Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Review Article - (2015) Volume 5, Issue 3
Selecting patients of appropriate risk is a seminal element of any clinical trial methodology. However, inappropriate risk markers may result in selecting patients with unintended risk levels. We aimed to review systematically the outcomes of randomized clinical trials of antithrombotics in acute coronary syndromes (ACS) in relation to the inclusion risk markers, dividing them into groups reflecting increased hemodynamic (for example Killip>1, ejection fraction<40%) or bleeding risks (for example renal failure, elderly age). According to our analysis, the trials including increased bleeding risk selection criteria were significantly related to the trial outcome of increased bleeding.
Conclusions: Results of antithrombotic trials in ACS may be related to the kind of patients’ selection criteria rather than the drug efficacy/safety. We also provide a conceptual basis for avoiding the pitfalls, which will help future researchers to design and carry out robust studies. Implications for clinical practice, sponsors and regulators are highlighted.
Keywords: Acute coronary syndromes; Clinical trial; Drug therapy; Systematic review; Enrichment
There are a growing proportion of antithrombotic clinical trials in acute coronary syndromes (ACS), which by so called “enrichment” design include patients with higher baseline risk for primary outcomes. This is one of the critical aspects of any trial design, regulated by Food and Drug Administration draft guidance [1]. The enrichment ensures increased number of relevant events within a smaller population. In practice it is attained by adding various combinations of higher risk entry criteria, including: acute heart failure, lower ejection fraction, diabetes, elderly age, impaired renal function, TIMI or GRACE risk scores, etc, according to the classic concept of risk (more risk markers=higher risk).
The efficacy of any antithrombotic drug in ACS is a derivative of a dichotomous drug potential (antithrombotic/pro-bleeding) and a given patient dichotomous risk structure (susceptibility to bleeding/potential for hemodynamic improvement) (Figure 1). However, many markers of cardiovascular risk overlap with those of bleeding. The use of undifferentiated high risk markers may lead to an unintended selection of patients, for example more susceptible to bleeding but with trivial ACS (left upper quadrant of Figure 1), which may likely shift the study outcomes towards more harm than benefit of potent antithrombotic therapies. On the other hand, the selection of patients with large hemodynamic threat but low risk for bleeding (right lower quadrant of Figure 1) may “inflate” the efficacy and conceal complications of the therapy tested. These scenarios suggest that uncontrolled choice of the trial selection criteria may influence the study outcomes rather than the drug action, creating opportunities for either intentional or unintentional trial misconduct.
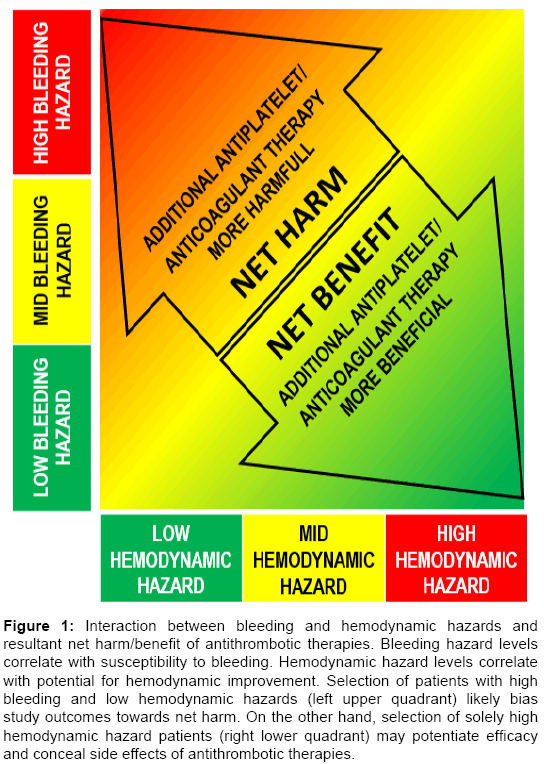
Figure 1: Interaction between bleeding and hemodynamic hazards and resultant net harm/benefit of antithrombotic therapies. Bleeding hazard levels correlate with susceptibility to bleeding. Hemodynamic hazard levels correlate with potential for hemodynamic improvement. Selection of patients with high bleeding and low hemodynamic hazards (left upper quadrant) likely bias study outcomes towards net harm. On the other hand, selection of solely high hemodynamic hazard patients (right lower quadrant) may potentiate efficacy and conceal side effects of antithrombotic therapies.
