Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2016) Volume 5, Issue 2
Introduction: Muslims practice intermittent Islamic fasting all over the globe each year during Ramadan. This practice induces several changes that may affect work performance. The aim of this study is to evaluate the impact of fast during Ramadan on eating behaviors, sleep habits, daytime sleepiness, and professional life.
Methods: Target population was medical trainees who were working since at least 4 months at the beginning of the study. They were invited to complete an anonymous self-administered questionnaire during and apart from Ramadan.
Results: Two hundred forty-three subjects (243) had correctly completed the questionnaire (mean age = 26.81 ± 2.17 years and sex-ratio = 0.69). During Ramadan, all Alcohol drinkers had stopped drinking (p<0.001), and daily tobacco consumption had significantly dropped from 14.82 ± 8.26 to 11.67 ± 8.64 cigarettes during Ramadan (0.002). Consumption of both coffee and tea was significantly reduced from 2.44 ± 1.3 to 1.03 ± 0.71 and from 1.06 ± 0.59 to 0.77 ± 0.66 cups a day, respectively (p<0.0001). The average number of meals per day dropped from 2.92 ± 0.49 before Ramadan to 1.79 ± 0.58 during Ramadan (p = 0.032). The average bedtime was significantly delayed until to 3.80 ± 5.37 am, while it was at 9.7 ± 10.93 pm during the previous month (p<0.0001). The percentage of subjects who went to bed after midnight also had significantly increased from 57.1% to 93.1% (p<0.001). The degree of dissatisfaction about sleep quality had substantially increased from 18.9% at baseline to 54.7% during Ramadan (p<0.0001). Fasted Trainees found more difficult getting up in the mornings (74.1% versus 79% respectively, p<0.0001). The percentage of trainees who often arrived late for work or missed it increased significantly, from 3.7% at baseline to 11.9% during Ramadan (p<0.0001). The majority (81.1%) reported feeling extra sleepy during the daytime of Ramadan month as compared to 60.1% during the previous month (p<0.0001). It was also noted a higher frequency of digestive disorders (46.9% versus 29.6%, <0.001), morning headaches (15.2% versus 6.6%), excessive nervousness (65% versus 57.6%, p<0.001) and concentration and memory disturbances (88.9% versus 77%, p<0.001). Both daily and weekly working hours had significantly decreased during the month of Ramadan (p<0.001). Trainees started their daily work 15 minutes later and left 20 minutes earlier, which results in 35 less minutes worked per day, and around 3 and half hours less per week. Most of participants (88.1%) thought that Ramadan had a negative effect on their sleeping pattern and affected their daytime functioning. Although, the percentage of those who took sedative-hypnotics for sleep disorders had significantly dropped from 7% at baseline to 3.3% during this month (p = 0.0001).
Conclusion: The present study showed that Ramadan is associated with several changes in eating behaviors and sleep habits. These changes resulted in sleep pattern impairment, increased daytime sleepiness and reduced work performance. Healthy sleep and eating habits with a suitable work rhythm should be recommended to Fasted medical trainees to minimize the impact of Ramadan on their wellbeing and professional life.
Keywords: Sleep; Ramadan; Medical trainee; Wakefulness behavior; Eating
Ramadan is the ninth lunar month of the Islamic calendar. Fasting during this month is obligatory on every adult, sane, and able Muslim and concerns around one and a half billion of people around the world. It involves abstinence from three primal physical needs of human beings- food, drink, and sexual intercourse from dawn to sunset during the entire month of Ramadan (for a period of 29 or 30 days) [1].
Eating is only allowed during the night. The pattern of meals changes as well. Usually two to three main meals are taken: the first called “Iftar”, which means breakfast, is served right after sunset, the second one is served after night prayer, while the third one called “Suhur” is taken right before dawn. Besides, Muslims engage themselves in many religious activities such as offering voluntary prayers, and reciting the Quran particularly in the final third part of the night.
They also have larger and more frequent nocturnal collective gatherings and others ceremonies. As a result, most of people stay awake until the early hours of the morning, which can lead to diurnal sleepiness and affects alertness at work as was suggested by several previous studies [2].
