Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2016) Volume 6, Issue 5
Background: Contamination of healthcare surfaces contributes to Healthcare-associated infections (HAIs) transmission, representing a global concern. Conventional chemicals-based sanitation shows limitations in controlling surface contamination and related HAIs onset, and can select multi-resistant pathogen species. Recently, a sanitizing procedure involving probiotic-based detergents was shown to decrease surface pathogens up to 90% more than conventional disinfectants, without selecting resistant species. This study aims to analyse the influence of a probiotic-based sanitizing intervention on HAIs incidence and typology. Design: Seven Italian hospitals representative of all Italian geographical areas will be recruited for participation in a multicentre, prospective, randomised, pre-post interventional study, analysing simultaneously for a consecutive 18- months period both microbial surface contamination and HAIs occurrence. The intervention will consist in the substitution of the conventional cleaning procedure (chlorine-based) with a probiotic-based one. In the preintervention phase, hospitals will maintain conventional sanitizing procedures; in the post-intervention phase, the probiotic-based sanitation will be applied, allowing a buffer period for the stabilization of the new method. The participating hospitals will be randomly allocated in the following groups: no-intervention (one hospital), intervention-1st group (three hospitals) and intervention-2nd group (three hospitals), entering the study with a 5- months delay. During the whole study period, all patients admitted to the recruited hospital wards will be continuously surveyed for HAI occurrence. Meanwhile, surface bioburden will be monitored monthly by both biological and molecular assays. Discussion: This study will be the first to provide robust data on the impact of sanitation procedures on healthcare associated infections onset and typology, as no previously reported studies evaluates simultaneously and continuously for a period of 18 months both the environmental surface bioburden, its resistome and the healthcare associated infections onset. Results: The results generated from this study might be important for the development of future guidelines to modulate environmental microbiota and to ameliorate hospital environmental cleaning, implementing prevention strategies to reduce HAIs onset.
Keywords: Hospital surface bioburden; Drug resistances; Probiotic cleaning; Healthcare associated infections
Healthcare-associated infections (HAIs) are a major cause of morbidity and mortality in healthcare settings. In high-income western countries, including Europe, about 5-15% of all hospitalized patients develop at least a HAI during the hospital admission, with high avoidable costs, patient suffering and poor patient outcome [1-4]. In particular, according to the European Centre for Disease Prevention and Control (ECDC), about 3.2 million patients acquire an HAI in European acute hospitals every year, and 37,000 die as a HAI direct consequence [5,6].
In Italy, the HAIs incidence varies from 5 to 10%, and infections caused by antibiotic-resistant microorganisms are becoming more and more common, with a mortality rate of 20-30% [7]. Most frequently, HAIs include urinary tract infections, Surgical Site Infections, pulmonary infections and Blood Stream Infections and Gastrointestinal infections. Italian studies performed in over 50 healthcare structures, confirmed these HAIs as most common and Internal Medicine Wards are among the most involved structures in the phenomenon [7-9].
Based on several evidences, it is accepted that the healthcare environment plays a key role in the transmission of HAIs [4,10-14].
Nevertheless, most reports evaluating the association between environmental cleaning and reduction of infections are based on individual wards or hospital settings [15], and systematic multi-centre studies are lacking.
Also, data on the effectiveness of hospital environmental cleaning are limited, as most studies analyse it as a bundle including multiple components influencing diverse hospital cleaning practices (i.e. training, technique, product, communication) [15,16].
So far, control of surface bioburden has been addressed by conventional chemicals-based cleaning products, which however show limitations, as they do not prevent recontamination phenomena and can furthermore select resistant pathogen species [17-20]. In the search for efficient sanitizing procedures, recently a system based on the use of detergents containing apathogenic probiotic of the sporeforming Bacillus genus (Probiotic Cleaning Hygiene System, PCHS) was shown to reduce pathogen contamination on hospital surfaces up to 90% more than conventional disinfectants [21,22]. Notably, the probiotic-based sanitation also decreased pathogen drug resistance [23]: moreover, safety concerns were addressed in a four-year previous study, showing the genetic stability of PCHS-Bacilli [21,23] and the absence of any infectious risk associated with patient’s exposure to probiotic-treated surfaces [24].