We previously introduced a multidimensional risk management concept for ACS [2]. The novel approach differentiates bleeding and hemodynamic hazards allowing conscious management of these contradictory sources of threat. Basically, it divides the high risk markers into subgroups reflecting either hemodynamic (impaired ejection fraction, acute heart failure, large jeopardized myocardial territory) or bleeding hazards (elderly age, anemia, renal impairment, diabetes).
We hypothesized that the multidimensional risk management concept for ACS may be relevant for enrichment strategies in antithrombotic trials in ACS. Specifically, we evaluated whether the kind of selection criteria, reflecting bleeding and hemodynamic hazards, were related to the safety and efficacy of a trial, respectively.
The studies were selected according to PRISMA recommendations (Appendix 1). We identified randomized multicenter cardiovascular clinical trials reflecting the contemporary practice of care in acute coronary syndromes, i.e. double antiplatelet therapy, and intended invasive management of the majority of patients, percutaneous intervention with routine stenting, fulfilling additional criteria – (1) primary efficacy endpoints based on “hard” clinical events including: death, myocardial infarction, revascularization, heart failure, objective ischemia, re-hospitalization for ischemia, or combination thereof, (2) predefined primary safety endpoints, (3) in the case of mixed population (stable/unstable coronary disease) the majority of patients with acute coronary syndromes. We excluded trials referring to the patients’ transfer strategies, or solely timing or drug dosages [3-26]. Out of 1897 publications reviewed on Pubmed database and 646 studies reviewed on www.clinicaltrials.gov, we identified 24 clinical trials fulfilling the above criteria.
Subsequently, we reviewed the inclusion criteria of the trials and recorded all additional inclusion criteria intended to increase the risk for the study patients such as (1) acute heart failure (defined as either Killip class>1, or descriptive), (2) prior myocardial infarction, (3) low ejection fraction (<40%) or heart failure (NYHA class>I), (4) non-revascularized multivessel coronary disease, (5) TIMI risk score characteristics (includes diabetes), (6) diabetes, (7) peripheral arterial disease, (8) stroke history, (9) elderly age (one trial age>55, 2 trials age>60, 9 trials age>65), and (10) renal insufficiency (GFR<60 ml/min × 1.73m²). Based on the analysis of GRACE risk score, HAS-BLED, CRUSADE or ACUITY bleeding risk scores, as well as our previous analysis, we prospectively identified the inclusion criteria of numbers 5 to 10 as reflecting an increased bleeding hazard, likely to impact the treatment safety [27-30]. The hemodynamic hazard characteristics (criteria 1 through 5) were regarded as reflecting an increased hemodynamic burden of the index ischemic event, potentially improvable by the ACS treatment.
Baseline patients’ characteristics were collected from available published data, and for all studies included median age, gender and diabetes prevalence.
The primary efficacy, safety and net outcomes were collected for each trial and were categorized into either significantly different or not between the treatment versus the comparator groups. The primary outcomes of all trials were composites, and in all cases included death or recurrent ACS, in some cases additional stroke, coronary revascularization, heart failure, rehospitalization for ischemia.
For the purpose of the current analysis, we defined the following outcomes according to the current consensus referring to antithrombotic studies in ACS:
Safety
1. Positive primary safety outcome (decreased bleeding)
2. Negative primary safety outcome (increased bleeding)
3. Neutral primary safety outcome (no significant impact on bleeding)
Efficacy
1. Positive primary efficacy outcome (decreased event rate)
2. Negative primary efficacy outcome (increased event rate)
3. Neutral primary efficacy outcome (no significant impact on event rate)
Net
1. “Net harm” comprising either negative safety outcome+neutral or negative efficacy outcome, OR negative efficacy outcome+neutral safety outcome.
2. “Net benefit” comprising either positive safety outcome+positive or neutral efficacy outcome, OR neutral safety outcome+positive efficacy outcome.
3. “Net neutral” comprising both neutral safety and efficacy outcomes, OR positive safety outcome+negative efficacy outcome, OR negative safety outcome+positive efficacy outcome.
Early termination of a trial for safety reasons was treated as “negative primary safety outcome”.
Given that the expected impact of a trial design on the outcomes should be most pronounced within trials testing new therapies added to the standard of care, we separately analyzed a subset of “on-top-of ” trials.
