Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Case Report - (2013) Volume 3, Issue 4
We report a patient with Coronary Heart Disease (CHD), hypertension and type 2 Diabetes Mellitus (DM) who volunteered to stop all conventional medications and use honey as an alternative therapy for almost 11 years. In spite of persistent hyperglycemia and dyslipidemia, unexpectedly his blood pressure was controlled, his CHD improved or at least stabilized, and he did not develop cerebral strokes. Moreover and unexpectedly he did not develop diabetic ketoacidosis or hyper-osmolar coma. However he developed micro-vascular complications in the form of peripheral neuritis and non proliferative retinopathy after 6 and 8 years, respectively. Although a final conclusion could not be drawn from a single case, this case study highlighted important questions and observations that warrant well designed randomized controlled studies to evaluate whether intake of honey, as a complementary agent, concomitantly with anti-diabetic treatment has the potential to prevent or reduce both macro-and micro-vascular complications of diabetes
Keywords: Honey; Diabetes; Coronary heart disease; Dyslipidemia; Hypertension; Neuropathy; Retinopathy; Micro-albuminuria
In spite of recent advances in the management of Diabetes Mellitus (DM) the mortality from macro-vascular complications, particularly Coronary Heart Disease (CHD) is still high. For many decades researchers have been trying to solve the puzzles surrounding the pathogenesis of diabetes and its complications, aiming at achieving the main goal; prevention or remission of diabetes; or at least prevention of its complications. These complications are responsible not only for significant morbidity and mortality but also for a large economic burden. For this; several treatment strategies, including drugs, have been used in DM to control hyperglycemia and other associated metabolic derangements; and to treat complications particularly CHD. However control of hyperglycemia and dyslipidemia, at least in some patients, has failed to prevent or reduce these complications.
Honey is a natural substance produced by honey bees. It has many benefits for nutrition and health [1]. Recently, the potential beneficial effects of honey in DM and its potential mechanisms of action were reviewed [2]. Furthermore there is no reported toxicity to honey intake except for the recommendation of not giving honey to infants below the age of one year, which is controversial because of the possible rare existence of clostridium botulinum spores in honey.
In this report we present a case with type 2 DM, hypertension and Coronary Heart Disease (CHD), who volunteered to stop all conventional medicines and use honey, as an alternative medicine for treatment of his diseases. The data presented in this report were from October, 2002 to April, 2013.
Patient
The case is an Egyptian non smoker man born to non consanguineous parents on 1956. He is the 3rd of five siblings; all are males. All his brothers presented with hypertension, dyslipidemia and Coronary Heart Disease (CHD) after the age of forty. The father also had CHD and died at the age of 63 because of acute myocardial infarction. The elder brother also died, in the late fiftieth, of sudden cardiac arrest a few months after Coronary Artery Bypass Grafting (CABG). The 4th brother is now arranging for CABG. The father, the 1st, 3rd and 4th siblings developed DM a few years after their cardiovascular disease.
On 1997 he was admitted to intensive care unit with severe acute chest pain which was found to be due to acute myocardial ischemia. He was hospitalized for one week and discharged on medications. On July 1999, when he was 43 years old, implantation of stents for both right coronary and circumflex arteries was done. On June 2002, while he was prepared for an operation for drainage of a perianal abscess, diabetes was accidentally discovered. Between 1997 and 2002 while he was compliant to his medications (isosorbide dinitrate, diltiazem hydrochloride, hydrochlorothiazide, acetyl salicylate, statin, glimepiride and vitamins B1, B6, and B12) he suffered frequent attacks of angina as well as transient ischemic attacks. His usual daily physical activities were markedly limited because of dyspnea and chest pain, Also he suffered frequent Upper Respiratory Tract Infections (URTI); nearly 6 times per year, each lasted at least 3 weeks. The patient did not receive anti-pneumococcal or anti-influenza vaccine.
On the first of October 2002 he volunteered to stop all medications and use honey as an alternative treatment; and he provided a written consent (Figure 1). The patient was clearly informed about the risk events that might occur if he stopped his medicines and use honey, with its well-known high sugar content, as an alternative therapy. His religious belief that honey is a healing agent and the fact that his father and elder brother died of CHD in spite of being compliant to their medicines were among the factors which made him to try this risky trial. Based on the observations that honey might improve glycemia [3] and might have cardio protective effects through its anti-oxidant properties [4,5], it was initially planned to provide oral honey in large doses in order to produce fast effects expected to be worrisome or beneficial. In case of the former the study will be terminated.
