Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2014) Volume 4, Issue 6
Question: Repetitive practice facilitates motor learning after stroke but the effect of a rehabilitation program which provides an extra amount of the same, repetitive practice per week remains unknown. This protocol paper describes the methods to address the questions of a planned systematic review:
(1) Does extra practice per week of the same rehabilitation lead to improved activity in stroke survivors? and
(2) What is the amount of extra rehabilitation that needs to be provided to achieve an effect?
Method: A systematic review will be conducted, commencing with a search of Medline, EMBASE, CINAHL, and CENTRAL databases. Randomised and non-randomized controlled trials that compare stroke rehabilitation programs involving similar content but different duration (recorded as therapy time per day or week) will be included. The outcome of interest will be activity, represented by walking ability or upper limb ability. The methodological quality of included studies will be assessed independently by two reviewers using the PEDro scale. Data will be extracted by two reviewers and will be pooled in a meta-analysis where there is sufficient homogeneity. We will calculate mean differences (MD) or standardized mean differences (SMD) and 95% CI for continuous outcomes as appropriate. We will calculate a Pearson correlation coefficient and ROC calculation to define the amount (in hours) of extra rehabilitation that needs to be provided to achieve improved activity in stroke survivors.
Discussion: Findings will explore the relationship between increasing intensity of rehabilitation and improved activity in stroke survivors, and provide guidance to rehabilitation clinicians, inform policy and provide future directions for research.
Systematic review registration: PROSPERO CRD42012003221.
Keywords: Stroke, Rehabilitation, Occupational therapy, Physical therapy, Review systematic, Meta-analysis, Intensity, Dose-response
Stroke is a leading cause of disability among adults worldwide; approximately 80% of stroke survivors are left with impairments affecting activity and participation [1,2]. Repetitive practice promotes motor learning in stroke survivors and prior investigations have shown that an increase in the amount of practice can improve motor outcomes for stroke survivors [3-8]. Despite this overarching finding, confounding factors have been identified when investigating the relationship between increased rehabilitation intensity and patientlevel outcomes [5,6,9]. While more practice is considered best, there is uncertainty regarding the sensitivity of the relationship between rehabilitation intensity and improved activity performance after stroke.
Motor learning occurs through active engagement of the participant in repetitive practice of specific tasks that are challenging, progressive and skill-based [6]. It is generally accepted that therapists should encourage the person with stroke to complete high numbers of repetitions [10-12]. Since 1996 previous systematic reviews have explored the effect of increased amounts of practice in rehabilitation programs; each review has included between 7 and up to 30 randomized and non-randomized controlled trials, and all have consistently generated findings that suggest an overall trend of a positive effect [4- 9], i.e. that providing more therapy leads to better outcomes. Earlier reviews found a small to medium positive effect on walking ability from additional walking practice (summary effect size of 0.32, SD 0.11- 0.52) [8], and significant improvement in ADL from an additional 16 hours of exercise therapy stroke (summary effect size of 0.22, SD 0.07-0.37) [7]. However, more recent investigations exposed conflicting factors that were overlooked during investigations into the complex relationship between a rehabilitation program providing intensive practice and improved outcome [6,9].
More recent systematic reviews modified their inclusion criteria in an attempt to address the criticism made of earlier reviews; that studies provided different therapy interventions across trial arms which would understandably result in different outcomes [5]. An intensive program would provide extra practice of the same task per day or per week, yet some previously included trials were not designed to measure the effect of different doses of the same therapy, rather they studied different types of therapy delivered in different doses, or they studied therapy compared to no therapy [9]. When controlling for therapy type, there was no elvidence for an effect of intensity [9] demonstrating that earlier investigations of the relationship may have been inflated.
Furthermore, earlier reviews did not distinguish between the types of activity practiced, simply grouping all types of practice together to represent a generalized practice incorporating the duration of the entire rehabilitation program. They defined an intensive rehabilitation program as ‘more time in rehabilitation’, thus, actually investigating the effect of an accumulated duration of therapy not the effect of an intensive rehabilitation program [3,7-9]. While the number of repetitions completed over a specific time period is the most sensitive measure of intensity, the duration of rehabilitation sessions is the most commonly reported measure in trials investigating the effect of intensity on outcome [4-9]. When the total duration of practice is matched there is strong evidence of a positive non-linear relationship between dose and response, suggesting a small overall benefit of augmented intervention time in therapy (g=0.35; 95% CI (0.26-0.45); Zobs=7.21) [6]. However a more sensitive approach is to calculate the ‘dose’ of extra practice by comparing the difference of ‘time in rehabilitation per day or per week’ provided to the control group compared to the experimental group.
