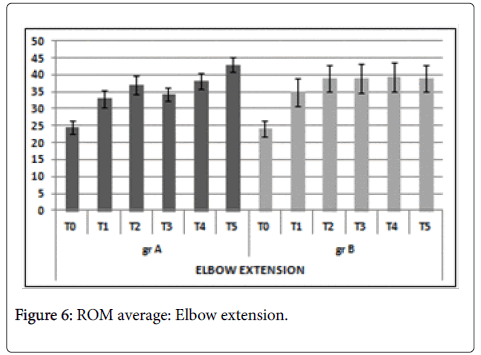
Figure 6: ROM average: Elbow extension.
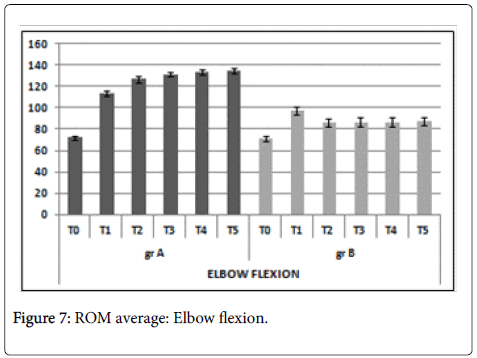
Figure 7: ROM average: Elbow flexion.
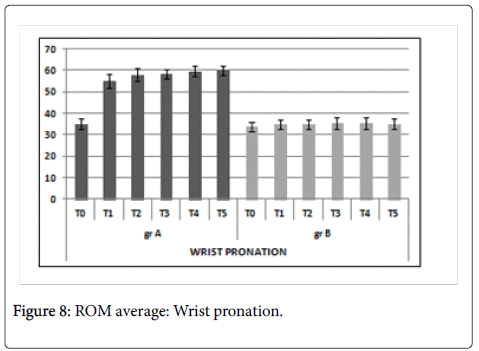
Figure 8: ROM average: Wrist pronation.
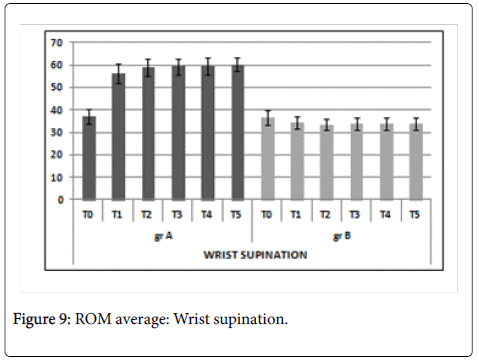
Figure 9: ROM average: Wrist supination.
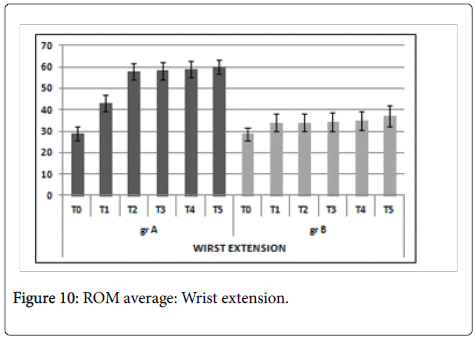
Figure 10: ROM average: Wrist extension.
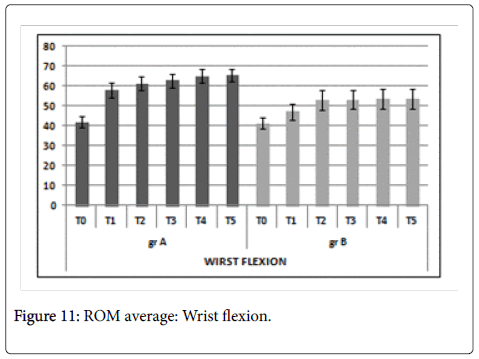
Figure 11: ROM average: Wrist flexion.