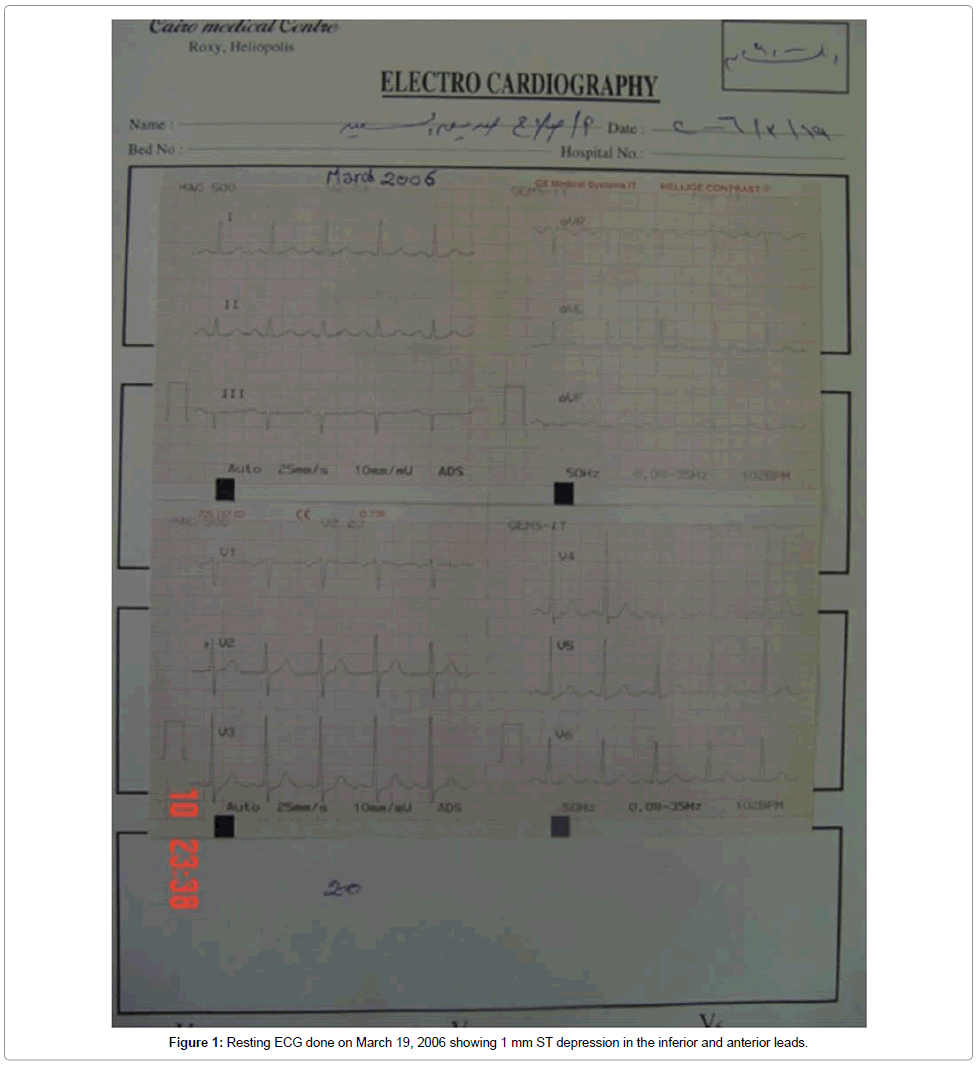
Figure 1: Resting ECG done on March 19, 2006 showing 1 mm ST depression in the inferior and anterior leads.
Honey
The honey used in this study was an Egyptian clover honey of a carbohydrate content of 78.4 g/100 g, pH of 3.7 and a moisture content of 18.8%. The fructose and glucose content of the honey were 37.8 and 30.2 g%, respectively. Starting from October 3, 2002 the patient stopped all medicines and consumed honey in an empirical dose of 2 gm/kg/ day assuming body weight 75 kg i.e., 150 gm (125 ml) honey daily. The daily dose was divided as 50 ml (60 gm) honey dissolved in water and given before meals twice daily. The remaining 25 ml (30 gm) were used for sweetening purposes. Dissolving honey in water enhances the anti-microbial properties of honey [6], facilitates swallowing and helps adjusting the dose. As each gm of honey yields 3 kcal, this daily dose of honey provided 450 kcal. This amount of calories was not subtracted from his meals as there was no specific diet restriction except for food preservatives and additives, beverages and sweets. He was asked to use honey as the only sweetening agent. Because of its anti-microbial properties [6], it was planned, in case the study was not terminated, to double or triple the daily dose of honey during any infection particularly respiratory tract infections.
Base line characteristics
At base line the patient’s general condition was fair, his Body Mass Index (BMI) was 27.8, his resting pulse was 82/min and regular, and his B/P was 160/110. There was no evidence of heart failure. His chest, heart and abdomen were clinically free. There was no edema of lower limbs and the peripheral pulsations were palpable. Also there was no evidence of peripheral neuritis and fundus examination was normal. The only abnormality in urinalysis was glucosuria. The findings on chest X-Ray were unremarkable. Doppler echocardiography showed Segmental Wall Motion Abnormalities (SWMA) and left ventricular diastolic dysfunction (Table 1).
| Characteristic | |
|---|---|
| Body weight (BW) (kg) | 86 |
| Height (Ht) (cm) | 176 |
| BMI | 27.8 |
| Blood pressure (mmHg) SBP DBP |
160 110 |
| Random blood sugar (RBS) (mg/dl) FBG (mg/dl) 2hr PBG (mg/dl) |
325 178 351 |
| Hb A1c % | 11.68 |
| Serum creatinine (mg/dl) | 1.22 |
| Blood urea (mg/dl) | 32 |
| Serum triglycerides (TG) (mg/dl) | 189 |
| Serum cholesterol (TC) (mg/dl) | 270 |
| High density lipoprotein (HDL) (mg/dl) | 46 |
| Low density lipoprotein (LDL) (mg/dl) | 186.2 |
| VLDL (mg/dl) | 37.8 |
| Serum uric acid (mg/dl) | 4.06 |
| Alanine aminotranseferase (ALT) (U/L) | 52 |
| Aspartate aminotranseferase (AST) (U/L) | 21 |
| Hb (g/L) | 13.1 |
| TLC (/cmm) | 5800 |
| Platelets (/cmm) | 226 × 103 |
Table 1: Baseline characteristics of the patient before starting honey therapy.
