Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2015) Volume 5, Issue 1
Introduction: Physical activity is recommended to maintain physical health. In addition, it is also thought that exercise affects the brain in different ways that may counteract the effects of mental deficiency, such as encouraging neurogenesis and improving cerebral perfusion and increasing cerebral blood flow.
Background: Physical exercise and fitness have been proposed as potential factors that promote healthy cognitive function.
Objective: Our objective was to evaluate the effects of a training program with standardized exercise on reaction time in male adolescents with mental deficiency.
Method: A total of 51 male adolescents, aged 14 to 16 years were divided into three groups: (1) healthy group (HG: 17 healthy school children without any mental deficiency), (2) a trained group (TG: n=17) that participated in an aerobic programme,consisting of one daily session (~60 min),twice weekly, during a period of three months, and (3) a sedentary group (SG: n=17, that performed no training). HG and TG were participants with mild mental deficiency. The software “REACTION” was used to measure the reaction time in response to visual stimulus at different periods (at rest: one day before exercise, immediately after exercise and one day after exercise). Anthropometric characteristics were determined in the three groups. All measurements were determined before and after the experimental period.
Comparisons were determined for intra and inter-groups.
Results: The results showed significant differences (p<0.001) in reaction time between SG and TG in the different time periods. In addition, the mean of reaction time in TG was similar to that observed in HG.
Conclusions: This research suggests that three months of regular exercise training significantly improved reaction time and consequently the cognitive function in mild mentally deficient adolescents. Physical activity seems to be an indispensable means of improving performance of cognitive activity in adolescents with mild mental deficiency. In addition, these results could be used to justify the relationship between task difficulty and exercise.
Keywords: Cognitive function; Reaction time; Mental deficiency; Adolescents; Physical activity
The positive effects of physical activity on cognition have been extensively recognized [1,2]. Physical exercise is a behavioral intervention known to enhance brain health and plasticity [3]. Esteban- Cornejo et al. [4] showed that there may be a dose response between physical activity intensity and cognitive functioning in older adults. The findings supporting a relationship between moderate- to vigorousintensity physical activity and cognitive functioning are consistent with previous observational and intervention studies.
Clinical and experimental studies from animal models of Alzheimer’s disease have revealed that if initiated early in life, exercise effectively decreases the development of cognitive deficits caused by senescence [5,6]. Several studies have demonstrated that the scores on the Mini Mental State Exam (MMSE) of individuals over 55 years old who had a history of exercising have been compared to those without a history of exercising and showed that performance in cognitive tests can be influenced by age, education level and physical exercise [7]. For that reason, it seems that the practice of physical activity is an indispensable mean of maintaining good physical [8] and mental health [9]. People with intellectual disabilities [10], also known as mild to moderate intellectual disabilities [11], are no exception to this trend. Indeed, physical activity is probably as the field which the greatest number of implementations has been made to ensure that disabled people can practice [12].
Difficulties in the integration of perceptual information into motor action may result in inadequate solutions to daily motor problems. Intellectual disability relates to inability to integrate visual inputs and hand movements [13]. Scientific studies have demonstrated the usefulness and importance of regular, moderate physical activity qualitatively among disabled people [14]. This practice also allows important properties facilitating the autonomy of the disabled on the physiological, psychological and social field [15]. Since the sixties, it was shown that individuals with mental disabilities-cons have no indication of a capacity to exert a physiological physical activity or sport [16].
To date, there is no proven link between fitness and cognitive impairment. However, it was revealed that the low overall fitness of mentally retarded subjects compared to their age [16,17]. This deficit is attributable directly. In fact, the study of Roebroeck et al. [18] showed that specific impairments in executive functioning might be related to everyday physical activity of adolescents and young adults with meningomyelocele. Numerous studies have shown that endurance training, regular and sustained improves muscle strength, cardiovascular and ventilatory in patients with intellectual disabilities [19]. Thus, any program of rehabilitation training based on the individualization of physical preparations, an appropriate intensity, sufficient regularity and appropriate teaching methods improved the physiological capacities of the public. Therefore, it was suggested that the low fitness observed in people with intellectual disabilities compared to non-deficient populations appears to be due to physical inactivity commonly evoked in subjects with intellectual disabilities [17]. It is now well established that the practice of physical activity can improve the coordination of movement and the precision of movement [20]. Furthermore, it allows the acquisition of a higher self-esteem and reinforces the pleasure of making and succeeds [21]. However, the situation of mental disability can cause difficulties in learning and thinking and can cause an increase in reaction time of the affected patient. Indeed, the cognitive performance of disabled and able-bodied people is different [22].