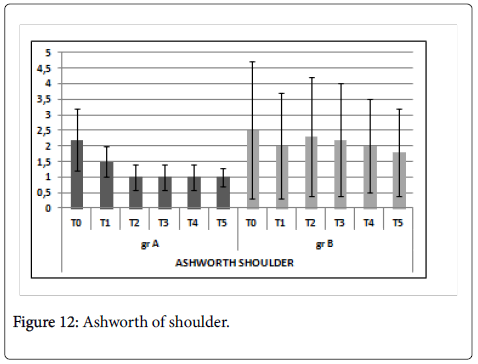
Figure 12: Ashworth of shoulder.
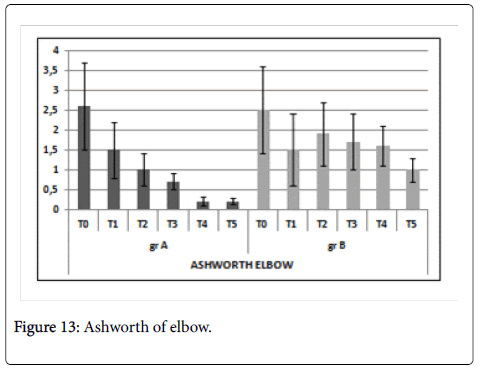
Figure 13: Ashworth of elbow.
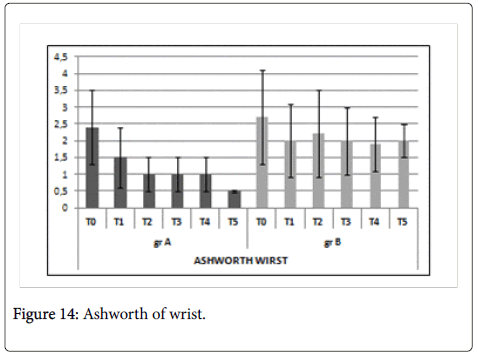
Figure 14: Ashworth of wrist.
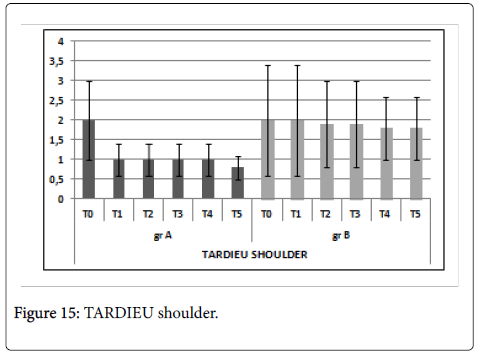
Figure 15: TARDIEU shoulder.
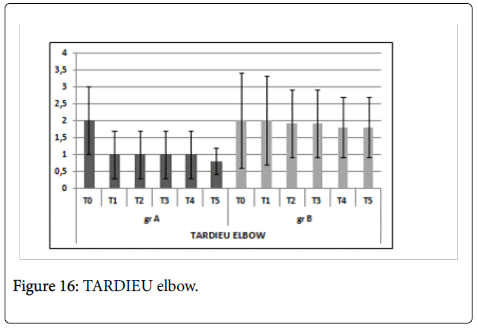
Figure 16: TARDIEU elbow.
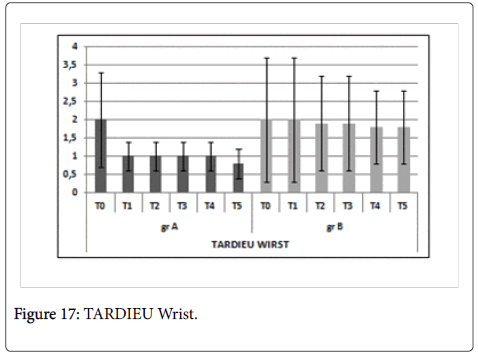
Figure 17: TARDIEU Wrist.