Changes during study
During the first 3 weeks of the study, while the patient was monitored on daily basis, the general condition remained stable and his blood pressure and blood glucose levels remained nearly within the same range as before starting honey. However, after the third week he developed polyuria and polydipsia and he started to lose weight. The blood glucose level rose, and frequently exceeded levels of 500 mg/dL. Unexpectedly these high levels of blood glucose were not associated with dehydration, ketoacidosis or even ketones or albumin in urine. At this stage it was decided to stop the trial, but because the patient’s exercise tolerance improved, he asked to continue the trial in spite of persistent hyperglycemia and in spite of being informed that complications related to hyperglycemia, particularly the acute complications might develop at any time. Since discovery of his CHD, the patient has been afraid from sudden death at any time. He was not convinced that conventional medicines will save his life because his father and some of his relatives and friends died of CHD in spite of being compliant to their medications and in spite of fair control of blood sugar. Throughout the period of the study the levels of Random Blood Glucose (RBG) ranged from 175-667 mg/dL [mean ± SD=386.78 ± 75.44 mg/dL]. Levels above 600 mg/dL were recorded during the first few months of the study. The patient was also able to fast Ramadan months without developing dehydration. Fasting during Muslim month of Ramadan involves abstinence from food and water for twelve hours or more during the day from dawn to dusk (Table 2).
| Characteristic | Year | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 02/03 | 03/04 | 04/05 | 05/06 | 06/07 | 07/08 | 08/09 | 09/010 | 010/011 | 011/012 | 012/013 | |
| BW (kg) [range] | 83.8 ± 1.7 [81- 86] |
80.1 ± 1.5 [78-81.5] |
77.5 ± 2.3 [75-79.5] |
78.1 ± 0.7 [77-79] |
77.3 ± 0.7 [76.5-78] |
78.5 ± 0.5 [78-79] |
79.1 ± 1.4 [77-80] |
79.5 ± 1.3 [78.5-81] |
78.8 ± 0.3 [78.5-79] |
78.8 ± 0.9 [78-80] |
79 ± 0.4 [78.5-79] |
| Resting pulse (beats/min) [range] | 83.9 ± 4.8 [70-90] |
81 ± 3.9 [75-86] |
82.2 ± 2.4 [78-86] |
81.3 ± 2.4 [78-86] |
79.6 ± 2.6 [76-84] |
80.5 ± 3.3 [75-86] |
82.3 ± 3.5 [78-88] |
84 ± 2.1 [80-88] |
84.3 ± 6.6 [80-103] |
82.9 ± 3.2 [80-89] |
84.5 ± 3.4 [80-90] |
| SBP (mmHg) [range] |
130.4 ± 31.1 [100-220] |
116.8 ± 5.8 [105-123] |
124.1 ± 13.2 [110-160] |
125.7 ± 18.3 [110-165] |
120.4 ± 6.2 [110-130] |
112.5 ± 7.2 [110-120] |
117.1 ± 4.6 [110-125] |
114.6 ± 5 [105-120] |
113.1 ± 11.1 [90-135] |
124.6 ± 16.4 [105-160] |
124.2 ± 9.2 [115-140] |
| DBP (mmHg) [range] |
82.3 ± 13.6 [70-110] |
75.8 ± 5.2 [65-80] |
79.5 ± 5.8 [70-90] |
79.9 ± 7.8 [65-95] |
75.7 ± 3.7 [70-80] |
74.6 ± 4 [70-80] |
76.1 ± 4.2 [70-80] |
72.5 ± 5 [65-80] |
73.5 ± 6.6 [60-83] |
78.3 ± 8.4 [65-95] |
78.3 ± 4.1 [70-80] |
| RBG(mg/dL) [range] |
438.9 ± 88 [221- 667] |
399.3 ± 49.8 [333- 483] |
335.5 ± 17.1 [315-364] |
346.1 ± 45.2 [267- 414] |
338.3 ± 11.5 [322-356] |
339.5 ± 7.1 [330-355] |
363.6 ± 38.5 [325-415] |
361.6 ± 55.1 [175-530] |
349 ± 20.1 [320-376] |
331.5 ± 30.2 [288-410] |
330 ± 52.9 [290-390] |
| FBG(mg/dL) | 226 | 278 | 255 | 205 | 315 | ND | 190 | 220 | 232 | 256 | 210 |
| PBG(mg/dL) | ND | ND | ND | ND | ND | ND | 297 | 320 | 357 | ND | 323 |
| HbA1c (%) | ND | ND | ND | ND | ND | ND | ND | ND | ND | 11.8 | 12.2 |
| TG (mg/dL) | 683 | 410 | 483 | 648 | 549 | 470 | 379 | ND | 454 | 393 | 311 |
| TC (mg/dL) | 264 | 256 | 251 | 279 | 248 | 272 | 237 | ND | 248 | 242 | 259 |
| HDL (mg/dL) | 39 | 49 | 48 | 46 | 44 | 41 | 35 | ND | 36 | 36 | 34 |
| LDL (mg/dL) | 124 | 135 | 130 | 104 | 120 | 149 | 126.2 | ND | 145 | 127.4 | 162.8 |
| VLDL (mg/dL) | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | 62.2 |
| Apo A-1 (mg/dL) (N=104-202) |
ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | 140 |
| Apo B (mg/dL) (N=66-133) | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | 150 |
| Blood urea (mg/dL) | 31 | 27 | ND | 24 | 39 | ND | 24 | 37 | ND | ND | ND |
| BUN | ND | ND | ND | ND | ND | ND | ND | 14 | 16 | 19.6 | 11.3 |
| Serum creatinine (mg/dL) | 0.86 | 0.93 | ND | 1.0 | 0.96 | ND | 0.88 | 1.17 | 1.01 | 1.12 | 0.98 |
| Serum uric acid (mg/dL) | ND | 7.1 | ND | 5.7 | ND | ND | ND | ND | 6.8 | 7.3 | 7.5 |
| ALT (U/L) | ND | 25 | ND | 26 | 22 | ND | 25 | 28 | 22 | 22 | ND |
| AST(U/L) | ND | 19 | ND | 16 | ND | ND | ND | 33 | ND | ND | ND |
| CK(U/L) | ND | ND | ND | 51 | ND | ND | ND | 96 | ND | ND | ND |
| LDH(U/L) | ND | ND | ND | 176 | ND | ND | 228 | ND | ND | ND | ND |
| Urine albumin/ creatinine (mg/g) | ND | ND | ND | ND | 19.03 | ND | ND | ND | 29.3 | 33.34 | 43.22 |
| Hb (g/L) | ND | ND | ND | ND | ND | ND | ND | ND | 12.8 | 12.9 | 12.4 |
| TLC (/cmm) | ND | ND | ND | ND | ND | ND | ND | ND | 6600 | 7200 | 5200 |
| Platelets (/cmm) | ND | ND | ND | ND | ND | ND | ND | ND | 186×103 | 175×103 | 149×103 |
| CRP (N < 8 mg/dL) | ND | ND | ND | ND | ND | ND | ND | ND | ND | 5 | 3 |
Table 2: Values and mean values of the patient’s characteristics during the period of the study.