Really, several researchers have shown that a mild mental disability is characterized by an efficiency reduced intellectual functioning, due to a deficit of selective attention (the person does not choose the right information), lack of working memory, less efficiency in a situation of systematic problem solving, lack of cognitive and meta-cognitive strategies [22,23]. Other researchers have revealed that there are some neuro-endocrinological predictors of early cognitive decline in clinical settings [24].
Up to now, there is limited experimental evidence and lack of studies or previous publications having examined the effect of training on the reaction time to support the view that training is a mean for improving the reaction time in adolescents with mild intellectual disabilities. To our knowledge, this is possibly first study examining impact of exercise on cognitive function in a mentally disabled population, whereas impact of exercise on speed of processing has been examined in other populations. Therefore, our objective in this work was to study the effect of training on cognitive development. We choose to compare the reaction time in three groups: a healthy group and two groups of adolescent subjects with mild intellectual disabilities (trained and no groups). We look ahead to prove that reaction time could be higher in trained subjects compared to untrained ones. The objective of this study was to examine if an aerobic programme could affect ability on cognitive tests in Tunisian mental deficient adolescents. In addition, we would like to compare the trained group with others without any mental deficiency. So, we anticipate that reaction time could vary during the day and depends on the activity of the individual; i.e., why we measured the reaction time in different periods (at rest, immediately after exercise and one day after exercise).
Participants
The target population studied consists of 51 male adolescent subjects aged 15 to 17 years, with mild intellectual disabilities. They have all voluntarily participated in this study. All subjects were recruited from the hospital and were divided to a control group (CG), a trained group (TG) and a healthy group (HG). None of the participants had, during the experiment, apart from slight mental retardation, other medical history or significant traumatic. The investigation was conducted in accordance with the Declaration of Helsinki. All participants were informed of the purposes of the study as well as the experimental procedure. Before testing began, participants gave written informed consent after receiving both a verbal and a written explanation of the experimental design and its potential risks. The subjects were told that they were free to withdraw from the trial without penalty at any time. All procedures were approved by the Institutional Review Committee for the ethical use of human subjects, according to current national laws and regulations.
Sample allocation: This sample was divided into three groups:
• The sedentary group (SG), consisting of 17 sedentary subjects consisted of participants with mental disabilities who received no training.
• The trained group (TG) formed with 17 subjects that participated in an aerobic programme, one daily session (~ 60 min) twice weekly during three months.
• The healthy group (HG) formed with 17 subjects without any mental deficiency and received no training.
Study Design
Anthropometric measurements: Anthropometric measurements were performed by the same experimenter, at the beginning of the familiarization session. These measurements concerned the height and the weight. All measures were conducted on the same day and were completed in the standardized order described below.
Height measurement: Stature was measured to the nearest 0.01 m using a wall stadiometer. The subject starts in standing position, arms extended alongside the body, and bare feet together, heels close together, feet pointed slightly away, head and body straight as with eyes in the horizontal plane.
The size is measured using a measuring rod, torsion with a cursor perfectly perpendicular to the vertical rod graduated (graduation 1 mm). During the measurement, the cursor is placed in contact with the top of the crane supporting material to the hair, while checking if the heels are evaluated in contact with the ground.
Body mass measurement: Body mass was measured using an electronic balance with an accuracy of 100g (Precision balance type EKS) and the subjects were lightly clothed, without shoes and feet together. Age and Anthropometric characteristics of both sedentary and trained groups are presented in Table 1.
| Parameters | HG | SG | TG |
|---|---|---|---|
| Age (years) | 15.5 ± 0.66 | 15.21 ± 0.87 | 15.97 ± 0.91 |
| Weight (kg) | 67.70 ± 3.40 | 72.02 ± 4.07 | 64.70 ± 4.00 |
| Height (cm) | 165 ± 1.86 | 166 ± 3.0 | 164 ± 2.83 |
| BMI (kg/m2) | 24.00 ± 2.20 | 26.17 ± 2.36 | 23.89 ± 2.10 |
Table 1: Mean values of age and anthropometric parameters in the three groups: HG, SG and TG.
