Andrology-Open Access
Open Access
ISSN: 2167-0250
ISSN: 2167-0250
Research Article - (2014) Volume 3, Issue 2
Objective: To investigate the oxidative DNA damage in the seminal plasma and spermatozoa of infertile men with varicocele and to evaluate the potential relationship between oxidative DNA damage and varicocele.
Methods: This case-control study recruited 180 infertile men with varicocele and 199 infertile men without varicocele and 168 fertile male control subjects. Semen parameters, seminal plasma 8-hydroxy-2-deoxyguanosine (8-OHdG) and sperm DNA Fragmentation Index (DFI) were assessed.
Results: Compared to the infertile men without varicocele and control subjects, infertile men with varicocele exhibited lower sperm concentration, lower progressive motility, lower vitality and lower percentage of normal morphology (all P=0.0001). The seminal content of 8-OHdG and sperm DFI were higher in infertile men with varicocele than in infertile men without varicocele and in the control group (all P<0.001). A positive correlation was observed between the 8-OHdG levels and DFI (P<0.001). However, There were negative correlations between seminal plasma 8-OHdG levels or sperm DFI with sperm concentration, progressive motility, vitality, and normal forms in the varicocele group (all P<0.001). Furthermore, the seminal plasma 8-OHdG content and sperm DFI was significantly higher in grades II and III than in grade I after controlling age, BMI, abstinence period and semen parameters.
Conclusions: Infertile men with varicocele have greater oxidative DNA damage in seminal plasma and spermatozoa than the subjects without varicocele. The degrees of varicocele and DNA damage were associated with decreased semen quality in infertile men with varicocele.
<Keywords: 8-Hydroxy-2-deoxyguanosine; DNA fragmentation index; Oxidative DNA damage; Infertility; Varicocele
Varicoceles are present in 15 percent of the adult male population and in approximately 40 percent of men presenting with infertility. Varicoceles are thought to progressively reduce spermatogenesis via elevated intratesticular temperature and altered testicular blood flow; the decreased supply of oxygenated blood and nutrients to the sperm production sites reduces sperm quality and quantity, and consequently, their fertility capacity [1]. Varicoceles are also highly associated with increased oxidative stress, which may also diminish sperm function through sperm membrane and DNA damage [2].
Seminal plasma is well endowed with an array of anti-oxidant defense mechanisms to protect spermatozoa against oxidants. Antioxidants that are present in the seminal plasma compensate for the deficiency in cytoplasmic enzymes in the spermatozoa [3]. Several studies suggested relationships between oxidative stress and male infertility. Infertility can be caused by an imbalance between Reactive Oxygen Species (ROS) and seminal antioxidants in the semen, resulting in oxidative stress and spermatozoa damage [3]. Many markers can be used to assess the spermatozoa oxidative stress and semen. Of them, 8-hydroxy-2-deoxyguanosin (8-OHdG) is widely considered as one of those markers of oxidative DNA damage [4].
Oxidative stress to sperm DNA increases DNA fragmentation and causes transition mutagenesis due to an increased content of 8-OHdG [5]. Some studies have shown that the 8-OHdG level in sperm is closely associated with the presence of antioxidants in semen and that oxidative damage to sperm DNA might be important in the cause of male infertility [6,7].
Oxidative stress in association with varicocele might cause sperm DNA damage and sperm apoptosis. However, the oxidative DNA damage in infertile men with varicocele remains poorly understood.
The objective of the present study was to determine the oxidative DNA damage in seminal plasma of infertile men with varicocele, and to explore the potential correlation between oxidative DNA damage and sperm quality.