By the second year of the study the severity of polyuria and thirst decreased and thereafter the severity fluctuated, being increased during periods of stress. When there was polyuria the patient was drinking large amounts of water and he was instructed not to reduce water intake being misled by increased frequency of urination. Daily urine output and water intake were not monitored throughout the period of the study.
The rate of weight loss was relatively higher during the first 2 years of the study, where the patient lost about 13% of his weight. Thereafter the body weight fluctuated between 78 to 80 kg (BMI=24-26).
The serum lipid profile including Low-Density Lipoprotein (LDL) cholesterol, High-Density Lipoprotein (HDL) cholesterol, triglycerides and total cholesterol remained abnormal throughout the study. However measurements of apolipoprotein (apo) A-1 and apo B done only once during 2013 found normal apo A-1 level.
Associated with previous changes, the blood pressure started to normalize about 6 months after start of intervention and it remained almost within the normal levels until now. The mean (± SD) systolic and diastolic blood pressures after the first 6 months of study were 119.20 (± 11.75) and 76.39 (± 6.12), compared to 149.88(± 34.31) and 91.5 (± 13.48) mmHg during the first 6 months of study, respectively. However transient elevation of blood pressure (~ 160/90) was recorded once in 2005, twice in 2006 and once in 2012. Each of these episodes of hypertension remained for about 2 to 3 days and resolved without -hypertensive medications.
Throughout the study period the patient was doing his daily activities in a nearly normal way. He is living in the eighth floor of a building of eight roles. He stated that when there was a problem in the elevator, a situation that happened several times, he was able to ascend to the eighth floor without non-stop and without experiencing chest pain. However he experienced three attacks of acute chest pain in 2004, 2006 and 2010. In 2004 he was hospitalized for 12 hours and discharged on medications. His B/P was 115/75 and his pulse was 78/min and regular. His cardiac enzymes and resting ECG were normal. He did not receive the prescribed medications but continued consuming honey. On 2006, he was hospitalized for 3 days during which he received medications including insulin. The resting ECG showed 1 mm ST segment depression in the inferior and anterior leads (Figure 1). Because there was doubt about diagnosis, ECG with exercise was done next day but the test was ended after 8 minutes because the patient reported tiredness but not chest pain, and the tracing showed 1 mm ST segment depression in the inferior and anterior leads (Figure 2). However the blood pressure response during the test was normal. The findings on Doppler echocardiography were nearly normal except for diastolic dysfunction. However there were no SWMA and the ejection fraction was 65% (Figures 3 and 4). After discharge he stopped receiving his medicines and continued taking honey. On 2010 he was not hospitalized. His cardiac enzymes including treponin I, done more than 12 hr after the acute episode, were normal. His resting ECG was also normal (Figure 5).
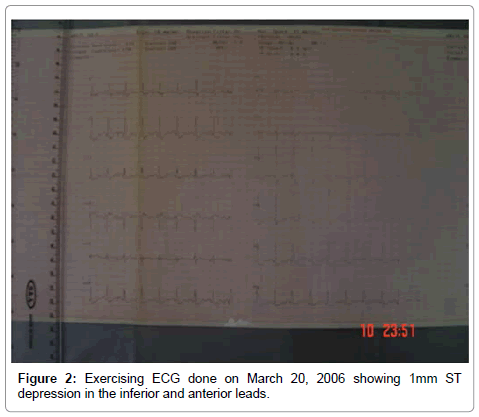
Figure 2: Exercising ECG done on March 20, 2006 showing 1mm ST depression in the inferior and anterior leads.
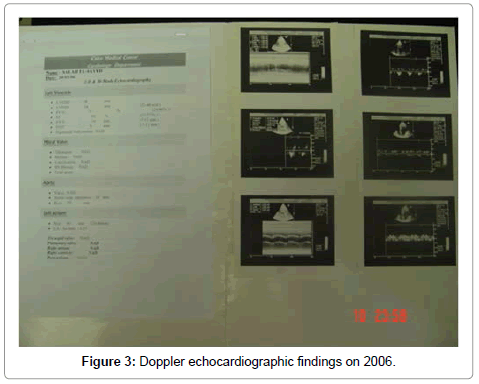
Figure 3: Doppler echocardiographic findings on 2006.
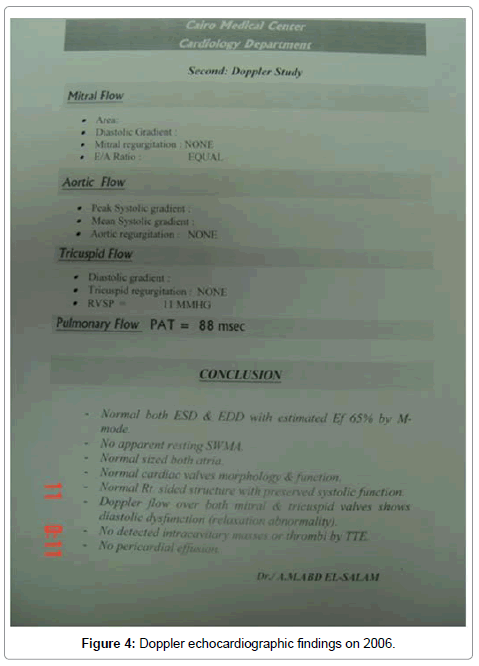
Figure 4: Doppler echocardiographic findings on 2006.