The planned systematic review aims to build on this knowledge by searching for recent randomized trials designed to measure the effect of more practice of the same rehabilitation. It will identify and synthesize evidence of the association between increasing the intensity of rehabilitation and improving activity in stroke survivors and determine the strength of the effect. A meta-analysis will be completed along with further investigation into the relationship between an intensive rehabilitation program and improved activity after stroke. We aim to determine the sensitivity of an intensive rehabilitation program on improving activity as well as explore the issue of how much more practice is necessary. We also aim to determine if a threshold exists to determine the strength of the effect. The information sought in this review will provide unique information relative to previous systematic reviews. Therefore, the specific questions that the methods of this review will address are:
1. Does extra practice per week of the same rehabilitation lead to improved activity in stroke survivors?
2. What is the amount of extra rehabilitation that needs to be provided to achieve an effect?
A systematic review will be carried out (Figure 1) and reporting will adhere to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement [13]. The protocol for the review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) and has the registration number CRD42012003221.
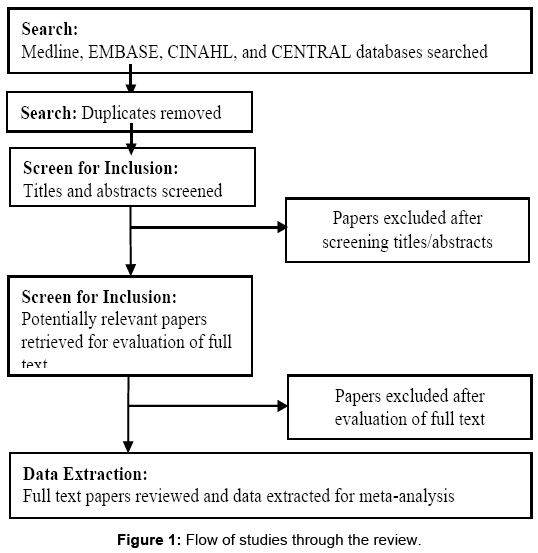
Figure 1: Representative photomicrograph of histopathological features in pulmonary necropsies.
Identification and selection of studies
Searching: The following electronic databases will be searched: Medline, EMBASE, CINAHL, and the Cochrane Central Register of Controlled Trials (CENTRAL). Medical Subject Headings (MeSH) relating to stroke, hemiplegia, physical therapy, occupational therapy, rehabilitation and intensity will be combined with text words in search strategies. An additional documentation file details the search strategy. The MEDLINE search strategy will be adapted for other databases with the assistance of an informed specialist (a medical librarian). One reviewer (ES) will review titles and abstracts of the records identified from the electronic searches and exclude irrelevant studies. Full text versions of the remaining studies will be obtained and two reviewers (ES and NL) will select studies for inclusion based on the pre-specified inclusion criteria (Table 1). Disagreements will be adjudicated by a third reviewer (LA). Trial authors will be contacted for missing study details when required, and reasons for exclusion of full text papers will be documented. Eligible papers will be published in peer-reviewed journals and available in English. No date restrictions will be set. Conference proceedings will not be included.
| Design | •Randomized controlled trials and/or controlled trials. |
| Participants | •Adult age ≥18 years old with a diagnosis of stroke (as diagnosed using any recognized diagnostic criteria) (≥ 80%, others being stroke-like). •Activity limitations affecting walking and/or upper limb ability. |
| Intervention | •Activity limitations affecting walking and/or upper limb ability. |
| Outcome measures | •Performance of activity measured by walking or upper limb ability. |
Table 1: Inclusion criteria.
Characteristics of studies
Design: Randomized and non-randomized controlled trials will be included in this review. For three armed trials and multiple-armed trials comparing different intensities of rehabilitation, we will enter the sample size for the group receiving the most minutes of rehabilitation per week compared to the group receiving the least minutes of rehabilitation per week.
Participants and settings: Participants will be aged 18 years or older. Studies will be included where 80% or more of participants have a diagnosis of stroke (diagnosed using any recognized diagnostic criteria) and loss at the level of activity [14]. Studies will be included if the participants are at any stage of recovery (acute, sub-acute, or chronic) and receiving occupational therapy and/or physical therapy in hospital, rehabilitation or community settings. Study details will be recorded, including the number of participants, age, gender, diagnosis, time since onset of stroke, and type of rehabilitation service (acute,sub-acute or chronic). The number of people recruited to the study, randomized and number of withdrawals will be noted.
Intervention: Interventions must involve active engagement of the participant to promote motor learning. Interventions will be classified as involving active engagement if at least half of the total interventions are targeted at the level of activity, as defined by the International Classification of Function (ICF) [14], and if at least one aim of the intervention is to improve walking ability, upper limb ability and/or both. Activity-specific interventions, such as additional sit-to-stand practice, will be included for comparison as long as both groups received interventions that would result in a similar outcome. Interventions provided to the experimental and control group will be matched at the activity level so that both groups received rehabilitation to practice the same activity in different durations (minutes per day or per week). The minutes of practice received by the control group will be calculated specific to the activity completed during the extra practice they received. Differences in the minutes of practice will be used to calculate percentages of practice provided to both groups. As this review is investigating the effect of extra minutes of rehabilitation per week, a group that does not receive any therapy will not be included. A greater contrast in the duration of intervention time per day/week between the experimental and control groups would most accurately represent the effect of an intensive rehabilitation program.