Participating subjects
The present study was designed as a case-control study. The research subjects were recruited from the clinic unit of the Guangdong Family Planning Science and Technology Institute in 2010 and were entered into this study following written informed consent. The study protocol and the consent procedure were approved by the Human Ethics Committee of Guangdong Family Planning Science and Technology Institute. Infertility was defined as the failure to conceive after more than 12 months of unprotected intercourse with the same partner. Diagnosis of varicocele was based on local examination of both testicles and spermatic cords in addition to Doppler ultrasonography. Varicoceles were graded according to the criteria described by the World Health Organization manual [8]. Graded I, the varicocele could only be palpated after the valsalva maneuver in the upright position; graded II, the varicocele was easily palpable but not visible; and graded III, the varicocele was easily visible. As listed in Table 1, One hundred and eighty infertile men with varicocele (varicocele group) have an average age of 34.9 ± 5.3 years and infertility duration of 5.2 ± 3.6 years. The varicocele group was divided into three subgroups-grade I, grade II and grade III varicocele-consisting of 45, 48, and 87 cases, respectively. One hundred and ninety-nine infertile men without varicocele have an average age of 34.9 ± 5.3 years and infertility duration of 4.6 ± 5.4 years. The control group consisted of one hundred and sixty-eight fertile male volunteers with an average age of 34.1 ± 6.0 years, who had no history of varicocele or fertility problems.
| Variable | Control group (n=168) | Infertile group without varicocele(n=199) | Varicocele group (n=180) | Sig. | |||
|---|---|---|---|---|---|---|---|
| mean | Std. Deviation | mean | Std. Deviation | mean | Std. Deviation | ||
| Age | 34.09 | 5.97 | 34.95 | 5.31 | 34.93 | 5.25 | 0.246 |
| BMI | 22.27 | 2.34 | 22.71 | 2.63 | 22.66 | 2.52 | 0.202 |
| Sperm concentration106/ml) | 56.26 | 38.21 | 44.74 | 28.74 | 38.43 | 30.95 | 0.000 |
| Progressive motility (%) | 58.97 | 11.2 | 45.17 | 12.88 | 27.53 | 14.83 | 0.000 |
| Vitality (%) | 68.86 | 11.52 | 54.11 | 12.48 | 36.71 | 14.77 | 0.000 |
| Normal forms (%) | 17.08 | 8.36 | 12.89 | 4.96 | 7.06 | 5.39 | 0.000 |
| seminal 8-OHdG(ng/ml) | 19.27 | 5.01 | 19.57 | 5.95 | 22.39 | 5.01 | 0.000 |
| Sperm DFI (%) | 21.73 | 9.49 | 29.09 | 9.62 | 35.15 | 10.71 | 0.000 |
BMI: Body Mass Index; 8-OHdG: 8-hydroxy-2-deoxyguanosine; DFI: DNA Fragmentation Index
Table 1: Characteristics and semen parameters in varicocele and control groups.
Semen parameter analysis
All specimens were collected in sterile plastic containers by masturbation after an abstinence period of 3-5 days and were analyzed within 1 h of collection. At least two semen samples for each subject were collected, with a one-month interval between collections. Semen parameters were analyzed according to the World Health Organization guidelines [9]. After allowing at least 30 min for liquefaction, semen samples were subjected to analysis of semen volume, sperm motility, vitality, sperm concentration, and sperm morphology. The semen volume of the ejaculate was measured by weighing the sample collected in the vessel. To determine the percentage of sperm motility, a 10 μl sample was placed onto a clean glass slide and covered with a 22 ×22 mm coverslip. The preparation was allowed to stabilize for 10 min and analyzed in a 20 μl depth chamber. The preparation was then examined at 400x magnification at 37°C using a phase-contrast microscope. The microscopic field was scanned systematically and sperm motility was graded as Progressive Motility (PR), Non-Progressive Motility (NP), and Immotility (IM). Sperm motility (as a percentage) was calculated as 100× (PR+NP)/(PR+NP+IM). At least 200 spermatozoa per sample were assessed. Vitality was measured using eosin–nigrosin. The sperm concentration was determined using the haemocytometer. The sperm morphology was assessed after slide staining with the modified papanicolaoustaining method with strict criteria.