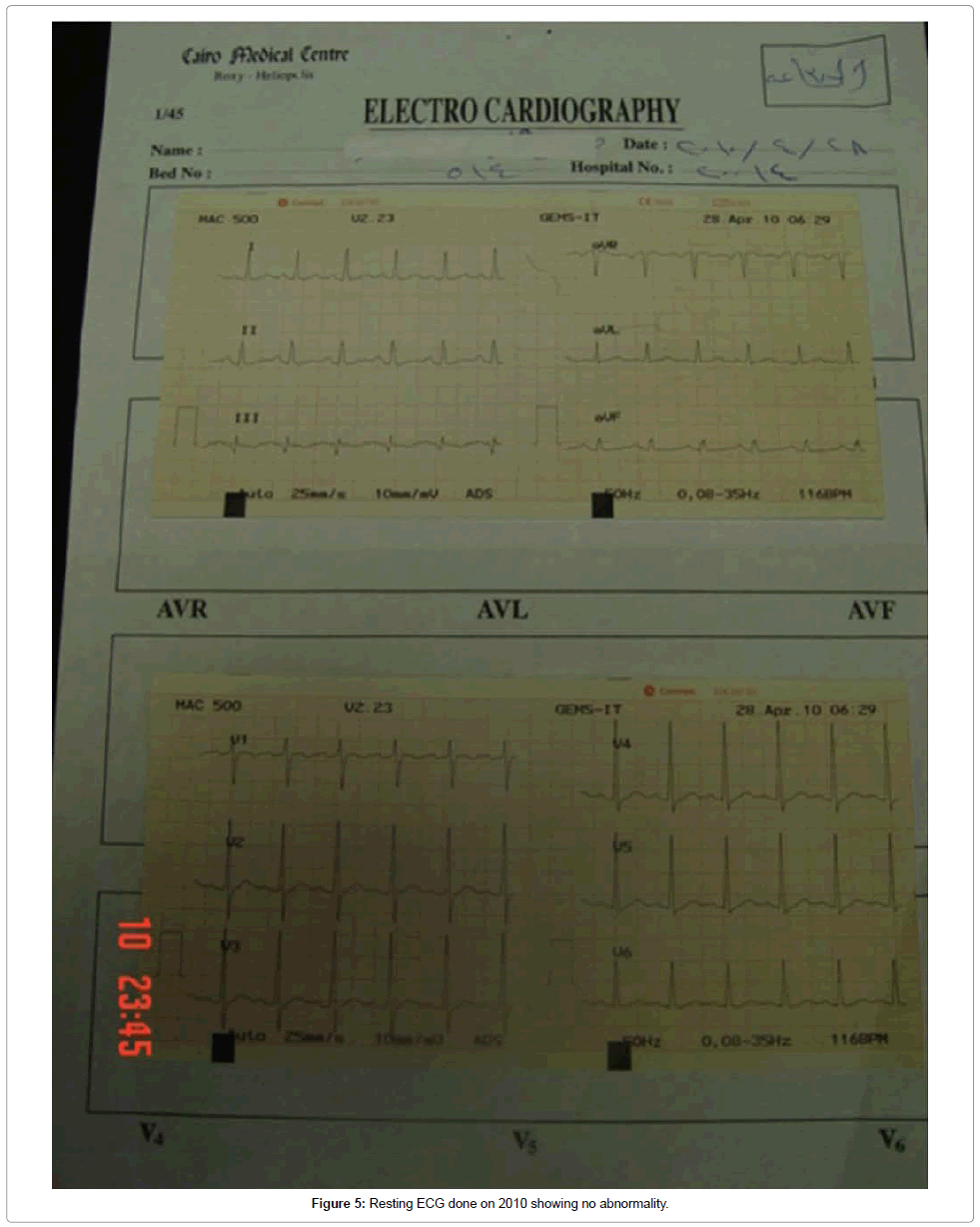
Figure 5: Resting ECG done on 2010 showing no abnormality.
On 2013 the findings on Doppler echocardiography were nearly similar to those on 2006, with no evidence of SWMA (Figure 6) and the resting ECG was also normal (Figure 7).
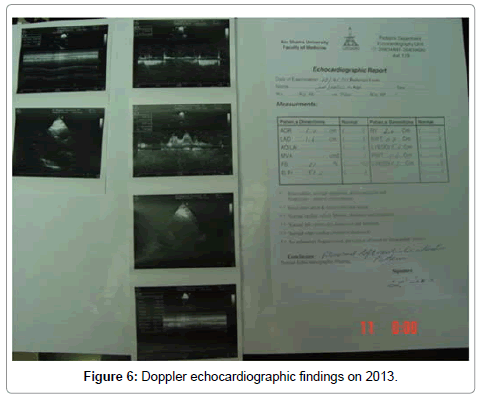
Figure 6: Doppler echocardiographic findings on 2013.
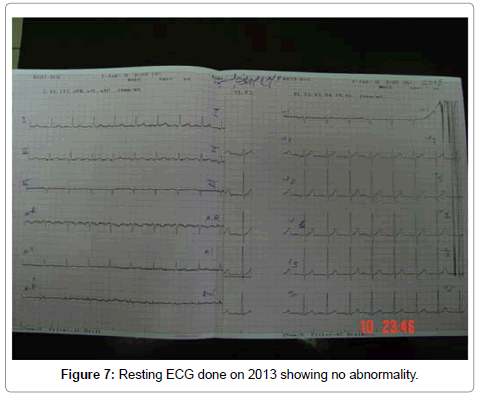
Figure 7: Resting ECG done on 2013 showing no abnormality.