Like in others Muslims countries [1], sleep and eating behavior changes during Ramadan in fasting individuals have been noticed increasingly in Tunisia but have not been well documented.
Medical trainees are particularly concerned by these problems. Actually, they represent the largest and the most active population in Tunisian university hospitals and they have to work nocturnal shifts. They need to maintain optimal alertness and function at peak levels during work to ensure that patients receive safe and effective care.
The present study aimed to investigate the effects of Ramadan fasting on sleep habits, daytime sleepiness and wakefulness among a group of Tunisian medical trainees.
Type of study
This was a prospective monocentric and cross-sectional study performed one week before Ramadan and during the last week of Ramadan, June-July 2014.
During the study period, fasting day was about 15 hours, dawn (beginning of fasting) was between 03:00 and 03:15 am, and sunset (end of fasting) was between 06:30 and 06:45 am. The weather was hot with an average ambient temperature around 38°C and a relative humidity of 70% at the city of Sfax.
The study was approved by the university ethics committee, and informed consent was obtained from each participant.
Participants
The study was carried out in the two University Hospitals of Sfax (Hedi CHAKER and Habib BOURGUIBA university hospitals) and included medical trainees who were working since at least 4 months at the beginning of the study.
Trainees who took leave from work during Ramadan and those who didn’t fast were excluded as well as pregnant or nursing women. The average working hours for Tunisian medical trainees is 6 hours a day, 6 days a week. They also work
They also work night shifts usually more than one time a week. Of 570 subjects approached at the beginning, 60 had immediately refused to participate because of lack of time or lack of interest in the studied subject. As a result, a total of 510 subjects had agreed to participate in this study.
Data collection
The participants were requested to complete an anonymous selfadministered questionnaire with honesty, and were assured of absolute confidentiality of all of their responses. The questionnaire was adapted from a French sleep disorders network “reseau moprhée” and modified according to the specificities of our population.
It contained 51 questions concerning the following aspects: demographic parameters, socio-economic conditions, habits and pathological antecedents, working conditions, eating behaviors, sleepwake schedule, quality of sleep, wakefulness at work and daytime performance.
Statistical analysis
The data were analyzed (SPPS 20.0 for windows, United States) using descriptive statistics and expressed in the text and tables as means ± standard deviation or as percentages, when appropriate. For continuous variables, comparisons were performed using one-way repeated measures ANOVA.
When the difference was significant, post hoc testing was performed using Dunn’s multiple comparison tests. Chi-square test was used for discrete variables. The statistical significant level was set at p<0.05.
Demographic characteristics
Of the 510 trainees who participated in the study, only 243 subjects had correctly completed the questionnaire, for a response rate of 47.64%. The mean age of these participants was 26.81 ± 2.17 years with a slight female predominance (sex-ratio = 0.69).
About two third of them were single (62.6%), and most of them lived in families (85.2%). Among married participants, 14.8% had one or more children. The average body mass index (BMI) was 23.18 ± 3.34 Kg/m2. Nearly the fifth of participants (21.3%) were overweight, while obesity was noted in 4.6% of cases.
A weight gain of 5.68 ± 3.9 kg during the last six months was reported by 71 participants (29.2% of cases). The most common medical conditions reported by participants were, by descending order, psychiatric disorders (n = 19, 7.8%), and cardio-respiratory diseases (n = 8 3.3%).