The aim of this study is therefore to assess whether the use of a probiotic cleaning system can directly influence the number and typology of HAIs in acute care hospitals.
Study design
This is a multicentre, prospective, pre-post interventional study analysing simultaneously the level of surface contamination and the incidence of HAIs by number and typology in seven Italian public hospitals over a 15 months period. Trial timing is shown in Figure 1. The following wards will be included in the study: Internal Medicine ward, Geriatric ward, Cardiology ward, Gastroenterology ward,Neurology ward. Each hospital will participate with up to four wards, chosen among those indicated. The typology of the chosen wards should guarantee a wide statistical basis without high variations between the individual wards in terms of HAIs incidence, as these wards have similar HAIs prevalence values (range 4-6%) [7,8]. Six hospitals will receive the intervention, whereas one hospital will serve as an external control for eventual seasonal HAIs fluctuations not related to the intervention. The hospitals will be divided in two groups, which will enter in the study period with a 5-months delay, to minimize seasonal variations. All participating hospitals will be randomly allocated, by a computer-generated choice, in one of the described groups (no intervention; intervention-first group; intervention-second group). The intervention will consist in the introduction of the PCHS sanitizing procedure, which will replace the traditional chemicals-based one. Cleaning staff will be adequately trained for the correct application of the PCHS method in all the hospitals receiving the intervention.
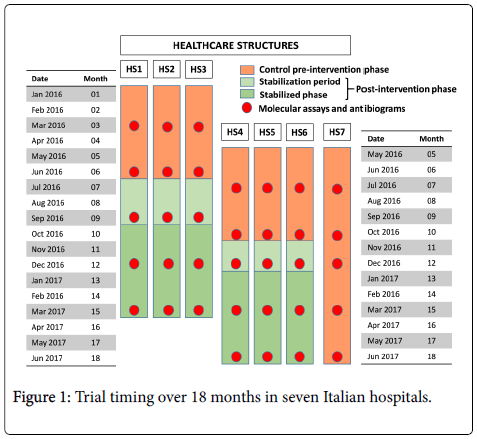
Figure 1: Trial timing over 18 months in seven Italian hospitals.
The study will be divided in two phases (Figure 1): 1) in the control pre-intervention phase the hospitals will maintain the conventional chemicals-based (chlorine products) sanitizing procedures (6 months); 2) in the post-intervention phase the probiotic-based sanitation will be applied, including a first ‘stabilization period’ (2 or 3 months, depending on the hospital group) [21] and a ‘stabilized period’ of continuous intervention application (6 months).
Wards healthcare personnel will be blinded about the change of the cleaning procedures and will keep the existing procedures for prevention and control of HAIs. All participating hospitals agreed to not introduce changes or special programs on HAIs prevention and control during the study period. Hospitals directorates will not be blinded because it is not possible to blind the cleaning staff to the intervention.
During the whole study, specifically trained healthcare personnel will record continuously all HAI events developed in the hospital wards enrolled in the study, using a data base specifically designed and realized for this study. Each HAI will be identified accordingly to the criteria defined by the European Centre for Disease Prevention and Control (ECDC) [25]. A quote corresponding to at least 10 recorded HAIs per hospital setting will be validated by a blinded second expert enrolled in the study, to minimize the risk of infection miscoding.
HAIs recordings will be collected by specifically trained staff (one per hospital), and a central team will be available during the whole study period to standardise data collection. Recording personnel will be provided with a touch screen tablet containing two pre-charged formats, which will be filled-up and uploaded in a password-protected remote database for subsequent analyses.
Bioburden analyses will be performed monthly (Figure 1), by environmental sampling performed in six or three randomized rooms (by a computer-generated random number) for each hospital, respectively for hospitals with more or less than 100 in-patients beds (Table 1). Three different sampling points per room will be sampled (floor, bed footboard and sink), based on previous observations on the representativeness of sampled points [21]. Each point will be analysed with both conventional microbiological and molecular analyses. Microbiological assays will be carried out by use of Rodac contactplates containing selective mediums for quantitation and identification of the following pathogens: total bacteria (TSA medium), Staphylococcal spp. (Baird Parker medium), Enterobacteriaceae spp . (McConkey medium), Acinetobacter spp . (Herella medium), Mycetes (Sabouraud medium), Pseudomonas spp . (Cetrimide medium). Each point will be sampled in duplicate or triplicate (Table 1), resulting in a total number of 42 or 21 plates for each searched pathogen.