During the study the patient did not develop cerebral stroke but suffered transient ischemic attacks; nearly once or twice per year.
On October, 2008 manifestations of peripheral neuritis became evident. On November, 2009 he developed a wound in the sole of the left foot as a result of his attempt to remove callus at the base of the left big toe using a cutter. Only topical honey was used for wound dressing.
On February, 2010 fundus examination showed non proliferative diabetic retinopathy with macular edema of the left eye.
On April 22, 2010, fluorescein retinal angiography revealed severe non-proliferative diabetic retinopathy with cystoid macular edema in the left eye. The right eye showed moderate non-proliferative diabetic retinopathy with focal maculopathy (Figure 8). A few minutes after injecting the fluorescein dye he developed anaphylaxis from which he was successfully treated. Two days after the procedure the wound at the base of the left big toe became gangrenous and the infection extended to involve most of the dorsum of foot (Figure 9). He refused to do below knee amputation and was discharged against medical advice after 12 hour hospital stay. On May 2, 2010 he was readmitted to another hospital and only wound debridement was done as he was still refusing below knee amputation (Figure 10). He remained in the hospital for 4 days during which he received insulin and antibiotics. After hospital discharge he continued both honey and insulin therapy. Amputation of the left big toe was done on June 18, 2010 based on the surgeon’s assumption that the deeply infected big toe might hinder the rate of healing process. On July 24, 2010, he stopped insulin. With topical honey the wounds healed completely on March 2011 (Figures 11 and 12).
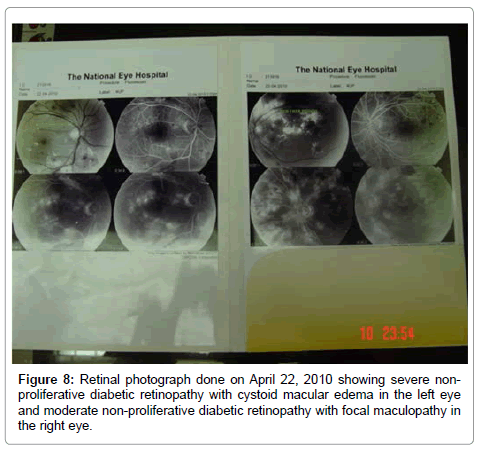
Figure 8: Retinal photograph done on April 22, 2010 showing severe nonproliferative diabetic retinopathy with cystoid macular edema in the left eye and moderate non-proliferative diabetic retinopathy with focal maculopathy in the right eye.
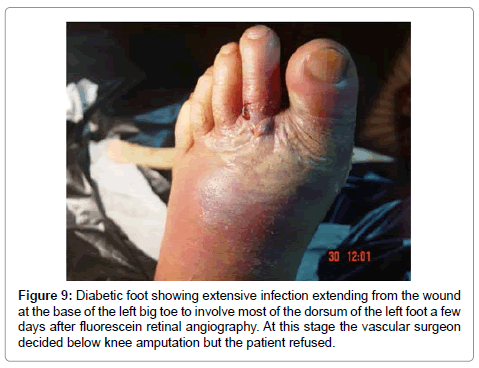
Figure 9: Diabetic foot showing extensive infection extending from the wound at the base of the left big toe to involve most of the dorsum of the left foot a few days after fluorescein retinal angiography. At this stage the vascular surgeon decided below knee amputation but the patient refused.
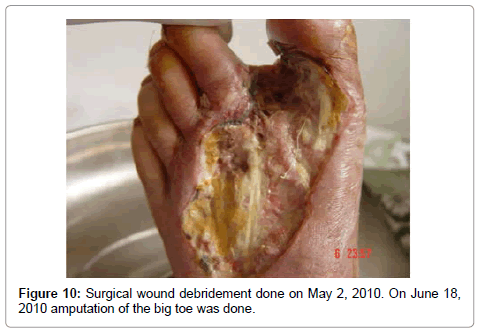
Figure 10: Surgical wound debridement done on May 2, 2010. On June 18, 2010 amputation of the big toe was done.
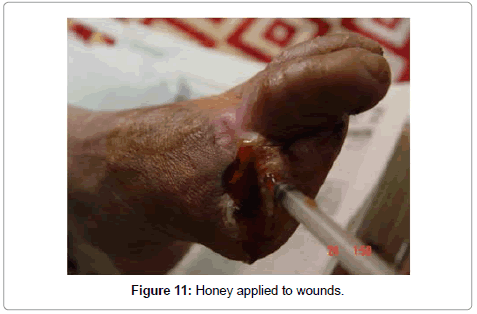
Figure 11: Honey applied to wounds.
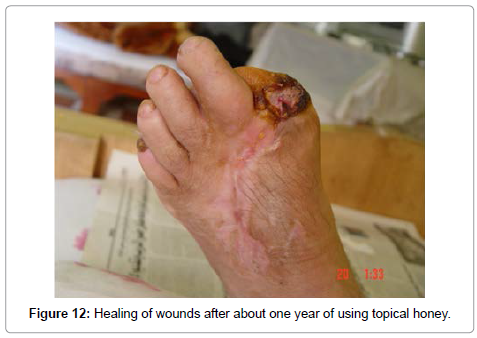
Figure 12: Healing of wounds after about one year of using topical honey.
Laser photocoagulation was done to both eyes on August 9, 2010 and the patient refused to do it again. Thereafter repeated fundus examination did not show progression of retinopathy.
On June 28, 2011 a small ulcer developed at the tip of the 2nd left toe. The lesion progressed to gangrene (Figure 13) and the patient also refused to amputate the toe, and continued using topical honey for dressing. Complete healing occurred but the rate of healing was slow (Figure 14).