Statistics
Continuous variables are presented as medians (25th, 75th quartiles) and are compared with the Mann-Whitney test. Categorical variables are presented as numbers/proportions and compared with Fisher’s exact test. Logistic regression was performed for establishing the odds ratio (OR) and 95% confidence interval for the predictive value of the analyzed risk markers, and for presenting the primary safety and efficacy outcomes of the trials. A value of P<0.05 was considered nominally significant. Because of the small number of the trials, no statistical interaction tests and multivariable analyses were performed. All analyses were performed with the Medcalc Ver.13.1.0.0. (MedCalc Software, Ostend, Belgium) statistical software.
There were 24 trials of 16 drugs within 6 therapeutic groups, which enrolled 158,989 patients. A reduction of the primary efficacy outcome was shown in 4 (17%) of the trials, and an increased event rate in 2 (8%). The primary safety outcome (bleeding) reduction was observed in 2 (8%) trials, and in 14 (58%) studies the safety outcomes were worse for the treatment studied. “Net harm” of the therapy analyzed was reported in 13 (54%) cases, whereas “net benefit” in 4 (17%), including the two cases with improved safety (Figure 2).
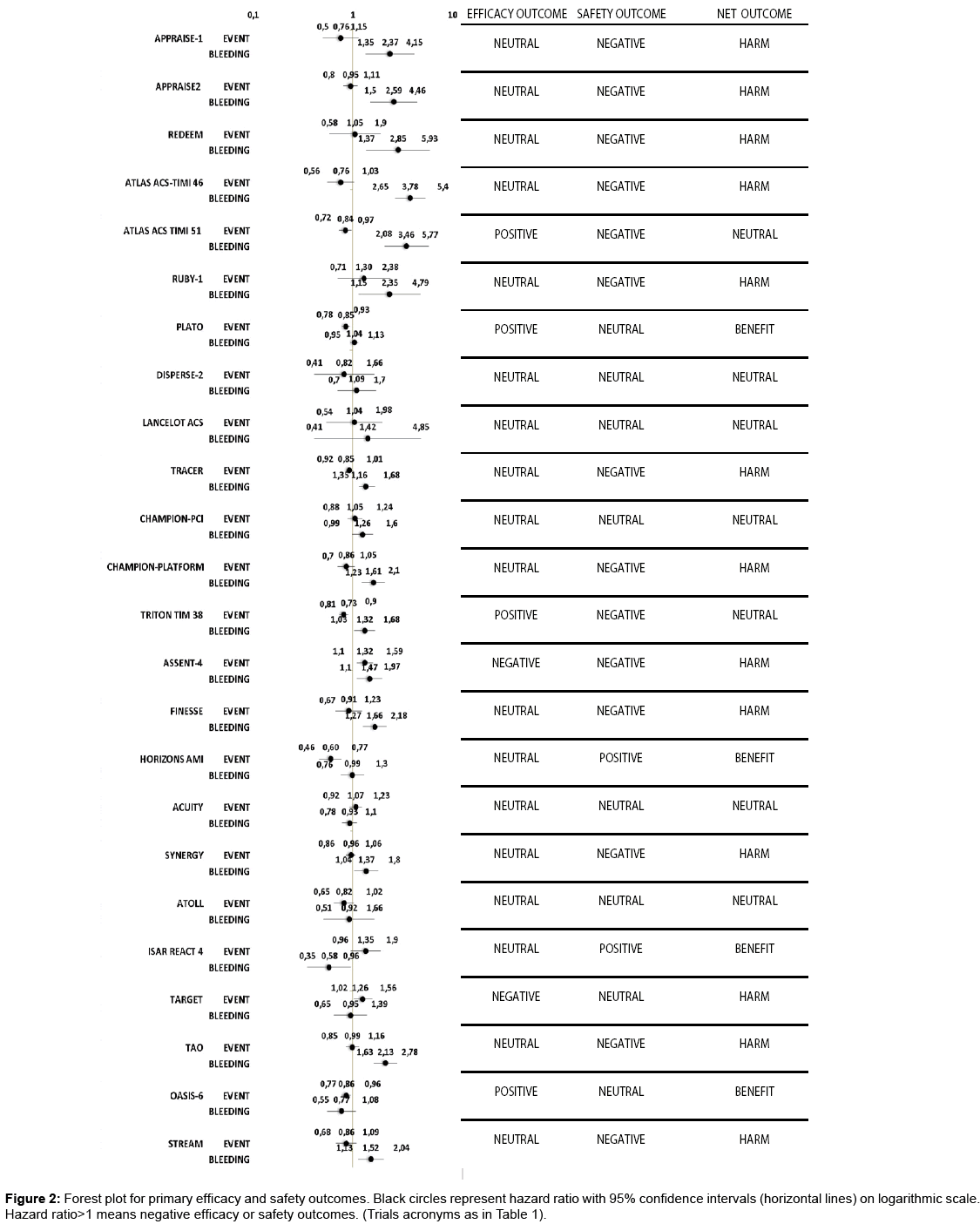
Figure 2: Forest plot for primary efficacy and safety outcomes. Black circles represent hazard ratio with 95% confidence intervals (horizontal lines) on logarithmic scale. Hazard ratio>1 means negative efficacy or safety outcomes. (Trials acronyms as in Table 1).