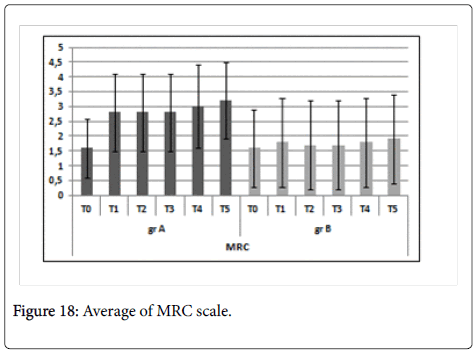
Figure 18: Average of MRC scale.
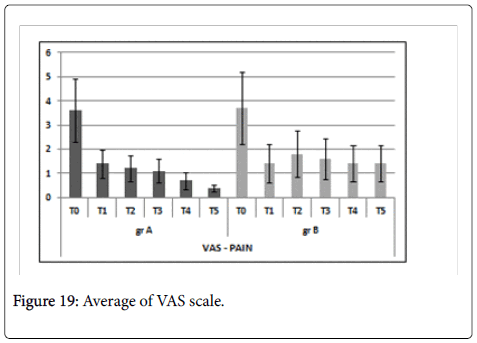
Figure 19: Average of VAS scale.
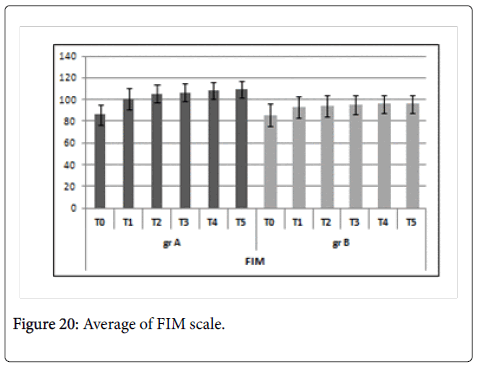
Figure 20: Average of FIM scale.
The analysis of the results of the present study demonstrated the effectiveness of the administration of BTX-A in controlling focal spasticity. In line with the literature, we highlight the need to place such treatment in a wider rehabilitation process, in such a way to optimize the results in terms of action and duration.
In fact, between T0 (first dose) and T1 (30 days after the first administration that corresponds to the peak of the pharmacological action of the toxin), in both groups a statistically significant reduction of spasticity (assessed by MAS and Tardieu scale) was observed, together with an increase in passive ROM of the joints of the upper limbs, of muscle function (measured by MRC scale), an improved quality of life (increased FIM scale values) and a greater ability to opening the hand (Bakhta test).
In the subsequent follow-up, performed after 3 months, i.e., just before repeating the successive inoculation of BTX-A (and, therefore, when the pharmacological action of the toxin was decreased due to the onset of neuronal sprouting phenomena), it was shown:
In group A (who performed BTX-A inoculation and specific and complex rehabilitation project post inoculation), a progressive reduction of focal spasticity and a progressive increase in passive ROM of the upper limbs joints, improvement of muscle function with greater ability to open the hand and an improvement in quality of life between T1 and T2 and then in all the follow-up performed at T3-T4 and T5.
In group B (who performed BTX-A inoculation and home therapy) a slight increase of focal spasticity and reduced passive ROM of the joints of the upper limbs, muscle function and the ability to perform common AVQ between T1 and T2, i.e., between the first and the third month; in the subsequent follow-up at T3, T4 and T5 was detected a maintenance of the values found in all parameters considered at T2.
These results have demonstrated the importance of structuring a rehabilitative intervention which should be technically and temporally appropriate, after the administration of botulinum toxin for focal spasticity.
The data show that the rehabilitation project carried out in group A has allowed to modulate the complex phenomenon of focal spasticity irrespectively of the pharmacological action of botulinum toxin. These results enable us to state that the use of BTX-A determines a significant reduction in spastic hyper-tonicity but to the extent that the rehabilitator, exploiting the duration of its pharmacological effect, is able to have effect on the components of the peripheral afferent of spasticity which causes its persistence.