Following semen analysis, the samples were centrifuged at 1000 g for 10 min at room temperature. The pellets of each sample were resuspended in 0.2 ml physiological saline. 1 ml of the seminal plasma (supernatant) and pelleted sperm were then frozen at -80°C for future experiments [10].
Oxidative DNA damage measurement
To measure oxidative damage to sperm DNA, the seminal plasma 8-hydroxy-2-deoxyguanosine (8-OHdG) and sperm DNA integrity were tested.
The seminal plasma levels of 8-OHdG, a biomarker of DNA damage, were determined by the Enzyme-Linked Immunosorbent Assay (ELISA) method using a competitive enzyme-linked immunosorbent assay kit (New 8-OHdG Check, Japan Institute for the Control of Aging, Fukuroi, Shizuoka) at 450 nm wavelength, according to manufacturer protocol. Seminal plasma levels of 8-OHdG were presented as ng/ml.
Sperm DNA integrity was evaluated by the Sperm Chromatin Structure Assay (SCSA), which tests the susceptibility of sperm DNA to acid-induced denaturation and the values are expressed as sperm DNA Fragmentation Index (DFI: percentage of sperm with denatured nuclei) [11]. It is a potential parameter for fertility investigation [12]. A minimum of 5000 cells from 2 aliquots of each sample were analyzed using the FACSCalibur flow cytometer (Becton Dickinson, San Jose, California) interfaced with a data handler (CELLQUEST 3.1; Becton Dickinson). WinList (Verity Softwarehouse Inc, Topsham, Maine) was used to generate the cytogram (red vs. green fluorescence) and histogram (total cells vs. DFI) plots, as well as DFI reading. The variability of the replicate of DFI measures was less than 5%.
Sample size was powered for a difference of approximately 1 Standard Deviation (SD) between the fertile and infertile groups. Values were expressed as mean ± SD. Skewed distribution of variables was normalized by square root or logarithmic transformation as appropriate. One-way ANOVA test was used to evaluate the difference between groups. Dunnett T3 test was used to show the difference within the groups. Generalized linear models were used to assess the combined effects of all variables of the semen parameters. The significance level was defined as P<0.05. Pearson linear correlation was also used. All analyses presented in this report were performed with SPSS 15.0 (SPSS, Inc, Chicago, IL, USA).
Comparison of general semen parameters and 8-OHdG levels in seminal plasma between infertile men with varicocele and fertile men
The general characteristics and semen parameters of the infertile men with varicocele, infertile men without varicocele and control groups are shown in Table 1. Age, Body Mass Index (BMI), and semen volume among the varicocele, infertile men without varicocele and control groups did not differ significantly (P>0.05). Compared to the control subjects, infertile men with varicocele and infertile men without varicocele exhibited significantly lower sperm concentration (38.43 ± 10.95, 44.74 ± 28.74 vs. 56.26 ± 38.21 million/mL), progressive motility (27.53 ± 14.83, 45.17 ± 12.88 vs. 58.97 ± 11.20%), vitality (36.71 ± 14.77, 54.11 ± 12.48 vs. 68.86 ± 11.52%), normal morphology (7.06 ± 5.39, 12.89 ± 4.96 vs. 17.08 ± 8.36%, all P<0.001).
To examine oxidative DNA damage status, we measured seminal plasma levels of 8-OHdG and sperm DFI. As shown in Table 1, the seminal content of 8-OHdG was greater in the varicocele group (22.39 ± 5.01 ng/ml) than in the infertile men without varicocele group (19.57 ± 5.95 ng/ml, P <0.001) and in the control group (19.27 ± 5.01 ng/ml, P<0.001). The infertile men with varicocele exhibited higher DFI than in the infertile men without varicocele group and control group (35.15 ± 10.71 vs 29.09 ± 9.62, 21.73 ± 9.49%).