Table 1 summarizes the principal characteristics of our population.
| Age (years) | Characteristics | 26.81±2.17 |
|---|---|---|
| Sex-ratio (Females/Males) | 0.69 | |
| BMI | Mean (kg/m2) | 23.18±3.34 |
| =18.5 (%) | 3.3 | |
| 18.5-25 (%) | 70.7 | |
| 25-30 (%) | 21.3 | |
| =30 (%) | 4.6 | |
| Martial statue (%) | Single | 62.6 |
| Married | 33.7 | |
| Free Relationship | 3.7 | |
| Number of children (%) | 0 Child | 85.2 |
| 1 Child | 11.5 | |
| 2 children | 2.9 | |
| 3 children | 0.4 | |
| Habitation (%) | Single | 7.4 |
| In family | 85.2 | |
| Ingroup of friends | 7.4 | |
| Medical conditions (%) | Respiratory | 4.1 |
| Arterial hypertension | 2.5 | |
| Cardio-vascular diseases | 3.3 | |
| Thyroid diseases | 2.5 | |
| Neurologic diseases | 0.8 | |
| Psychiatric diseases | 7.8 | |
| Others | 5.8 |
Table 1: Characteristics of the 243 participants.
Habits and eating behaviors
Ten point seven pour cent of participants (n = 26) were drinkers, with an average of 2.23 ± 2.8 drinks per days. During Ramadan, all of them had stopped drinking (p<0.001).
Likewise among the 39 smokers (16%), daily tobacco consumption had significantly dropped from 14.82 ± 8.26 to 11.67 ± 8.64 cigarettes during Ramadan (p = 0.002). However, no one had stopped smoking during this month. Eighty three point one per cent of participants (n = 202) were coffee drinkers consuming an average of 2.44 ± 1.3 per day, while 56% of them were tea drinkers with an average consumption of 1.06 ± 0.59 cups a day.
During Ramadan, consumption of both coffee and tea was significantly reduced at 1.03 ± 0.71 and 0.77 ± 0.66 cups a day, respectively (p<0.0001).
The average number of meals per day dropped from 2.92 ± 0.49 before Ramadan to 1.79 ± 0.58 during Ramadan (p = 0.032).
The time of the first meal changed as well, and it was between 07:00 pm and 08:00 pm in the majority of cases (95%). Nearly two third of participants (61.3%) used to take a second meal during Ramadan, and it was commonly between 12:00 am and 01:00 am.
The Suhur, the third meal, was taken by only one third of the participants (37.4%), and it was between 01:00 am and 03:00 pm (Table 2).
| BeforeRamadan | During Ramadan | p | ||
|---|---|---|---|---|
| Smoking | 16% | 14.82±0.42 (cigarettes/day) | 11.67±8.64 | 0.002 |
| hookah | 7% | 0.94±0.36 hookah /day | 0.94±0.65 hookah /day | 0.705 |
| Coffee | 83.1% | 2.44±1.3 cups/day | 1.03±0.71 cups/day | <0.0001 |
| Tea | 56% | 1.06±0.59 cups/day | 0.77±0.66 cups/day | <0.0001 |
| Alcohol | 10.7% | 2.23±2.8cups/day | 0 cups/day | <0.001 |
| Number of meal per day | 2.92±0.49 | 1.79±0.58 | 0.032 | |
| First meal | From06 am to 07 am:13.2% | From 07 pm to 08 pm:95.5% | ||
| From07 am to 08 am:61.7% | Beyond 08 pm:4.5% | |||
| From08 am to 09 am:21.8% | ||||
| Post prandial:3.3% | ||||
| Second meal | From12 am to 01 pm:11.5% | From 09 pm to 10 pm:3.7% | ||
| From01 pm to 02 pm:45.3% | From 10 pm to 11 pm:7% | |||
| Beyond 02 pm:41.2% | From 11 pm to 12 pm:10.7% | |||
| From 12:00 am to 01:00 am:39.5% | ||||
| No second meal:2.1% | No second meal:38,7% | |||
| Third meal | From 06 pm to 07 pm:1.6% | From 01 am to 02 am:4.1% | ||
| From 07 pm to 08 pm:26.7% | From 02 am to03 am:33.3% | |||
| From 08 pm to 09 pm:39.1% | No third meal:62.6% | |||
| From 09 pm to 10 pm:19.8% | ||||
| Beyond 10 pm:10.7% | ||||
| No third meal:2.1% | ||||
Table 2: Habits and eating behaviours in our population before and during Ramadan.