Aerobic training
All exercise sessions consisted of 10-15 min of warm-up and cooldown stretching and 40-50 min of aerobic exercise. These sessions were carried out two days/week (in TG) in a gymnasium or outdoors; whereas SG and CG were untrained groups. The standardized sessions were supervised by the same physical trainer. Each session lasted 50- 65 min (mean duration of exercise sessions 55 minutes. The intensity and duration of the exercise program were progressively increased throughout the 3-months periods, according to the tolerance of each individual patient.
Before the experiment period, the participants of CG and SG groups were informed that they would need to wait on premises during exercise training for TG group.
Measurement of the reaction time
The software “REACTION” was used to measure the time of reaction using values (the value considered here is the mean and the evolution of the deviation from the different reaction time).
This software includes various tests: comparisons of forms, appearances of forms, a form of recognition among others. The user could choose the color of various geometric figures or even choose static images (flowers, books ...). In this experiment the test was chosen as the recognition of a “blue square” among other figures (circles, triangles, square, and rectangle) of the same color. Each patient was asked to click on assessed as quickly as possible when he saw that form. Throughout the experimental period the individual should keep the same test with the same color and same shape (Figure 1). The appearance of the form takes 400 milliseconds as inter-stimulus interval. On the test day, all subjects were asked not to drink coffee, tea, cola and other drinks considered to have stimulant effects (Ruijter et al. 2000). In addition, we asked all subjects to sleep at night at the same time (21 h). All subjects evaluated in this study have never used the software before. The reaction times were measured after the entire exercise intervention was completed (before and after three months) in three different periods (one day before exercise, immediately after exercise and one day after exercise). Testing sessions were conducted at the same time of the day (at 12H 30 min), and under the same experimental conditions. Therefore a meeting of the recognition software was conducted during which each subject performed a familiarization trial in the two days prior to the main testing. All individuals were subjected to the test under the same conditions and have completed three trials during the test. Each trial consisted of ten times of reaction. Testing sessions were conducted at the same time of the day, and under the same experimental conditions, at least 3 days after the most recent competition. All participants were tested using identical protocols and the tests were completed in a fixed order. Statistical analyzes included the number of errors and omissions in calculating the reaction time (Figure 1).
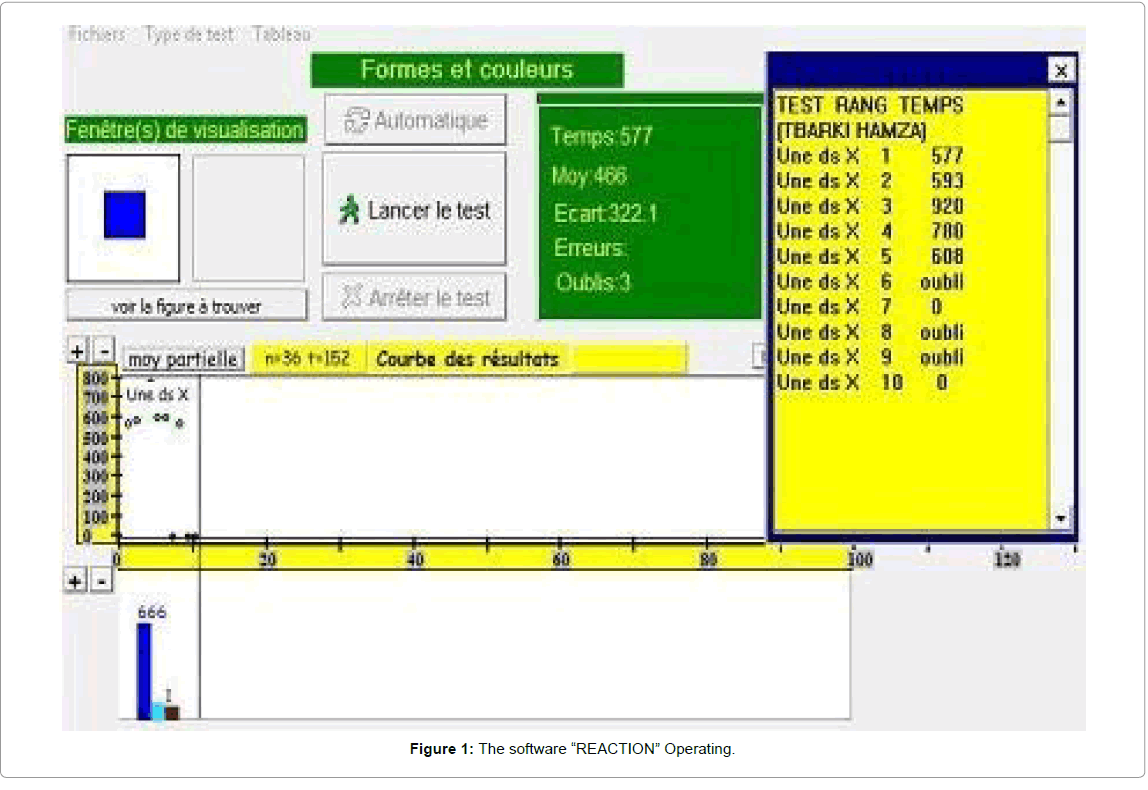
Figure 1: The software “REACTION” Operating.