| HS1* | ||||||
| HS2* | ||||||
| Sampled points | Room 1 | Room 2 | Room 3 | Room 4 | Room 5 | Room 6 |
| Floor | 3 | 2 | 2 | 3 | 2 | 2 |
| Bed footboard | 3 | 2 | 2 | 3 | 2 | 2 |
| Sink | 3 | 2 | 2 | 3 | 2 | 2 |
| Total plates/room§ | 9 | 6 | 6 | 9 | 6 | 6 |
| *Healthcare structures with enrolled wards including more (HS1) or less (HS2) than 100 in-patients beds; §Corresponding to 42 plates/pathogen (HS1, 6 rooms) or 21 plates/pathogen (HS2, 3 rooms). | ||||||
Table 1: Monthly environmental sampling by Rodac plates in healthcare structures (HS).
Quarterly, the same sampled points will be also collected by sterile swabs and analysed by real time quantitative PCR (qPCR) microarray, to characterize the population resistome (Figure 1). These data, evidencing simultaneously 84 resistant genes, will allow evaluating precisely the trend of drug resistance genes/species in basal conditions and following the intervention. In parallel, all S. aureus isolates, chosen as a drug resistance reference, will be tested by conventional antibiograms for their drug-susceptibility using the following drugs: Penicillin G, Ampicillin, Vancomycin, Oxacillin, Cefotaxime, Imipenem.
In the post-intervention phase, the same molecular assay will be used to analyse two colony isolates of PCHS-Bacillus collected from each sampled point, to monitor the appearance of each eventual new acquired resistance genes, with the aim of confirming the genetic stability already observed in previous studies [21,23]. All microbiological and molecular data will be recorded in a specifically designed common database.
Bioburden data will define the surface microbiota both quantitatively and qualitatively, allowing to compare the preintervention and post-intervention population, and to correlate the level and type of contamination with HAIs data.
All hospitals receiving the intervention will have their own control, represented by the data collected during the control phases. A further external control will be represented by one hospital not receiving the intervention.
Study setting
This study will take place in seven public Italian hospitals representative of Italian large and medium healthcare structures, from different geographical Italian territories (North, Centre and South), and fulfilling the following eligibility criteria:
-each hospital has the indicated wards
-each hospital has over 100 in-patients beds
-each hospital has an established HAIs surveillance program
Recruitment
All patients admitted to the wards of the seven hospitals included in the study will be surveyed in the study, without distinction of age or gender and keeping their identity completely anonymous.
The study will survey a total expected number of 19,000 patients in the entire study period in the six hospitals subjected to the intervention (about 9,500 in the pre-intervention phase and 9,500 in the postintervention phase), and about 2,000 patients in the control hospital.
All patients admitted to the enrolled hospital wards will be monitored daily for the development of HAIs. To this aim, an electronic medical record will be created and uploaded in a specifically designed common database for each observed patient and each arisen HAI. Database analysis will evidence any variation in HAIs number and type between the pre- and post-intervention phases of the study. Overall data regarding the total admitted patients will be useful to conduct comparative analyses on the risk factors of the patients at admission as well as to explore the incidence variation of HAIs.
Intervention
The intervention will be environmental, and it will consist in the introduction of the probiotic-based sanitizing procedure (PCHS), which will replace the conventional chemicals-based one. Cleaning staff will be adequately trained for the correct application of the PCHS method in all the hospitals receiving the intervention. No other new intervention but those still existing potentially affecting HAIs incidence will be implemented in the interested wards during the study.
Outcome measures
The primary outcome measure will be the rate of HAIs (whole infections and typology stratified) in each hospital. Hospitals will collect data in continuum, using a specifically designed electronic medical record, through specifically trained healthcare personnel. Data about all studied patients from the seven hospitals will be kept anonymous and collected in a specifically designed common database. A quote of recorded HAIs (minimum 10 infections) for each hospital will be validated by a second blinded expert, to avoid the risk of infections mis-coding. HAIs will be characterized by typology and route of transmission, and data analysis will be particularly focused on infections transmitted by contact with contaminated surfaces.