Sleep pattern
During Ramadan, the average bedtime was significantly delayed until to 3.80 ± 5.37 am, while it was at 9.7 ± 10.93 pm during the previous month (p<0.0001). The percentage of subjects who went to bed after midnight also had significantly increased from 57.1% to 93.1% (p<0.001). On the other hand, the sleep latency had slightly decreased during Ramadan, but this decrease did not reach statistical significance (from 18.98 minutes to 18.29 minutes, p = 0.508).
It had also noted that 48.1% of participants complained of insomnia at baseline versus 57.6% during Ramadan (p<0.0001). In response to the question “do you feel that you don’t sleep enough at night”, the percentage of participants who replied “yes” had significantly increased from 18.9% at baseline to reach 54.7% during Ramadan (p<0.0001). Most of participants (88.1%) thought that Ramadan had a negative effect on their sleeping pattern and affected their daytime functioning.
Although, the percentage of those who took a sedative-hypnotics for sleep disorders had significantly dropped from 7% at baseline to 3.3% during this month (p = 0.0001) (Table 3).
| Before Ramadan | During | P | ||
|---|---|---|---|---|
| Ramadan | ||||
| Bedtime | 9.7±10.93 pm | 3.80±5.37 am | <0.0001 | |
| Bedtime after midnight (%) | 57.1 | 93.1 | 0.001 | |
| Sleep latency (min) | 18.98±14.78 | 18.29±16.61 | 0.508 | |
| Do you think you have insomnia (%)? | No | 51,9 | 42.4 | 0.0001 |
| Small | 33.3 | 28.4 | 0.0001 | |
| Medium | 10.7 | 16 | 0.0001 | |
| Very | 2.9 | 9.9 | 0.003 | |
| Extremely | 1.2 | 3.3 | 0.0001 | |
| Do you feel that you don’t sleep enough at night (%) | Yes | 18.9 | 54.7 | 0.0001 |
| Moderately satisfied | 63.4 | 38.3 | 0.0001 | |
| Highly satisfied | 17.7 | 7 | 0.0001 | |
| Do you take sedative-hypnotics for sleep disorders (%)? | Yes | 7 | 3,3 | 0.0001 |
| No | 93 | 96.7 | ||
| Do you think Ramadan had a negative impact on your sleep pattern and daytime functioning (%)? | Yes | 88.1 | ||
| No | 11.9 |
Table 3: Pattern sleep before and during Ramadan.
Daytime wakefulness
During Ramadan, participants found more difficult getting up in the mornings (74.1% versus 79% respectively, p<0.0001) (Table 4). The percentage of trainees who often arrived late for work or missed it increased significantly, from 3.7% at baseline to 11.9% during Ramadan (p<0.0001).
| Before Ramadan (%) | During Ramadan (%) | p | ||
|---|---|---|---|---|
| Do you find more difficult getting upin the mornings? | Yes | 74.1 | 79 | 0.0001 |
| No | 25.9 | 21 | ||
| Do you arrive late for work or miss it? | Never | 53.9 | 41.2 | |
| Hardly | 42.4 | 46.9 | ||
| Often | 3.7 | 11.9 | ||
| Do you feel extra sleepy during the daytime? | Yes | 60.1 | 81.1 | |
| No | 39.9 | 18.9 | ||
| Do you feel sleepy sleepiness at the wheel? | Yes | 4,5 | 13.6 | |
| No | 95.5 | 86.4 | ||
| Do you have concentration and memory disturbances? | Yes | 77 | 88.9 | |
| No | 23 | 11.1 |
Table 4: Daytime wakefulness before and during Ramadan.
The majority (81.1%) reported feeling extra sleepy during the daytime of Ramadan month as compared to 60.1% during the previous month (p<0.0001). The time period of the day when trainees felt the sleepiest was the same for the two study periods. It was the end of the day, than in the morning (Figure 1).