Statistical analysis
The sample size for the trial was determined by the most demanding hypothesis to detect effects aerobic capacity on treatment. Statistical analyzes included the number of errors and omissions in calculating the reaction rate. Statistical analysis was performed using SPSS (version 17.0 for Windows, SPSS, Chicago, IL, USA). Overall adjustment responses were analyzed using a one-way repeated measures analysis of variance. Descriptive statistics are presented as means; standard deviation and range (mean ± standard deviation, range). The Intraclass correlation coefficients (ICC) for test outcomes ranged from 0.88 to 0.96 [25]. Statistical significance was set at 0.05.
Anthropometric measurements
Comparison of anthropometric parameters shows that the distribution of age in the three groups is very homogeneous (aged between 15.21 and 17.02 years) with a small variation in the size, weight and BMI, but without significant difference in all the parameters (Table 1).
Because not only intra-group comparisons are important but also multiple inter-group ones, for the reaction time, we made inter-group and intra-group comparisons for the three assessment periods (in the three groups).
Intra-group comparisons
The reaction time: The intra-group comparison of reaction time as measured at the three assessment periods in the three groups, presented in Table 2, showed that there was significant difference between the three assessment periods for each of the same group. The results showed that the reaction time was significantly increased in when it was measured just after training (Table 2).
| At rest (one day before training) |
One day after training | just after training | |
|---|---|---|---|
| Healthy group | 41658 ± 95.0 | 425.35 ± 118.8 | 666.22 ± 127.6a |
| Sedentary group | 906.37 ± 129.3 | 883.33 ± 147.4 | 985.33 ± 131.5a |
| Trained group | 549.56 ± 101.5 | 559.49 ± 104.2 | 673.56 ± 108.7a |
a: significantly different (P < 0.001) to the means observed both at rest (one day before training) and one day after training
Table 2: The Reaction time measured (expressed in msec) in healthy (HG), sedentary (SG), and trained (TG) groups, before the experiment period, at different selected periods: at rest (one day before training), immediately after training and 1 day after training.
The number of errors: Although, the mean values were increased in all the groups just after training, Table 3 showed no significant difference in the reaction time for all the groups.
| At rest (one day before training) |
One day after training | just after training | |
|---|---|---|---|
| Healthy Group | 0.85 ± 0.35 | 0.78 ± 0.25 | 1.0 ± 0.40 |
| Sedentary Group | 1.20 ± 0.68 | 0.82 ± 0.50 | 1.11 ± 0.80 |
| Trained Group | 1.23 ± 0.90 | 0.65 ± 0.20 | 1.05 ± 0.30 |
Table 3: The number of errors, for the reaction time, measured in healthy (HG), sedentary (SG), and trained (TG) groups, at different selected periods: at rest (one day before training), immediately after training and one day after training.