Secondary outcome measures will be the qualitative and quantitative evaluation of microbial surface bioburden, which will provide characterization of the surface persisting pathogens, and the analysis of the direct healthcare costs and productivity losses related to the two sanitizing methods. Bioburden will be quantified as number of CFU/m2 of microbial species [21]; resistance/susceptibility of individual isolated bacteria to antibiotics will be evaluated by conventional Kirby-Bauer antibiograms. The presence of drug resistance genes will be evaluated by qPCR microarray and expressed as number of resistance genes per μg of extracted microbial DNA [23].
Data collection and data management
Each participating hospital will be responsible for identifying HAIs events. HAIs recordings will be collected by specifically trained staff (one per hospital). A standardised spread sheet with predefined data fields (Excel 2013; Microsoft) will be specifically designed and used for data collection. A central team will be available during all the study period to discuss any doubt and standardize the data collection. Recording personnel will be provided with a touch screen tablet containing two pre-defined formats, submitted centrally via a secure, password protected website.
The first format (named S1) will be filled out for each patient admitted to the enrolled wards, and will contain anonymised general data of each patient: gender, age, provenience, admission date, admission cause, risk factors at admission time, antibiotics therapy in the two weeks preceding admission, presence of colonization by alert microorganism, eventual presence of HAI and etiological agent.
The second format (named S2) will be filled out in case of HAI onset, and will include information about basal risk at HAI onset, HAI localization, admission phase at HAI onset (initial, intermediate, advanced), HAI etiological agent, drug therapy, infection resolution or outcome.
All anonymised data will be analysed. A data monitoring committee will not be needed, since all data analysers will be blinded to the intervention time and hospital’s group.
In parallel, bioburden data will be collected monthly by the central team, through environmental sampling performed in 3-6 randomized rooms for each hospital. Each sampled point per room (floor, bed footboard and sink, in duplicate or triplicate) will be analysed by Rodac contact-plates, to identify and enumerate total bacteria, Staphylococcal spp ., Enterobacteriaceae spp ., Acinetobacter spp ., Mycetes , Pseudomonas spp . In parallel, all S. aureus isolates will be tested for their drug-susceptibility against Penicillin G, Ampicillin, Vancomycin, Oxacillin, Cefotaxime, Imipenem.
Quarterly, the same sampled points will be also analysed by qPCR microarray, to characterize the population resistome. In the postintervention phase two colony isolates of PCHS-Bacillus collected from each sampled point will be also analysed by qPCR microarray. All microbiological and molecular collected data will be uploaded in the same password-protected website, in pre-defined data fields.
Statistical analysis and power calculation
Variation in infection rates between pre and post intervention phase will be analysed both as incidence rates x 1000 patients days and as number of HAIs x 100 admitted patients. Analyses will be performed on all types of HAIs and etiological agents. Statistical analysis will be performed using χ2 test, Shapiro-Wilk test for evaluating normality, parametric (t test) and non-parametric (Mann-Whithney and Kruskall-Wallis) tests and multivariate analysis (logistic regression), assuming as statistically significant a p value <.05.
For study power calculation, the pre-intervention infection rate was estimated based on admissions and infection data from Italian hospitals [7-9]. The minimum sample size was calculated considering an infection reduction of at least 20% and an 80% power for detecting this difference. Assuming a two-sided test with an alpha level of 0.05 the minimum number of patients with infection should be 175 for the first 6 months (normal sanitization) and 140 for the last 6 months (new sanitization). Considering an infection rate of 5%, to reach at least 175 patients the first 6 months the minimum number of patients to be enrolled should be 6998 in the first 6 months. Taking into account also the three months of stabilization period, a number of around 16000 patients were considered sufficient. Thus, the enrolment of hospitals with a pre-intervention rate of 4-6% in the included wards (as measured in point-prevalence observations), with a total expected number of 19,000 patients in the entire study period, will confer to the study the power to detect a 20% post-intervention reduction of infectious risk.
Collected data will allow for the first time to evidence and measure in a continuous way the influence of sanitizing methods on the level of surface contamination and to correlate it with the onset of specific types of HAIs.