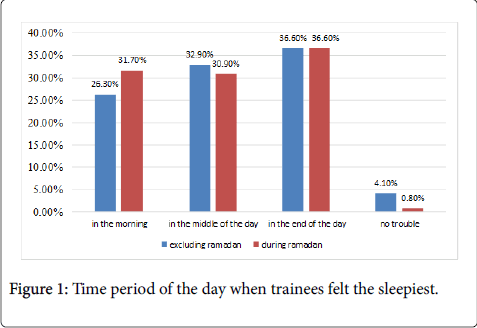
Figure 1: Representative photomicrograph of histopathological features in pulmonary necropsies.
With regard sleepiness at the wheel, the percentage was 4.5% at baseline, and has more than tripled over Ramadan to reach 13.6% (p<0.0001). Similar trends had been observed for concentration and memory disturbances which significantly increased to 88.9% during Ramadan as compared to 77% at baseline (p<0.0001).
Somatic and psychiatric symptoms
Over Ramadan, the percentage of trainees who complained of excessive nervousness significantly increased to 65% as compared to 57.6% at baseline (p<0.001). Similarly, morning headaches were more than tripled during this month, as it were reported by 15.2% of trainees versus 6.6% before Ramadan (p<0.001). It was also noted a higher frequency of digestive disorders which concerned about the half of participants (46.9%) during Ramadan, while in the previous month, it was reported by only one third of them (29.6%) (p<0.009). Epigastralgia was the most common digestive complaint during the two study periods.
Working rhythm
Both daily and weekly working hours had significantly decreased during the month of Ramadan compared to the month prior (p<0.001). The number of night shifts per week had also decreased (p<0.001). Moreover, it was noted that trainees started their daily work 15 minutes later and left 20 minutes earlier, which results in 35 less minutes worked per day, and around 3 and half hours less per week.
The present study explored the perception of young medical trainees in two Tunisian university hospitals regarding the impact of Ramadan fasting in their sleeping patterns, wakefulness and daytime functioning. A better understanding of this specific situation shall be helpful to propose suitable recommendations regarding working conditions, dietary habits and lifestyle behaviors adopted during Ramadan [3].
At baseline, smoking and alcohol consumption were notably less common than what was reported in general Tunisian population. In fact, smoking prevalence among Tunisian adults was estimated at 30.4% in 1996 as compared to 16% in our population [4]. Tunisians are also the heaviest drinkers in the Maghreb region, according to the World Health Organization. In contrast, only Ten point seven pour cent of our participants were drinkers, and most of them had low to moderate level drinking (average of 2.23 ± 2.8 cups per day). Coffee and tea were the preferred average by most of participants (respectively 83.1% and 56%) as they could potentially lead to an energetic impact, and improve wakefulness as well as mental performance.
During Ramadan, all these addictives behaviors were significantly reduced, which can be explained by a long fasting time, about 15 hours a day, while eating and drinking was allowed for only 9 hours a day [3]. Religious prohibition of alcohol was rigorously respected, and all drinkers had stopped drinking during the whole period of Ramadan. Similar result was reported in 2012 by Laraqui [5] in a cross-sectional study that concerned 2171 health care workers in a Moroccan hospital. However, no significant difference was found regarding coffee and tea consumption during Ramadan in comparison with the previous month. Likewise, in a Saudi study published in 2003 and including 56 Muslims healthy medical students, Bahammam [1] noted that there was no significant difference before and during Ramadan in the number of cups of tea, coffee, and chocolate or the number of cans of soda that subjects drank. In contrast with these findings, Laraqui [6], by asking 150 workers in a factory, reported a remarkable increasing consumption of energy drinks (coffee and tea) which was multiplied by four during Ramadan (from 12% to 50%).
Fasting during daytime leads to a sudden change in the circadian pattern of eating which concerns particularly meal schedule and frequency. As has been reported in previous study, the frequency of meals dropped significantly during Ramadan in our study [1,6]. Total food intake generally decreased [7] but a slight increase was reported in Moroccan and Saudi populations [8,9]. Similarly, in a study involving 147 Tunisian students from high health schools, Masmoudi [10] noted that Ramadan was notably associated with over-night eating and increasing consumption of sweet and anarchic food stuff. Eating such particular types of food at inappropriate times may be a factor in gastro-intestinal complaints and predisposes individuals to becoming overweight [11]. A significant correlation between the number of calories ingested during a meal and the duration of subsequent sleep has been reported in rats [12] but the relationship is less clear in humans. Similarly, eating at night after a day-time fast can disrupt sleep due to intestinal discomfort from eating too much or as sequel to hunger from having eaten too little earlier on [11].