In addition our results (Table 4) showed that the mean of reaction time obtained in TG after the experimental period was significantly lower (P<0.01) comparatively to that observed before experimental period. However, no significant difference was observed in HG and SG before and after the experimental period.
| At rest (one day before training) |
One day aftertraining | just after training | |
|---|---|---|---|
| Healthy group Before experimental period After experimental period |
416.58 ± 95.0 423.64 ± 88.5 |
425.35 ± 118.8 415.36 ± 90.4 |
466.22 ± 127.6 424.6 ± 100.5 |
| Sedentary group Before experimental period After experimental period |
906.37 ± 129.3 914,87 ± 110,40 |
883.33 ± 147.4 875,33 ± 151,60 |
985.33 ± 131.5 879,33 ± 115,28 |
| Trained group Before experimental period After experimental period |
549.56 ± 101.5 482,22 ± 78,74ab |
559.49 ± 104.2 497,34 ± 75,20ab |
673.56 ± 108.7a 603,90 ± 93,45ab |
a: significantly different (P<0.01) comparatively to the means observed before experimental period
b: significantly different (P<0.01) comparatively to the means observed both in SG and HG groups
Table 4: The Reaction time measured (expressed in msec) in healthy (HG), sedentary (SG), and trained (TG) groups after the experiment period at different selected periods: at rest (one day before training), immediately after training and 1 day after training.
Inter-group comparisons
The reaction time: The results of the inter-group comparison for the reaction time as measured in the three assessment periods are presented in Figure 2. Though both healthy and trained groups showed significant and a higher reduction in the reaction time when compared to the SG, the inter-group comparison between healthy and trained group showed comparable data with a small reduction which was no statistically significant in the HG compared to the TG. On the other hand, these data demonstrated that the performance obtained in TG after the experimental period was significantly better (P<0.01) than that of SG but still lower than that of HG (Table 4).
The results of the reaction time, one day before training (Figure 2), showed a significant difference (p<0.001) in the SG (906.37 ± 129.3 msec) comparatively to TG (549.56 ± 101.5 msec) and HG (516.58 ± 95.0). This difference is in favor of the TG (having the best performance).
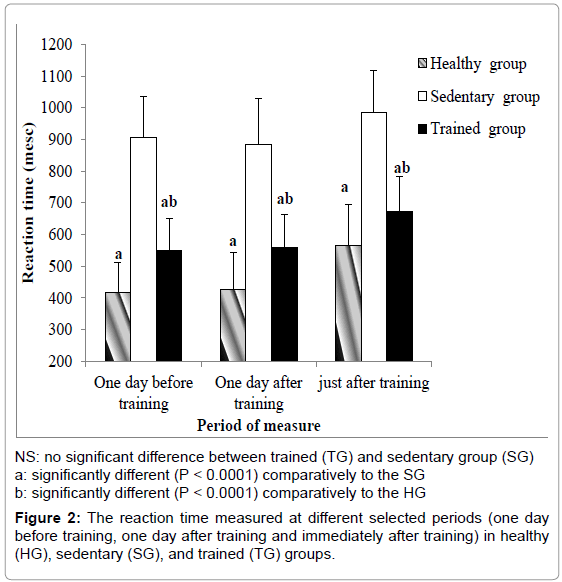
Figure 2: reaction time measured at different selected periods (one day before training, one day after training and immediately after training) in healthy (HG), sedentary (SG), and trained (TG) groups.
Just after training, the comparison of the reaction time between the TG (673.56 ± 108.7 msec) and the SG (985.33 ± 131.5 msec) (Figure 2) showed a significant difference for the trained group (p <0.001). Nevertheless, although the error rate is higher among the sedentary compared to trained subjects, the difference remained no significant (Figure 3)./p>
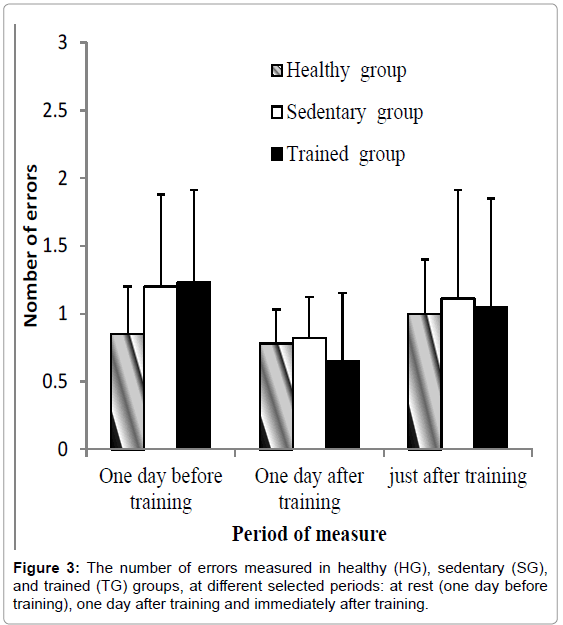
Figure 3: The number of errors measured in healthy (HG), sedentary (SG), and trained (TG) groups, at different selected periods: at rest (one day before training), one day after training and immediately after training.