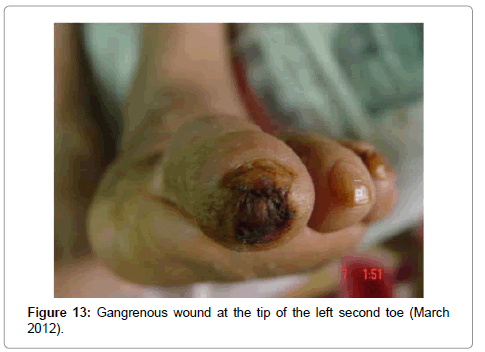
Figure 13: Gangrenous wound at the tip of the left second toe (March 2012).
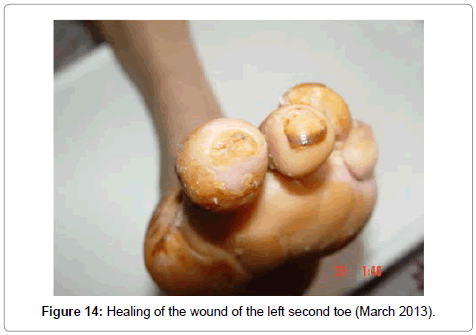
Figure 14: Healing of the wound of the left second toe (March 2013).
Apart from diabetic foot the patient did not develop other serious infections, and although he did not receive the anti-pneumococcal and influenza vaccination, the frequency and duration of respiratory tract infections reduced significantly.
The story of this patient did not end yet and follow up is still going on.
Although a final conclusion could not be drawn from a single case, the results of a single case study may sometimes highlight important observations and questions.
In this case there is one of two possibilities: First, the results observed are due to effects of honey. Second, these results might represent a natural course of the patient’s disease.
If the second possibility is true, this will raise important questions: First, why did not this persistent hyperglycemia and dyslipidemia in this patient lead to deterioration of his CHD and hypertension, development of other macro-vascular complications like cerebral stroke, or both? Second, why did not these high levels of blood glucose, which sometimes exceeded 500 mg/dL, lead to ketoacidosis or hyperosmolar coma particularly during periods of stress and during the fasting month of Ramadan?
We have not found in the literature reported cases type 2 DM, hypertension and CHD which showed, in the presence of long standing dyslipidemia and uncontrolled, hyperglycemia, decrease or at least stabilization of their macro-vascular complications.
Therefore the first possibility that these effects are due to honey is more likely. So the question is: Would honey have the potential to prevent or decrease the macro-vascular complications of type 2 DM?
The effects of only 8-week honey consumption in patients with type 2 DM were demonstrated in the study of Bahrami et al. [7] who found that honey intake resulted in weight reduction and improved lipidemia, but the levels of HbA1c increased. In their study the patients did not stop their medications. Although we cannot compare the findings of Bahrami and colleagues’ study, which was a randomized controlled study with many participants, with the findings of our single case study, yet these findings may raise an important question: would honey together with traditional anti-diabetic medicines have the potential to improve lipid profile, and hence to prevent or reduce both macro- and micro-vascular complications? This is because in our case, although the macro-vascular complications decreased, the lipid profile did not improve and the patient developed micro-vascular complications. To answer this question, well designed randomized controlled studies in large cohorts of patients are recommended to evaluate whether intake of honey, as a complementary agent, concomitantly with anti-diabetic treatment has the potential to prevent, cure or reduce both macro-and micro-vascular complications of diabetes.
There is a general agreement that glycemic control is needed to reduce the complications of diabetes. However there is still controversy regarding the levels of blood glucose optimal to achieve this goal. Although intensive control of glycemia might decrease micro-vascular complications, no marked effect has been reported on macro-vascular complications or all-cause mortality. Moreover intensive glycemic control may be associated with an increased risk of mortality [4-8]. Furthermore, compared to persistent hyperglycemia, intermittent hyperglycemia, i.e. glucose spikes, induces apoptosis of vascular endothelial cells [9]. Also considerable data have accumulated Figure 6: Doppler echocardiographic findings on 2013. indicating that elevated Postprandial Glucose (PPG) levels, even in the absence of high Fasting Blood Glucose (FBG), increase the risk for Cardiovascular Disease (CVD) [10,11]. Therefore, besides controlling overall glycemia, reduction of PPG and adjusting fluctuations of blood glucose might also be needed to prevent or treat CVD. However to achieve such an “ideal” glycemic control using only conventional anti-diabetic medicines may be faced by hypoglycemia as a major risk obstacle. Previous studies have shown that honey has an attenuated postprandial glycemic response [3,12-16]. In our case, because the macro-vascular complications are reduced in spite of high HbA1c, it might be suggested that honey intake reduced PPG levels and prevented glucose spikes which seem more important parameters than HbA1c in predicting major cardiovascular events. This might address questions: First, what would be the ideal PPG level in patients with type 2 diabetes; is it an ideal level per se [17] or an ideal FBG/PPG ratio? Second, what would be the ideal range of blood glucose fluctuations or spikes below which no major cardiovascular events would be predicted? Future studies might answer these questions.
In vitro and animal studies have demonstrated that honey reduced the oxidative stress in diabetes [5,18-20], a factor contributing to vascular dysfunction [21]. Therefore it might also be suggested that honey, by reducing vascular reactive oxygen species and increasing bioavailability of nitric oxide [5,20,22] might reduce or prevent deterioration of endothelial function.
Randomized clinical trials have demonstrated the vascular benefit of lowering blood pressure to < 140 mmHg systolic and <80 mmHg diastolic in individuals with diabetes [23]. This goal was nearly achieved in our case and thus might also be a contributing factor in preventing stroke and reducing major cardiovascular events.