Association of 8-OHdG content and DNA fragmentation index with semen quality in infertile men
Using Pearson’s linear correlation, significant negative correlations were found between seminal plasma 8-OHdG levels and sperm concentration (r=-0.261, P<0.001), Progressive motility (r=-0.328, P<0.001), vitality (r=-0.336, P<0.001), and normal forms (r=-0.253, P<0.001) in the infertile men (Figure 1).
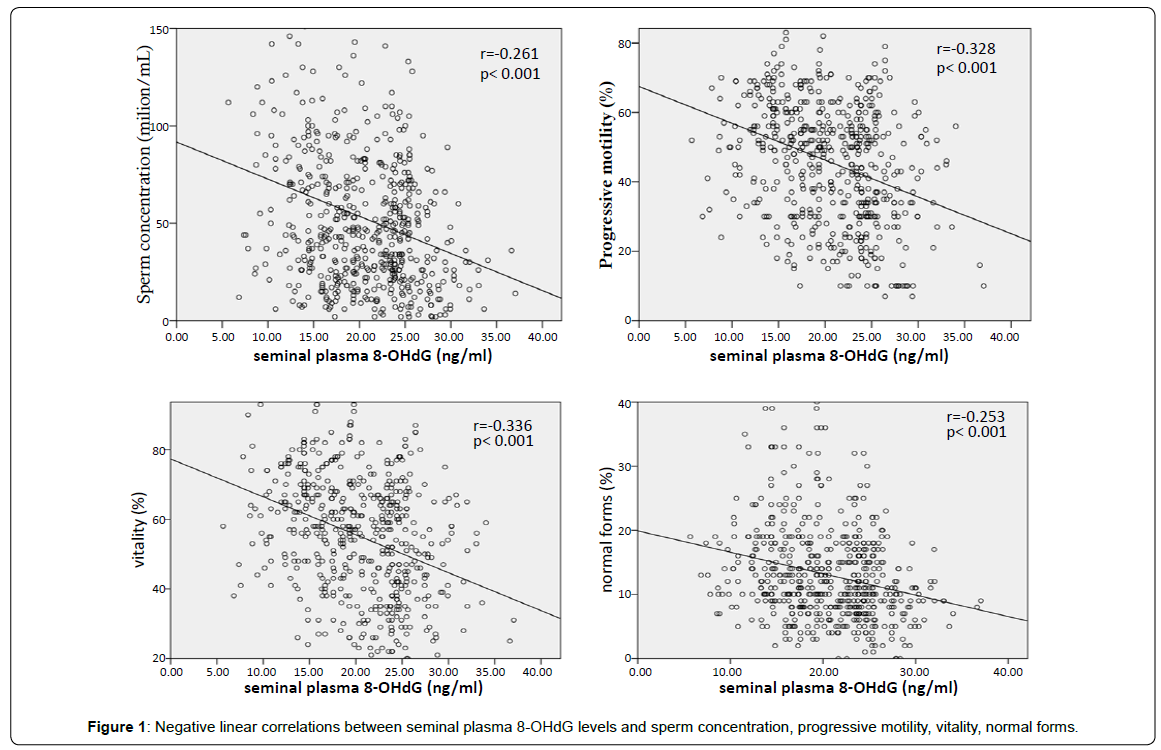
Figure 1: Negative linear correlations between seminal plasma 8-OHdG levels and sperm concentration, progressive motility, vitality, normal forms.
There were significant negative correlations between sperm DFI and sperm concentration (r=-0.155, P<0.001), progressive motility (r=- 0.612, P<0.001), vitality (r=-0.626, P<0.001), and normal forms (r=- 0.626, P<0.001) in the infertile men (Figure 2).