The importance of an adequate rehabilitation project is confirmed also by the recent definition and placement of spasticity disorders within the sensory-motor disorders field, which allows to put the damage of CNS in close relationship with the peripheral damage, in a system with positive feedback that tends to support itself [19].
Deformities that develop in spastic hypertonia, initially dynamic, tend to stabilize over time and it is just within the modifiability, extent and persistence of these disorders that based on recent evidences, new elements are introduced. These are defined "maladaptive plasticity", in relation to the plasticity of cortical networks and, therefore, the physiatrist is called to oppose.
So, on this basis and by the theoretical analysis of the most recent data of literature, the implementation of a complex rehabilitation project acting on the multiple components that can influence spasticity seems to be recommended, thus optimizing the response produced by the infiltration of BTX-A. As regards the use of the functional electrical stimulation, in association with BTX-A, this is extremely discussed particularly with regard to start time, duration of application and frequency [20].
Animal model studies showed an increase in internalization of botulinum toxin on the nerve endings of the trigeminal nerve when stimulated with repetitive electrical stimulation, leading to the hypothesis that the state of muscle activity may play an important role on the effects of treatment with BTX-A [21].
In 2008 Baricich, in a randomized pilot study [22] compared the different effectiveness of administration of 150 IU-250 IU of botulinum toxin (Dysport type) in the gastrocnemius muscle (medial head and lateral) in association with the taping (in Group I), to the functional electrical stimulation (in Group II) and the stretching (Group III) obtaining statistically significant results of Ashworth, ROM, motor potentials and gait functionality evaluated with Gait Analysis, which were higher in groups I and II. In a study of 8 healthy subjects it was shown that 20 minutes of stimulation NMES, applied at 5 Hz, after infiltration of 40 IU BTX-A, significantly reduced the amplitude of the motor maximum potential action. A recent study confirmed that functional electrical stimulation applied to 4 Hz on the muscles infiltrated, immediately after injection of BTX-A, significantly reduces the value of the MAS and the amplitude of the C-MAP with respect to the application of the same kind of treatment at a more delayed time [23].
Based on these data, we included functional electrical stimulation at 5 Hz in our rehabilitative project, on the second and third day after inoculation of BTX- A for a time of 30 minutes per session.
As regards muscular stretching, maintained by using specific functional bandaging, this method has proven extremely useful, according to several studies, and also recently approved by the Consensus of Post Injection Management in Post Stroke Spasticity [20].
Stretching promotes normalization of tone, maintains and/or increases the extensibility of the elastic tissue, reduces pain, maintains muscle function and may modify the viscoelastic and structural properties of muscle [24-26].
The maintenance of muscular stretching can be favored by the use of splints and/or functional bandaging. These, as performed in our study, and in accordance with what positively approved in COSMO project, should be applied between the seventh and the fourteenth day from infiltration, when the muscle relaxation induced by the administration of BTX-A has begun and, thus, the muscle can be maintained in the desired position [20].
In line with other studies we also used the manual therapy. It is known that manual therapy leads to a reduction of the release of inflammatory cytokines such as Tumor Necrosis Factor-α (TNF-α), interleukin-6 (IL-6) and reduces the phosphorylation of heat shock protein 27 (HSP27), relieving thereby the stress caused by cell injury of myofibrils and promoting muscle mitochondrial biogenesis [27].
In order to obtain an adjustment of tone and trophism that was more stable in time, we included in the rehabilitative project the focal vibration, directly applied on the spastic muscle at a frequency of 120 Hz with VISS system. (Vissman, Italy)
It has been hypothesized that the vibratory stimulation acts on a monosynaptic reflex circuit engaging the LA fibers and spinal motor neurons: this afferent pattern produces an involuntary contraction in the vibrated muscle (responsible for tonic vibratory reflex or TVR). This contraction is associated with a simultaneous relaxation of its antagonist. The stimulus exerted on the afferent LA fibers of the neuromuscular spindles leads to the activation of large amounts of α-motor neurons with a consequent recruitment of muscle fibers that were not previously active [28].