Outcome measures: The primary outcome of interest is activity. Included outcome measures will assess at the ICF level of activity performance in walking ability and upper limb activity. Assessments of walking ability may include assessment of gait speed (10-m Walk Test in s) and distance (6-min Walk Test in m). Assessments of upper limb activities may include the Nine Hole Peg Test and the Box and Block Test. To check the similarities of the studies we will record the outcome measures used and time points when they were administered. All review authors will assign outcome measures to the domain assessed (walking ability and/or upper limb activities). If data are skewed or more than one outcome measure is used in the same domain from the same study, we will include timed performance tests and the outcome measure most frequently used across included studies. There are no secondary objectives; however, all other outcome measures will be noted.
Two review authors will independently extract study data and record information on a pre-designed data extraction form. Information about the method (design, participants, intervention, outcome measures) and outcome data (number of participants exposed to intensive rehabilitation, mean (SD), walking ability and upper limb ability) will be extracted. Data will be crosschecked and differences resolved by discussion or a third review author as necessary.
Assessment of methodological quality
The methodological quality of studies will be assessed using the PEDro scale [15]. The scale produces a score out of 10 depending on whether the study controlled for the following sources of bias: random allocation; allocation concealment; similarity between groups at baseline, blinding of participants, personnel and outcome assessors; incomplete outcome data and reporting of data. Wherever possible, PEDro scores recorded on the PEDro database will be used. If a study has not been rated by the PEDro team, two review authors will independently score the study and a third review author will resolve any disagreements.
Data analysis
Where there is sufficient homogeneity between studies we will conduct a meta-analysis to determine if more practice per week of the same rehabilitation leads to improved activity after stroke. We will only pool outcome measures in meta-analysis if they are timed performance outcome measures. For continuous outcomes we will calculate Standardized Mean Differences (SMD) using RevMan 5.1 [16]. The immediate post-intervention scores will be used to first conduct a fixed-effects meta-analysis. Heterogeneity will be assessed via visual inspection of the forest plot and consideration of both the chi-squared test and the I-squared statistic. We will apply a randomeffects meta-analysis and conduct a sub-group analysis to assess the impact of heterogeneity on the SMD. In the case of significant statistical heterogeneity (I-squared over 50%) we will conduct a sensitivity analysis and apply a random-effects meta-analysis. We will not pool data if there is considerable variation in the results (I-squared statistic >75%).
We will calculate the percentage of extra practice provided in each trial and, using the SMD, we will calculate a Pearson correlation coefficient to explore the relationship between an increasing intensity of rehabilitation and improved walking and upper limb ability.
The positive or negative effect of increasing the amount of practice will be compared with the total volume of extra practice provided in each trial to conduct a ROC curve calculation. We will conduct a ROC curve calculation to determine the amount of extra rehabilitation that needs to be provided to achieve improved activity in stroke survivors. If there are a sufficient number of comparable studies (four or more), we will perform subgroup analysis to determine if the benefit of extra practice per week is dependent on the type of activity practiced (walking or upper limb activity) or the rehabilitation approach used.
A narrative synthesis summarizing the main findings of all included studies will be provided. It will be structured around the type and duration of rehabilitation, target population characteristics, type of outcome and intervention content. The description of studies will include a measure of stroke severity where available, such as the NIH Stroke Scale. In addition, we will summarize the time since stroke and the amount of rehabilitation stroke patients received compared to the amount planned across the experimental and control conditions, noting any recorded barriers to intervention. We will comment on the format of intervention provided, for example whether it was provided one-to-one or in a group setting.
Dealing with missing data: We will contact trial authors for missing data and convert available data where possible, as recommended by the Cochrane Handbook of Systematic Reviews of Interventions [17].
Unit of analysis issues: The unit of randomization in these trials is the individual patient. The number of participants in the intensive rehabilitation and usual care groups will reflect the two selected experimental groups; the mean and standard deviations will remain unchanged.
This review will explore the complexity that exists between the relationship of an intensive rehabilitation program and improved activity in stroke survivors.
The results of this systematic review will be compared to previous findings with differences and similarities explained. We will additionally compare our findings to data from studies which provide information on actual amounts of therapy provided and to current recommendations regarding the amount of therapy that should be provided in rehabilitation. While this review will provide information on the sensitivity of the optimal dose of therapy, there may be challenges in implementation: workforce shortages, current models of delivery (typically 1:1), patient expectations and motivation, therapist expectations and access to resources.
Findings will thus provide guidance to occupational therapists and physical therapists, inform policy decisions and provide future directions for research. Findings may lead to the development of a rehabilitation program that delivers the ideal opportunity for practice and will help clinicians identify how much extra practice stroke survivors have to do in a rehabilitation program to achieve improved outcomes.