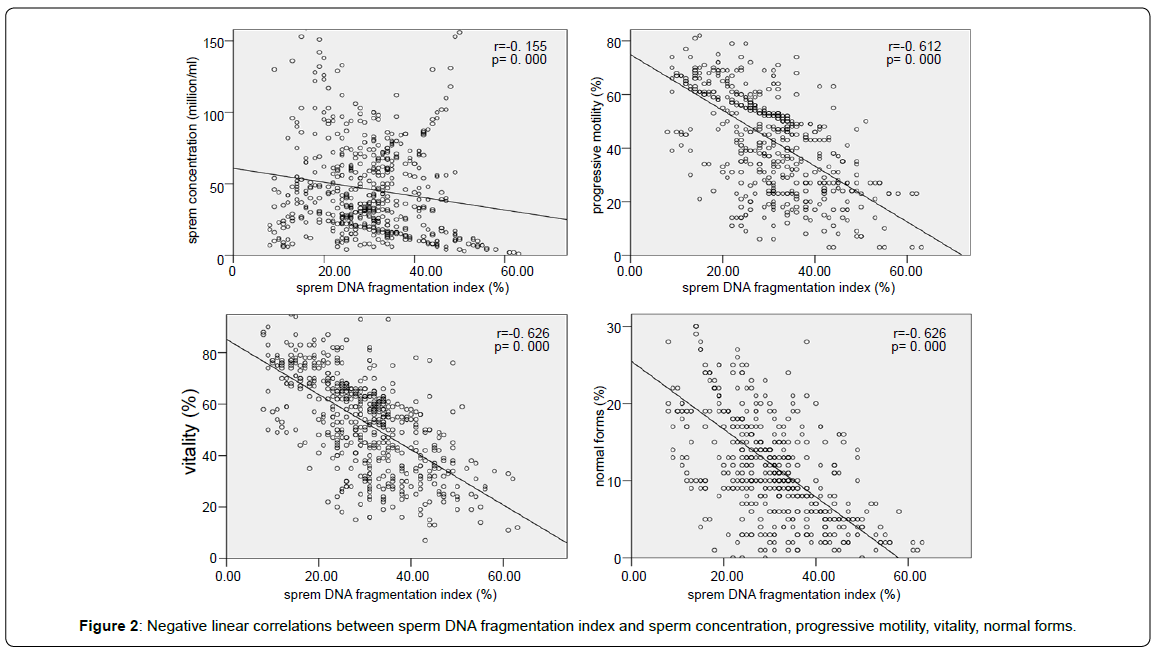
Figure 2: Negative linear correlations between sperm DNA fragmentation index and sperm concentration, progressive motility, vitality, normal forms.
There were significant positive correlations between seminal plasma 8-OHdG levels and DFI(r=0.669, P< 0.001) (Figure 3).
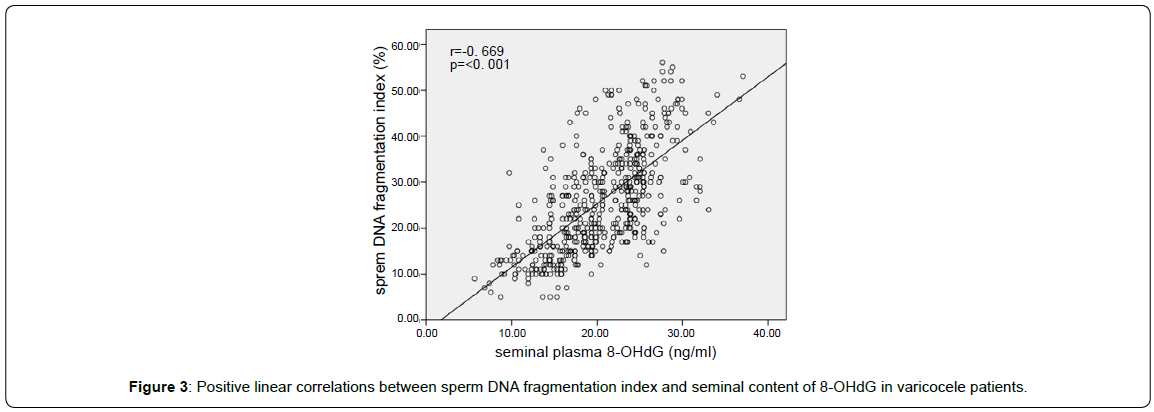
Figure 3: Positive linear correlations between sperm DNA fragmentation index and seminal content of 8-OHdG in varicocele patients.