Although intensive lowering of LDL cholesterol using statins has been established as an effective therapy to lower cardiovascular risk [24], the risk of major cardiovascular events remained in the range of 20% after 3 years of follow-up after an acute coronary syndrome [25]. Moreover, measurement of LDL cholesterol may not accurately reflect the true burden of atherogenic small LDL particles [26]. Also measurement of HDL cholesterol alone may not accurately reflect the anti-atherogenic capacity of HDL [27]. It has been suggested that apo B and apo A-1 may not only be relevant predictors of CHD [28] but even may provide more accurate information than LDL and HDL [29].
In our case the abnormal serum lipid profile persisted throughout the study period. However a single measurement of apo A-1 done on 2013 found it normal. ApoA-1 plays a critical role in preventing and reducing astherogensis [30-32]. Therefore preservation of Apo A-1 might also be a possible mechanism by which honey may prevent or reduce astherosclerosis. It might also be suggested that honey might have inhibited the formation of oxidized LDL [5], or might have reduced the burden of atherogenic small LDL particles which were not measured in our case; or both.
C- peptide levels have been used as a biomarker of β-cell function [33]. However, in type 2 diabetes higher C-peptide levels were found in some studies to be related to atherogenesis [34,35]. On the contrary, patients who had type 2 diabetes remission after bariatric surgery were found to have higher C-peptide levels than those without remission [36]. In addition, low C-peptide, especially the postprandial C-peptide level, was found to be a predictor of oral hypoglycemic agent failure in patients with type 2 diabetes who have high blood glucose level or longstanding diabetes [37].
In our case a single measurement of C-peptide done on 2013 showed normal fasting, and elevated postprandial level. Based on this observation it might be suggested, at least in this patient, that high C-peptide level might not be a predictor of CVD in type 2 DM.
Patients with diabetes are at increased risk of infections [38]. Respiratory tract infections are responsible for a significant number of medical appointments by persons with DM compared to those without DM [39]. Some infections almost always affect only persons with diabetes, such as malignant external otitis, rhinocerebral mucormycosis, and gangrenous cholecystitis [38]. Although some infections in DM are potentially serious, infectious diseases in general may predispose to ketoacidosis and coma in patients with diabetes. Although our case remained with persistent hyperglycemia for almost eleven years, serious infections did not develop. However the patient developed severe wound infection that ultimately resulted in amputation of his left big toe. In spite of being severe, the wounds, including the surgical ones, healed with topical honey without antibiotics. Furthermore although our patient did not receive the anti-pneumococcal and influenza vaccination, the frequency and duration of respiratory tract infections reduced significantly as compared with the situation before honey therapy. These findings might support the evidence that honey has also anti-microbial effects [6].
In conclusion; randomized controlled studies in a large cohort of patients are recommended to verify whether honey could act as a multi-targeted agent in type 2 DM.
Study interactions and ethical considerations
No ethical clearance had been sought before this trial because it was not expected to continue this trial for even a few days. Furthermore there is no strong scientific evidence that supports the use of honey as a sole treatment in diabetes and no one would accept stoppage of drugs in a patient with such kinds of diseases. Therefore it would be expected that no ethics committee or an institutional organization could accept such kinds of trials which might expose the patient to life threatening events. Because it has been reported in some studies that honey consumption might improve glycemia in DM [3] and might have cardio protective effects through its anti-oxidant properties [4,5], it was initially planned to start oral honey in large empirical doses (2 gm/kg body weight/day) aiming at producing fast effects. Also because the patient stopped his medicines, it was expected that these effects, which might be worrisome or beneficial, will appear within a few hours or maximum few days. The possibility of termination of this study in a matter of a day or few days was higher than the possibility of its continuation. Unexpectedly during the first 3 weeks of the study the patient’s condition remained stable and the levels of blood pressure and blood glucose remained within nearly the same range as before starting honey. However after the third week it was decided to stop the trial because of polyuria and worsening of hyperglycemia even though there was no dehydration, ketoacidosis or even ketones in urine. Because there was still a strong possibility that this hyperglycemia might untimely lead to complications, particularly acute complications; the patient was advised to resume his medicines and to stop honey. However the patient continued the trial because, as he reported, his exercise tolerance improved and he became able to perform his daily activities without chest pain. Since discovery of his CHD, the patient has been afraid from sudden death at any time. He was not convinced that conventional medicines will save his life because his father and some of his relatives and friends died of CHD in spite of being compliant to their medications and in spite of fair control of blood sugar. With continued honey consumption as a sole treatment, unexpectedly the polyuria decreased, the rate of weight loss also decreased and the blood pressure started to be normalized, along with improving exercise tolerance. At this stage it was realized that the patient’s cardiovascular status improved. However there was still a possibility that these effects might be temporary and the patient might be prone to develop complications especially micro-vascular complications at any time. Throughout the study which started on 2002, the patient was exposed to all kinds of pressure from his family as well as from consultants in cardiology and diabetes to stop this risky trial but he did not respond and he continued the trial for almost 11 years. On 2007, his elder brother developed sudden cardiac arrest and died a few months after coronary bypass grafting. This incident has led the patient to be more insistent to continue the trial. However, on 2010, when he developed diabetic foot, he was convinced to use insulin to control his blood sugar. At that time his cardiovascular status was already stabilized and there was no need to use other drugs. However after about three months he stopped insulin. Especially after the patient has developed micro-vascular complications I have tried to convince him to use insulin and to reduce the doses of honey in an attempt to produce fair glycemic control to prevent or at least to reduce the progress of these complications. However he did not also respond because he has already built the conceptions that his cardiovascular status remained stable with “honey’s hyperglycemia” and that honey will also be able to heal his micro-vascular complications.
The patient’s consent in its written form was provided years after beginning of this trial; mainly for publication purposes. In the light of the current controversy regarding the management of diabetes complications and in the light of the results of this long term case study, we have tried to convey a message that might be of help for patients with diabetes.