The obligatory additional risk modifying entry criteria were present in the majority, of 14 (58%) trials, including bleeding hazard in 14 trials and hemodynamic hazard in 10 of the trials. Four trials had solely bleeding hazard, and none had solely hemodynamic hazard markers (Table 1).
| # | Acronim | Number of patients | Therapy/phase | On top=1 other=2 |
Indication | Obligatory additional inclusion risk factor | |
|---|---|---|---|---|---|---|---|
| Bleeding risk (n) | CV risk (n) | ||||||
| 1 | APPRAISE-1 [3] | 1715 | Apixaban/2 | 1 | STEACS or non-STEACS | 5 | 3 |
| 2 | APPRAISE-2 [4] | 7392 | Apixaban/3 | 1 | STEACS or non-STEACS | 5 | |
| 3 | REDEEM[5] | 1861 | Dabigatran/2 | 1 | STEACS or non-STEACS | 4 | 2 |
| 4 | ATLAS ACS-TIMI 46[6] | 3491 | Rivaroxaban/2 | 1 | STEACS or non-STEACS or unstable angina | 2 | 1 |
| 5 | ATLAS ACS TIMI 51[7] | 15524 | Rivaroxaban/3 | 1 | STEACS or non-STEACS or unstable angina | 1 | 1 |
| 6 | RUBY-1[8] | 1279 | Darexaban/2 | 1 | STEACS or non-STEACS | 4 | 2 |
| 7 | PLATO[9] | 18624 | Ticagrelor/3 | 2 | STEACS or non-STEACS | 5 | 2 |
| 8 | DISPERSE-2[10] | 990 | Ticagrelor/2 | 2 | non-STEACS | 0 | 0 |
| 9 | LANCELOT ACS[11] | 603 | Atopaxar/2 | 1 | non-STEACS | 0 | 0 |
| 10 | TRACER[12] | 12944 | Vorapaxar/3 | 1 | STEACS or non-STEACS | 3 | 1 |
| 11 | CHAMPION-PCI[13] | 8877 | Cangrelor/3 | 2 | Stable angina, or STEACS or non-STEACS or unstable angina | 2 | 0 |
| 12 | CHAMPION-PLATFORM[14] | 5362 | Cangrelor/3 | 2 | non-STEACS or unstable angina | 2 | 0 |
| 13 | TRITON TIMI 38[15] | 13608 | Prasugrel/3 | 2 | STEACS or non-STEACS or unstable angina | 2 | 1 |
| 14 | ASSENT-4[16] | 1667 | facilitated PCI with tenecteplase/3 | 1 | STEACS | 0 | 0 |
| 15 | FINESSE[17] | 2452 | facilitated PCI with reteplase/3 | 1 | STEACS | 1 | 0 |
| 16 | HORIZONS AMI[18] | 3602 | Bivalirudin/3 | 2 | STEACS | 0 | 0 |
| 17 | ACUITY[19] | 13819 | Bivalirudin/3 | 2 | non-STEACS | 2 | 1 |
| 18 | SYNERGY[20] | 10027 | Enoxaparin/3 | 2 | non-STEACS | 1 | 0 |
| 19 | ATOLL[21] | 910 | Enoxaparin/3 | 2 | non-STEACS | 0 | 0 |
| 20 | ISAR REACT 4[21] | 1721 | Bivalirudin/4 | 2 | Stable angina or non-STEACS | 0 | 0 |
| 21 | TARGET [23] | 5308 | Tirofiban/3 | 2 | Stable angina or non-STEACS | 0 | 0 |
| 22 | TAO[24] | 13229 | Otamixaban/3 | 2 | STEACS or non-STEACS | 0 | 0 |
| 23 | OASIS-6[25] | 12092 | Fondaparinux | 3 | STEACS or non-STEACS | 0 | 0 |
| 24 | STREAM[26] | 1892 | Tenecteplase | 3 | STEACS | 0 | 0 |
Table1: Cardiovascular trials of antithrombotic, anticoagulant, thrombolytic drugs in acute coronary syndromes.