Nearly two third of participants (61.3%) in our study used to take a second meal during Ramadan, and it was commonly late at night, before going to bed (commonly between 00:00 and 01:00 am). It has also been suggested that late occurrence of meals may be responsible for circadian rhythm changes in body temperature, and sleep onset latency, as a result. Actually, body temperature falls during sleep and rises at wake time [1]. In general, a falling body temperature induces sleep, whereas a rising temperature provokes wakefulness. During Ramadan, spicy nocturnal meals, the favorite food at Tunisian Ramadan table, can result in an increase in nocturnal body temperature which leads into delay in sleep onset [1,13-15]. Alternatively, the increased sleep latency could be explained by more specifically sleep-related mechanisms. Feedings has shown to induce an increase in the extracellular concentration of histamine in the hypothalamus. In turn, the hypothalamic administration of histamine is able to increase wakefulness [16]. The effect of Ramadan on sleep onset was also examined using the polysomnographic recordings before, at the beginning, at the end and after Ramadan. Sleep latency increased in the 10th and the 24th days of Ramadan. In our study, we didn’t find any significant variation in the sleep latency.
The current study demonstrated a sudden and significant delay in bedtime and wake up during Ramadan, as compared to the month before, in agreement with previous works [1,5,10,14]. This delay occurred despite work commencement time did not change in Tunisian Hospitals during Ramadan, in contrast with others Muslims countries [15]. We hypothesize that, quite apart the changes in the circadian pattern of eating, several others factors may encourage participants to delay bedtimes, such as watching popular programs TV, gathering with families and friends, rising for the predawn meal and prayer, and many social activities that occur until late at night during Ramadan [14]. More than 60% of fasting individuals who stayed awake after 11:00 pm attributed their wakefulness to socializing with families and friends and watching TV [1,12].
As consequence of these nocturnal alterations, most of our study participants (88.1) thought that Ramadan had a negative effect on their sleeping pattern, and the frequency of dissatisfaction with sleep quality increased to 54.7% during Ramadan, as compared to 18.9% at baseline. In a sample of 734 Malaysian junior-level Muslim athletes, there was an equivocal opinion on whether Ramadan fast had any effect on their sleeping pattern. Of those who claimed that their sleep patterns were altered, about 45.9% complained of a reduction in sleeping duration and 45.4% reported that the quality and duration of their sleep were affected [17]. The same finding was reported by Bahammam [1], although, in this study, the total sleep time did not change before and during Ramadan. Rocky et al. [13] have demonstrated that the proportion of non-rapid eye movement sleep increased during Ramadan, particularly stage 2 which represents the light sleep; In contrast, Slow-wave sleep (deep sleep) duration and rapid eye movement sleep duration decreased. These disturbances of sleep structure may explain the subjective feeling of poor sleep quality during Ramadan even when getting the same amount of sleep as the previous month [1].
It appears that Ramadan has detrimental effects on daytime function and sleepiness. In support, it was observed that the majority (81.1%) of our study participants suffered from extra-daytime sleepiness during of Ramadan month as compared to 60.1% during the previous month. Several studies have assessed daytime sleepiness during Ramadan, subjectively, and objectively using the multiple sleep latency test (MSLTS) [15]. Among 734 Malaysian Muslim athletes, Singh et al. [17] noted that the majority of athletes (66.6%) reported feeling extra-sleepy during the daytime of the Ramadan month and 61.2% of these athletes took extra naps between 1-2 hours in the daytime during the fasting month. Likewise, in a sample including 2171 health care workers in Moroccan hospitals [5], sleepiness at work increased to 49.8% as compared to 9.8% at baseline, and the frequency of Epworth greater to 10 increased from 19.4% to 46%. Bahammam noted that the percentage of medical students who reported falling asleep in class increased from 15% at baseline to 36% during the first week of Ramadan [1]. The study of Roky [18] including 8 young Muslims showed an increase in daytime sleepiness, especially at 10:00 and 12:00 am at the end of Ramadan, and a decrease in daytime body temperature during Ramadan. Objective measure of alertness by the MSLT confirmed these results. Sleep latency, which is inversely proportional to sleepiness, increased during the daytime, particularly at 10:00 am, 12:00 am and 04:00 pm [19].