Furthermore, the vibratory stimulus, with specific frequencies, seems to affect the rheological properties of muscle with reduction of spastic hypertonia [29].
It is extremely debated in literature about the ideal frequency of vibration that could be useful to inhibit the spastic hypertonia and it is even discussed whether to use it directly on the spastic muscle or rather on his antagonist. In a recent study on the focal spasticity post stroke it has been observed that the application of a vibratory stimulus directly on the spastic muscle, at a frequency of 91 Hz, induced, initially, an intense contraction which was followed by a subsequent suppression of spasticity after applying continuous stimuli lasting several minutes. Vibratory stimulation initially produced an intense contraction of the spastic muscle, but after constant stimuli the contraction was suppressed. The exact mechanism by which this occurs is unknown. In a previous study, it was hypothesized that the T- and H-reflexes could be inhibited by a mechanism of presynaptic inhibition, induced by vibration in healthy subjects.
Another theory on the anti-spastic action of focal vibration is related to the induction of an alteration of motor cortex excitability [30].
Among the various sensorial stimuli, muscle vibration, applied at low intensity and high frequency, has proved to be suitable for selectively activating primary fusal afferents; several authors have shown that this type of stimulus is able to modify the excitability of M1 for a certain period of time.
Physiological studies demonstrated that exposure to sensory stimulation is able to "drive" the plasticity within the nervous networks that provide the motor control, thanks to the anatomical connections between homologous regions of S1 (primary somatosensory cortex) and M1 (primary motor cortex). The effectiveness of the focused vibration would then be put in relation to the tight interaction existing between the central and peripheral nervous system, and the phenomena of "cortical neuronal plasticity".
The vibratory stimulus, which appears to be useful to determine a reduction in spasticity, according to the literature, should be included in a range between 70 Hz and 120 Hz, and applied for at least 10 min5. Lastly, some studies reported the effectiveness of vibration on pain control, probably for the action it apparently carries on high caliber myelinated fibers, with neural marrow analgesic action.
The analgesic effect of vibration is based on the "gate control" theory, according to which the mechanical stimuli modulate pain transmission from the periphery to the central nervous system.
Lundeberg, in three studies on the effects of vibration in patients with chronic musculoskeletal pain, showed a significant reduction in pain, resulting in higher social activity [31].
It is known that the upper motor neuronal lesion, due to the loss of projections coming from the upper centers, determines qualitative and quantitative alterations of recruitment within the single muscle; these alterations result in inability to build complex motor tasks in terms of fragmentability, adaptability and variability. These motor patterns are aimless for the performance of AVQ and it is for this reason that through the ETC, in agreement with several studies, it was proposed to develop exercises specifically designed to the recovery of more complex and functional motor patterns.
In the light of what stated above, in order to optimize the health costs and ensure a better therapeutic efficacy and efficiency in subjects with focal spasticity, and in line with what has already been described in the literature, it is indicated that the inoculation of Botulinum toxin A may be properly placed within a specific rehabilitation program. The latter should be realized through a lengthening of the administration time of the BTX- A and the administration of specific rehabilitative procedures such as those described.
Clinical messages (max 50 parole)
The implementation of the proposed operational model has lengthened the interval of time between two subsequent administrations of BTX-A. This has allowed to reduce the number of injections per year from 4 to 3 by 25%, thereby reducing the costs for the NHS and the risk of side effects.
Author has no conflict of interest.
R Saggini: guarantor and designing study, writing the paper. L Scarcello: initiating the study, monitoring progress, writing a part of the paper. A Di Stefano: monitoring progress and writing a part of the paper. SM Carmignano: monitoring progress and writing a part of the paper. G Barassi: monitoring progress in rehabilitation. C Visciano: monitoring progress in rehabilitation, R Antonacci: monitoring progress in neurological examination. V Scorrano: monitoring progress in neurological examination. RG Bellomo: deciding on the analytic strategy, designing study and writing the paper.