The median age of the study patients was 62.0(61.0-63.0) years, diabetes was present on average in 24.0(18.6-29.9)% of the patients, and the mean percentage of women among the participants studied was 26.1(23.3-29.3)%. Patients with diabetes were more common among studies with versus without additional bleeding high risk criteria [28.6 (22.5-31.3) versus 19.4 (16.5-25.0), respectively, p=0.012]. There were no differences in age or of female sex prevalence between the groups.
Additional bleeding hazard markers and safety outcomes
Increased bleeding occurred more often among the trials incorporating additional entry bleeding hazard markers (11/14 as compared to 3/10 of the other trials) (Figure 2A) (OR 8.6; 95% CI: 1.3- 55.0, p=0.024). Although out of 13 “net harm” outcomes, 11 were based solely on increased bleeding events (p=0.003), the correlation of the net outcome with additional bleeding entry criteria did not reach statistical significance (OR 2.7; 95% CI: 0.5-14.4, p=0.244), the proportions are presented in Figure 2B.
The incidence of bleeding was higher within the “on-top of ” therapies than in the others (Figure 2C) (OR=22.5; 95% CI: 2.1- 238.1, p=0.010). Similarly, “net harm” was strongly predicted by the “on-top of ” type of trials (OR=15.0; 95% CI: 2.0-111.1, p=0.008), the proportions are presented in Figure 2D. Within the 11 trials testing the new therapy on-top-of routine treatment in 8 of 8 cases with additional bleeding criteria, excessive bleeding was ascertained as compared to 2 of 3 trials without additional bleeding criteria (p=0.273). With regard to “net harm” outcome, it was ascertained in 7 of 8 cases with additional bleeding criteria versus 2 of 3 trials without additional bleeding criteria (p=0.491).
The trials with worse bleeding outcomes tended to have more additional inclusion bleeding risk factors than those with neutral or improved bleeding outcomes (2 [1-4] versus 0 [0-2], respectively, p=0.058). The median number of bleeding risk factors for trials with “net harm” tended to be slightly higher than that for the other studies (2 [0-4] versus 0 [0-2], respectively, p=0.1995). Of the four trials with only bleeding risk additional criteria, one showed neutral outcome (impact on no outcomes) and three were harmful, all due to increased bleeding.
Additional hemodynamic hazard markers and efficacy outcomes
Improved clinical outcomes tended to be more often related to the trials with additional hemodynamic hazard factors than to those without (3/10 versus 1/14, respectively) (Figure 2D) (OR=5.6; 95%CI: 0.5-64.1, p=0.168). However, “net benefit” was observed with the same frequency irrespective of the group (2/10 with versus 3/14 without an additional hemodynamic hazard factor) (Figure 2E).
The trials representing the efficacy event reduction did not have more hemodynamic hazard factors than those without an event reduction (1 [1-2] versus 0 [0-1], respectively, p=0.290). Likewise, the number of hemodynamic hazard factors was not different between the groups with regard to “net benefit” outcome (0 [0-1] versus 0 [0-1] for groups without versus those with “net benefit” respectively, p=0.877) Figure 3.