In addition, the standard deviation is lower in the HG comparatively to the other groups but without significant difference between the three groups about the number of errors
The mean values of the reaction time, one day after practice showed a difference in favor of the TG trained group compared to the SG (p<0.001).
Our study illustrates improvements of reaction time in the trained group. By comparing the results of both HG and TG at the same time points, the performance obtained as well as one day before training or after one day of training remain significantly higher (p<0.0001) than that observed in the SG. However, mean values obtained in the TG are comparable to those of HG but still significantly higher (p<0.001). This explains that the performance in HG still better than that observed in TG, despite the improvement of the reaction time performance of TG. The results were consistent with their approach for distinguishing automaticity from the reaction time. When the reaction time is reduced, the performance will be improved and the ability to execute efficiently increase. Indeed, an increased performance in reaction time reflects a higher level of automaticity. It seems that aerobic exercise also helps keep the remaining nerve cells functioning.
If we start with the analysis of the anthropometric measurements, we notice that sedentary subjects have a relatively high mean BMI (26.17 ± 5.58 kg/m²) and are considered, according to WHO standard, as overweight (BMI>25) [26,27]. However, subjects in the TG or HG are characterized by an average BMI that is in the range recommended by WHO (23.89 ± 4.4 kg/m² and 24.00 ± 2.20 kg/m² respectively) allowing these subjects to have a normal build [26].
First of all, we made an intra-group comparison of the reaction time. The purpose of this comparison, particularly in the TG, was to examine whether the level of alertness (assessed by measuring the time reaction) may vary depending on the psychological state of the individual. We illustrate among the group of sedentary subjects, the intra-group comparison of reaction times measured at different times over the training period (one day before training, immediately after training and one day after training) showing no significant difference between time points. The same results were found for subjects in trained and healthy groups. This effect confirms the absence of external factors which could influence the results. Then for inter-group comparison, we can perceive that the values of the reaction time found in both groups (SG and TG) were higher compared to that in a healthy person (HG). These results are consistent with those in the literature [which could influence the results. Then for inter-group comparison, we can perceive that the values of the reaction time found in both groups (SG and TG) were higher compared to that in a healthy person (HG). These results are consistent with those in the literature [28]. So as valid for the reaction time of movement, an improvement has been also found in mild mental deficiency [29,30].]. So as valid for the reaction time of movement, an improvement has been also found in mild mental deficiency [29,30].
Furthermore, these results showed that the contribution of the practice of physical activity is not limited to improving the physical fitness but can also be observed on several fronts including on the psychic plane and engine. Lautenschlager et al. [31] reported that physical activity had positive effect in preserving cognitive function in older adults at risk for Alzheimer disease. In an experimental study, Clark et al. [32] had obtained a cognitive gain in a functional analysis of neurovascular adaptations to exercise in the dentate gyrus of young adult mice. In addition, Baker et al. [33] had shown a progress of cognitive capacities after an aerobic exercise on mild cognitive impairment in a controlled trial.
As mentioned by Chodzko-Zajko [34], there are very few studies that directly examined the relationship between task difficulty and exercise. Our results are in accordance with those found by Hawkins et al. [35] who used two visual attention tests that each had two levels of difficulty: one was a single task, the other a dual task. They found that after the assessment periods there were no differences between the exercise and no-exercise groups on the simpler task, but that timesharing costs on the dual task were more reduced for the exercise than the no-exercise group. Evidence thus suggests that task complexity may indeed partly determine whether an effect of exercise is seen or not, although it is inconclusive which type of task (simple or complex) actually shows greatest benefit.