Association of 8-OHdG content and DNA fragmentation index with varicocele grade in infertile men
As the variances of the 8-OHdG content and DFI in the varicocele subgroups were nonhomogeneous, the post hoc Dunnett T3 test was used to determine differences within the groups. Given unequal variances, differences were defined by pairwise tests at a 0.05 significance level and 95% confidence interval.
The levels of 8-OHdG and DFI were significantly higher (all of the mean differences >0, P<0.05) in grades II and III than in the infertile men without varicocele group (Figure 4A and 4B).
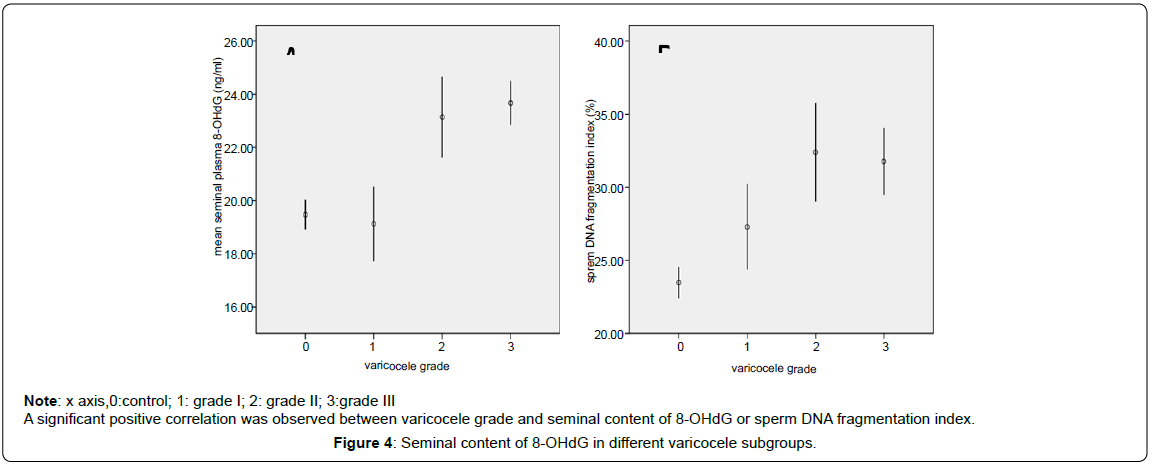
Figure 4: Seminal content of 8-OHdG in different varicocele subgroups.
Controlling age, BMI, abstinence period, semen parameters, the seminal plasma 8-OHdG content and sperm DFI were significantly higher in grades II and III than in grade I (Table 2).
| Variable | Varicocele grade | Adjusted Mean | Std. Error | 95% Wald CI | Wald Chi-Square | Sig. | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Seminal 8-OHdG | grade III | 24.01 | 0.48 | 23.08 | 24.94 | 40.892* | 0.000 |
| grade II | 22.71 | 0.67 | 21.41 | 24.02 | 18.269* | 0.000 | |
| grade I | 18.61 | 0.69 | 17.26 | 19.97 | |||
| Sperm DFI | grade III | 38.03 | 1.08 | 35.91 | 40.16 | 14.736* | 0.000 |
| grade II | 33.66 | 1.52 | 30.68 | 36.64 | 5.427* | 0.020 | |
| grade I | 30.64 | 1.58 | 27.56 | 33.73 | |||
#controlling for age, BMI, abstinence period, volume, sperm concentration, PR, vitality and normal form.
*comparing with the grade I group
Table 2: Comparison of seminal 8-OHdG levels and sperm DFI among the varicocele subgroups#.