Conflicting results have been reported with regard to the effect of Ramadan fasting on daytime function. Several studies including university students [19-21] reported that fasting may cause mood swings, morning headaches, lethargic feelings, high overall fatiguelevels, decreased memory which in turn can lead to loosing of hours work and decreased work performance as was observed in our study [17]. Similarly, Bahammam noted that the percentage of subjects who exercise regularly dropped from 24% before Ramadan to 5% at the end of Ramadan without any clear reason of this decline [1]. During the first week of Ramadan, psychomotor performance indicators such as critical flicker fusion [21] and choice reaction time [22] have been reported to be impaired. These changes were more important in regular smokers and coffee consumers [7]. In contrast of these findings, Lotfi S reported that physical performance was not dramatically impairment during Ramadan in 9 male resistance athletes. A study in a Jordan population has reported that suicidal behavior decreased during Ramadan [23].
There are different hypothesis to explain sleepiness and daytime dysfunction during Ramadan. Some studies suggested that sleep deprivation or disruption, even modest may be responsible, as was the case in our study [24-28]. Based on this hypothesis, Bahammam demonstrated that if a regimen of a fixed sleep-wake schedule and a fixed caloric intake is followed during intermittent fasting, the effect of fasting on sleep architecture and daytime sleepiness will be minimal. Metabolic changes during the intermittent fasting have been also ruled out as possible factor for increase in subjective and objective sleepiness. Actually Ramadan diurnal fasting lead to decrease in the resting rate and energy expenditure, which in return bring about diurnal rectal temperature decrease as was observed by Roky [18]. It also induces increased cerebral theta activity [22].
Several strategies may be helpful to circumvent or reduce the adverse perturbations of Ramadan fasting. Trainees must realize the importance of sleep as part of their overall rest and recovery strategies, and prioritize sleep time over their evening social activities to increase sleep time. Taking a short afternoon nap is also recommended. Otherwise, fasted trainees can sleep ∼1 hour earlier in the evening instead of taking naps during the day. In addition, taking three main meals especially the meal right before dawn is very important to have sufficient amount of calories over the 24 hours period during Ramadan. However, excessive eating at night, particularly prior to sleep should be ovoid. It also reasonable to improve training conditions as working in a hot and humid environment will result in a greater thermoregulatory challenge to the fasted trainees.
Our study has a few limitations that need to be addressed. First, the sample size of subjects recruited was small. The survey could only determine the subjective perception of participants, as no objective assessment methods was used. It was also difficult to distinguish the specific role of Ramadan in daytime sleepiness and functioning from others possible confounder factors such as sleep deprivation or disruption. Moreover, it must be noted that the findings of this study are specific to Tunisian Muslim medical trainees, and they are not necessarily valid as regards other countries observing Ramadan fasting. Further researches in Tunisia and adjacent Maghreb countries with polysomnographic recording is needed to objectively assess the effects of Islamic intermittent fasting on sleep architecture and daytime sleepiness.
Our study suggests that changes in lifestyle and eating behaviors during Ramadan may impact daytime sleepiness and functioning, which in return impair work performance. In contrast, the specific role of intermittent Islamic fasting is not supported by the available data. An approach to develop a tailored sleep health education and suitable nutritional behavior could be helpful to minimize adverse side effects on daytime function during fasting in medical trainees. Similarly, work rhythm should be adapted to specificities of this month.