For the neuromuscular interpretation, Krebs [36] had noted an improvement in gross motor skills through practice without physical modification of fine motor skills (precision gesture like writing). Therefore, cognitive impairment does not seem directly involved in motor skills of a subject. An individual may decide to present a low intelligence in the narrow sense of intelligence quotient (ability to symbolize, to manipulate and control concepts of abstraction) and a high psychomotor intelligence. These observations were confirmed by Ninot and Maino [15] who think that the sport for the disabled is an implementation project, enabling them to spend a motivation to practice and learn. It also gives them the motivation to carry it out and gives meaning to their action. Dejean [37] suggested that sport provides opportunities for athletes with physical or mental disabilities (people with intellectual disabilities and/or mentally ill) to practice a regular motor activity that contributes to improving their fitness, improves performance through a planned training. This increases their efficiency in all areas of daily life and experiences to facilitate their integration or inclusion. Our data are consistent with several authors [38] who have focused on the reaction time and demonstrated that the speed of simple reaction can be improved by 10-15%.
In our study, the result comparisons of the reaction time between the three groups also showed a significant difference immediately after training (p<0.0001). This effect explains why even the feeling of fatigue after training has not reverse the performance of the reaction time for the SG and the difference remains permanently in favor of the TG and HG (p<0.0001). These data showing a development of response speed in the TG compared to the SG in all measurement conditions may be due to several factors related to training [15]. The reaction time depends essentially on neuromuscular parameters (capturing information through receptors, its transport to the central nervous system by afferent neuron and selecting an answer and then sending the response in the efferent pathways to be physical response is more or less influenced by various factors including limiting factors that affect:
• The volume of muscle fiber: The physical training can change the diameter of the fibers or their ability to coordinate, but not the percentage of their distribution.
• The type of muscle: The speed of contraction of a muscle depends to a large extent, on the type of fibers that compose it. A high percentage of fast fibers are correlated with a high speed gestures.
Regarding the increase of reaction time observed in all the groups immediately after training (Figure 2), it seems to be related to the fatigue of neuromuscular parameters (capturing information through receptors, speed transmission of nerve impulses to or from the central nervous system and selecting an answer by the same structure) [15].
These findings are in accord with the results obtained by Dustman et al. [39] who found that aged subjects were able to improve their performances on a wide variety of neuropsychological tasks. But, results of physical training are more ambiguous. Our results are in contrast with those of Madden et al. [40] that examined the effect of 4 months of an aerobic programme on cognitive performance in aged adults. However, despite a significant increase in the aerobic capacity, no effect of the aerobic training was noted for any of the cognitive tasks examined in the study.
We must mention here that there are possible explanations for the differences observed between the groups which might be caused by differences in settings, the degrees of infirmity and the length of their life. These and other possible factors have to be avoided. In fact, several factors influence the development of a child’s social relationships and skills [41]. These physical and mental activities act as a central cause in their development. Furthermore, it might control long-term mental and physical health [42]. Law et al. [43] recognized some child factors that influence participation. They concluded that higher levels of physical exercise were related with augmented intensity of participation. Thus, it may possibly be anticipated that participation in an exercise programme can go ahead to the maintenance of the cognitive functions and mental health. Verschuren et al. [44] affirmed having a higher physical function that steer to a greater intensity of participation. This could explain the results of Faulkner et al. [45] who advance the knowledge concerning the timing, importance and viability of exercise as a secondary prevention strategy for improving health outcomes for stroke and Transient ischemic attack (TIA) patients.
The entourage of adolescents in the trained group and the medical staff declared obviously detecting improvements for the motor, executive, autonomy, and cognition functions. In the other side, sedentary group is at risk of a sedentary lifestyle that will irremediably influencing its reactivity [46] and consequently their mental health and cognitive skills. We can explain this by the decrease of the neuroplasticity in absence of stimulus and mental or physical activities. Such situation leads to the synaptogenesis and the synapse malleability. To avoid such adverse effects, it seems necessary for adolescent with mental deficiency to preserve a physical exercise program long-lived. Supervised training programs at hospitals or schools offer opportunities to a better wellbeing for mental deficient subjects. We have to study these possibilities in upcoming research.
This research suggests that standardized functionally based exercise program significantly improved reaction time. At this time, it seems that the best prescription for a better therapeutic on mild mental deficiency would be constant physical and mental activities. Moderate regular exercise ought to be considered as an indispensable mean of adjuvant treatment of mental illness and deficiency and improving mental wellbeing in a critical period of life such adolescence. We should, nowadays, elucidate which type of activity might be most practical.
Additional Contributions
We appreciatively recognize all children, their parents for participation. We express gratitude to the physicians and doctors in for their help and all research assistants for their assistance and support.