Varicocele is the leading cause of male infertility due to its impairment of spermatogenesis through several distinct pathophysiological mechanisms [13]. The pathology of varicocele is characterized by the dilatation and tortuosity of the pampiniform plexus, leading to higher temperature of the testes and thereby testicular atrophy with infertility. The seminal plasma of patients with varicocele has excessive oxidative stress, even in men with normospermia [14,15]. Seminal plasma 8-OHdG is a sort of common biomarker of oxidative stress [16]. The assay of sperm 8-OHdG might have potential diagnostic value in the evaluation of sperm function and male fertility [17]. Varicoceles have been associated with high levels of sperm DNA damage [18]. The present study showed that infertile men with higher varicocele grade exhibit higher 8-OHdG levels in seminal plasma and higher DFI than patients with varicocele grade I or those infertile men without varicocele or the fertile men and the sperm DFI was positively correlated with the 8-OHdG levels in seminal plasma for the patients with varicocele. Sakamoto Y et al. [15] addressed that the seminal plasma of patients with varicocele was under excessive oxidative stress, and partly even in patients with normospermia, and that the level of 8-OHdG reduced from 10.3 μmol/L to 6.2 μmol/L after varicocelectomy. The patients with a varicocele may also have a diminished seminal antioxidant capacity and sperm DNA fragmentation increases [19].
The present study also showed that the seminal 8-OHdG level and sperm DFI were significantly negatively correlated the sperm parameters (sperm concentration, progressive motility, vitality and normal form) and varicocele grade, after adjustment for potential confounding factors including age, BMI. These findings suggest the sperm quality of varicocele patients is correlated with the seminal oxidative pressure which lead to the oxidative sperm DNA damage, though the mechanisms remain to be clarified.
Sperm DNA damage may occur by at least one of three fundamental mechanisms: defective chromatin condensation or abortive apoptosis during spermatogenesis or transportation of sperm through the male or the female genital tract [17]. Increased Reactive Oxidative Species (ROS) levels in seminal plasma are strongly correlated with varicocele degree and are reported to decrease after varicocelectomy [20,21]. The present study also documented that varicocele degree are positively correlated with seminal plasma 8-OHdG level and sperm DFI in the varicocele group.
Morphologically abnormal spermatozoa and leukocytes are the main sources of ROS in the seminal plasma [22,23]. Due to higher seminal levels of ROS, infertile men with varicocele may therefore exhibit greater spermatozoa DNA damage [23]. DFI provides additional information about the potential for fertility and shows less biological variation when compared to conventional semen analysis [24]. Studies included in the meta-analysis demonstrated a strong correlation between semen parameters and ROS concentrations [25].
The present study possesses several limitations. This study did not include questionnaires about the dietary habits or daily physical activity of the subjects. The outcome of this study did not include follow-up on pregnancy. These potential confounding factors should be eliminated in future studies. Further investigation is also needed to reveal the cause and effect relationship between seminal plasma 8-OHdG levels and varicocele pathology, as well as the underlying mechanisms.
In conclusion, the present study demonstrates that infertile men with varicocele grade have greater oxidative DNA damage than the infertile patients without varicocele and fertile men, and that these changes are positively correlated with varicocele grade. This study therefore provides important insight into the role of oxidative stress in varicocele-associated infertility, and highlights the need for intervention trials to correct the spermatozoa oxidative damage and sperm abnormalities in infertile men with varicocele.
Li-xin Tang and Qi-ling Wang concepted and designed the study, collected the data, performed the statistical analysis and drafted the first version of the manuscript. All other co-authors took part in analysis and interpretation of data and revision of the manuscript, and all approved the final version of the manuscript.
This study was supported by funding from Guangdong Province Science and Technology Project of China (to LXT). The authors are grateful to the study participants, the staff of the infertility clinic. The authors would like to thank Professor David Ke for critically reviewing the manuscript.