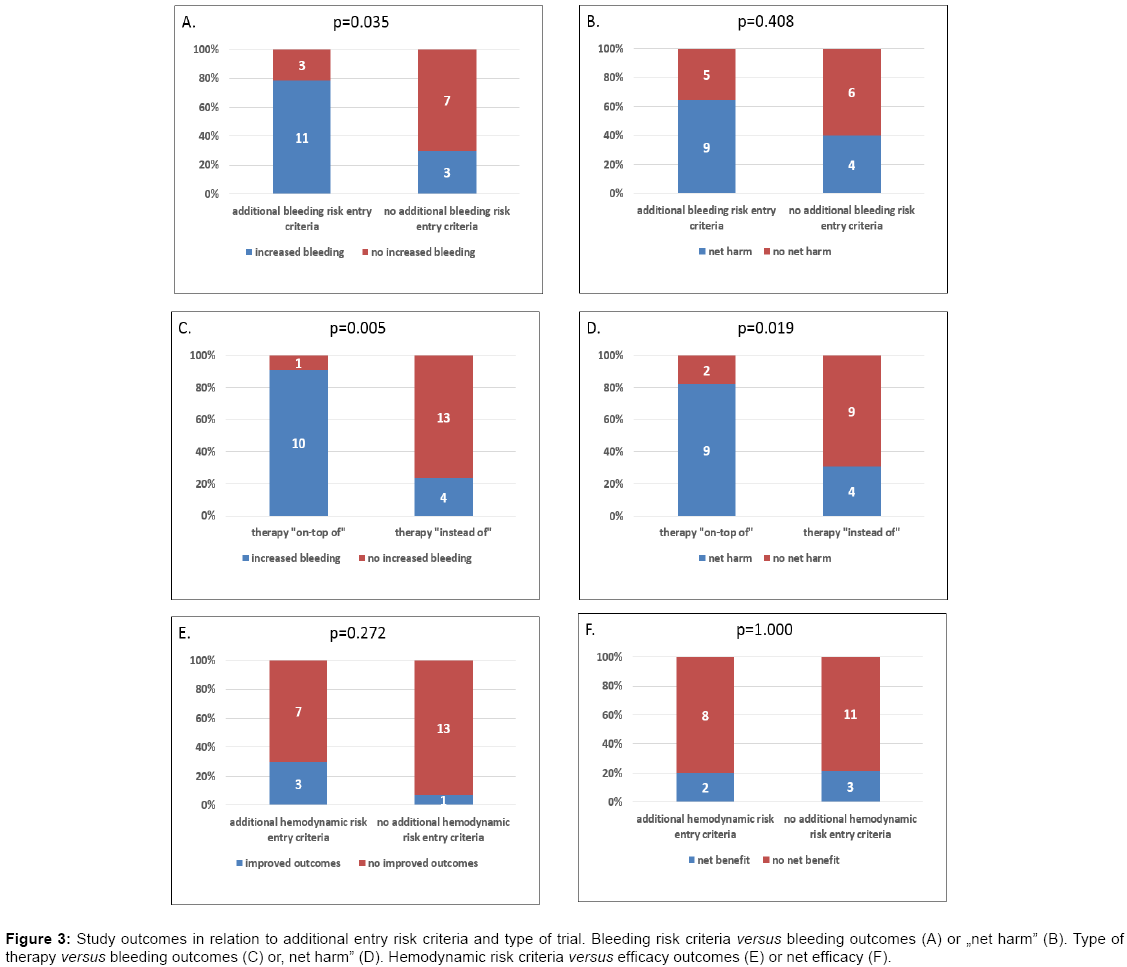
Figure 3: Study outcomes in relation to additional entry risk criteria and type of trial. Bleeding risk criteria versus bleeding outcomes (A) or „net harm” (B). Type of therapy versus bleeding outcomes (C) or, net harm” (D). Hemodynamic risk criteria versus efficacy outcomes (E) or net efficacy (F).
Our findings indicate that the outcomes of antithrombotic trials in ACS may be related to the trial selection criteria. We found that the enrichment strategy based on markers reflecting bleeding hazard in antithrombotic trials in ACS is correlated with more bleeding outcomes. This suggests that manipulating entry criteria may either hide or potentiate the tested drug efficacy and safety characteristics. Consequently, any trial results may be a priori, partially fixed by the use of the selection criteria rather than the actual drug action, which has heavyweight implications.
In December 2012, FDA published draft guidance “Enrichment Strategies for Clinical Trials to Support Approval of Human Strategies for Clinical Trials to Support Approval of Human Drugs and Biological Products“(1). It distinguished two types of trial enrichment: (1) prognostic – i.e. choosing high risk patients, more likely to have the study endpoint, and (2) predictive – i.e. choosing patients more likely to respond to treatment. The distinction is particularly applicable to ACS patients, where the risk markers are not synonymous with the risk factors predicting positive response to treatment. According to our previous analysis, only patients with relatively high hemodynamic hazard are likely to respond positively to more aggressive antithrombotic or invasive therapy (lower right quadrant in Figure 1). We previously showed that patients with high risk, but determined by non-hemodynamic hazard markers, despite trivial infarctions, had high risk of death associated with the highest rate of bleeding [2]. These patients were unlikely to benefit from aggressive reperfusion therapies.