Primary outcomes include the reduction of HAIs number following the introduction of PCHS sanitation, and the identification of a parameter correlating bioburden typology with HAIs onset.
Direct comparison of HAIs rates during pre-intervention and postintervention phases will allow evidencing any quantitative and qualitative variations.
Secondary outcomes include: 1) evaluation of bioburden data, which will provide quantitation and characterization of the pathogens persisting on surfaces, allowing to evidence any variations in HAIs agents prevalence and their antibiotic/drug susceptibility; 2) estimation of the global burden of HAIs management: a cost analysis will be performed from the social perspective, and direct healthcare costs and productivity losses related to the two sanitizing methods will be considered and quantified.
Participating sites agreed not to implement during the study period changes that could impact the trial, e.g. new cleaning policies or other interventions potentially affecting HAIs incidence (standard precautions, hand hygiene practices, etc.). A limitation of this study is that it is not possible to blind hospitals with regard to the change in sanitizing method. However, healthcare personnel recording patients’ data and HAIs will be blinded about the change of the cleaning procedures, and will keep the existing procedures for prevention and control of HAIs. Similarly, the personnel analysing and elaborating collected data will be blinded about the hospitals’ group identity.
Other limitations of the study could include outbreaks of HAIs, seasonal factors, organizational or policy changes. Each site will be constantly monitored, to minimize these factors.
The results generated from this study might be important for the development of future interventional studies aimed to modulate environmental microbiota to ameliorate guidelines about hospital environmental cleaning, for implementation of prevention strategies to reduce HAIs onset.
The results collected in this study will be disseminated through peer-reviewed journal publications, conference presentations and seminars. Moreover, a summary of obtained findings will be provided to all the participating hospitals.
At the time of manuscript submission, the study is ongoing, having started the enrolment of the second group of hospitals, being completed the data collection of the pre-intervention phase in the first group. Trial registration ISRCTN International Clinical Trials Registry, ISRCTN58986947.
Ethics approval and consent to participate
The study has received ethics approval by the Ethical Committees of all the seven healthcare structures participating to the study: Fondazione Policlinico Universitario Agostino Gemelli (Roma), protocol n. 7243/15, October 15th 2015; Ospedale di Santa Maria del Prato (Feltre, Belluno), protocol n. 841, November 5th 2015; Azienda Ospedaliera Universitaria Ospedali Riuniti di Foggia (Foggia), protocol n. 75/2015, July 13th 2015; Istituto Clinico Beato Matteo (Vigevano, Pavia), and Istituto di Cura Città di Pavia (Pavia), protocol n. 20160009859, March 14th 2016; Policlinico Universitario G. Martino (Messina), protocol n. 3/16, March 22th 2016; Ospedale Sant’Antonio Abate, Tolmezzo (Udine), protocol September 2th 2016.
Individual patients’ consent was not necessary, since the intervention is only environmental.
Competing interests and funding
The authors declare that they received unrestricted funding from Copma Scrl (via Veneziani 32, 44124 Ferrara, Italy). However, this does not influence in any way the design and development of the protocol, and the correlated results.
Availability of data and materials
The datasets generated during and/or analysed during the current study available from the corresponding author on reasonable request.
All authors contributed to the development of the study protocol and have been involved in drafting the manuscript or revising it critically for important intellectual content. SM is the overall chief investigator, coordinating central research team. EC contributed to project design, bioburden analyses, and wrote the manuscript. MC contributed to software realization and groups’ coordination. FB, LT, GV, SN, PA, NT, GP, VLF contributed to epidemiologic, and infection control analyses. SB contributed to epidemiologic analyses, health policy and decision making. All authors have read and approved this manuscript.
We thank the staffs of all the enrolled hospitals for their technical assistance. We thank the Study Group SAN-ICA: Luca Lanzoni, Maria D’Accolti, Maria Teresa Camerada, Alessandro Conte, Luca Arnoldo, Carla Rognoni, Antonella Mastretti, Federico Tassinari, Francesca Campanella, Paolo Grotto, Daniela D’Agostini, Eva Vieceli, Francesca Trozzi, Ermelinda Del Buono.