The dominant risk concept in ACS does not adequately account for the distinction between the risk markers and the risk factors, often leading to confusion followed by inappropriate management recommendations. Their example may be the European guidelines recommending urgent invasive management in patients with non ST elevation ACS and GRACE risk score>140 (for example 80-year olds with kidney failure and systolic blood pressure of 130 mmHg, regardless of ECG changes or troponin level), on an equal basis to patients with dynamic changes of ST-T or increased troponins [31]. Our data suggest that this inadequate risk concept contributes also to an inappropriate use of selection criteria for the enrichment of antithrombotic clinical trials in ACS. It may translate into losing control over the study outcomes or their erroneous interpretation. One of the extreme examples is the apixaban phase 3 trial - APPRAISE-2, where eligible patients were supposed to have two or more of 5 bleeding and 4 hemodynamic hazard markers (4). It resulted in a fragile study group without any precedence in real life; with median age of 67 years, 18% of patients with peripheral artery disease, 10% after stroke, 29% with GFR<60ml/min, and 48% with diabetes [27]. Not surprisingly, this phase 3 study, designed primarily for efficacy evaluation, was terminated for safety reasons. Paradoxically, the study group had a higher bleeding risk profile than promising in terms of clinical efficacy phase 2 trial, designed primarily for safety evaluation (APPRAISE-1) [3]. As shown by our results, such an effect was likely to be predetermined by the selection criteria, although contrary to the sponsor intent. On the other hand, selection criteria for a phase 3 study of a competitor agent – rivoraxaban – included barely one (conditional) bleeding hazard marker, and resulted in a beneficial outcome (in subjects under 55 years of age with either diabetes mellitus or a previous myocardial infarction) (ATLAS ACS TIMI 51) [7]. According to our analysis, it may have been the study designs and not the drugs’ properties that contributed to the divergent outcomes between apixaban and rivoraxaban studies. The examples above illustrate the confusion within top scientific and regulatory communities, regarding the enrichment of antithrombotic trials in ACS based on the current risk concept.
The uncontrolled pre-determination of any trial outcomes by inclusion criteria may result in either erroneous acceptation of harmful drugs, or abandoning the use of beneficial ones. In the case of conscious manipulation, it may lead to a fraud. According to the FDA document, any enrichment design should be explicitly described in the protocol and study report and should fully detail the enrichment maneuvers and their impact on interpretation of results (1). However, the lack of details in the document and corresponding confusion prompted big pharmaceutical companies to call on the FDA to supplement its guidelines [32]. Current results seem to support relevance of our multidimensional risk concept distinguishing between ischemic and bleeding hazards [2]. It may aptly complement the FDA recommendations, likely providing the sought for information within the ACS trials area. It allows for a conscious application of varying risk criteria for either prognostic or predictive enrichment of future clinical trials, helping to evaluate the intended aspects of the tested therapy, including the evaluation of “net benefit”. It also provides a basic concept helping to interpret the outcomes of both past and future studies, plan subgroup analyses, and better refer the selection criteria to real life patients. Moreover, it may serve as a platform for developing a multidimensional risk concept supporting management and drug development within other therapeutic areas, including antithrombotics use for emboli prevention in deep vein thrombosis or atrial fibrillation.
The number of the studies available was relatively small, not allowing for robust statistical subgroup or multivariable analyses. On the other hand, despite the small number of studies the differences were significant, underscoring the initial theses. Varying inclusion/exclusion criteria and the definition of outcomes across the studies analyzed did not allow us to perform a formal meta-analysis. Given that the studies reported were large, prospective, multicenter, randomized, sponsored trials, the risk of publication bias or selective reporting is low, though possible.
The results of antithrombotic trials in ACS are related to the trial selection criteria, suggesting that the trial results showing differences in safety and efficacy of the drugs used may be partially related to the trial population rather than differences inherent to the drugs.
Competing interests: the authors have no relevant interests to declare. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.