Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2014) Volume 4, Issue 2
Purpose: To investigate histopathological characteristics, we retrospectively analyzed data from patients who underwent resection of renal cell carcinoma pancreatic metastases (RCC-PMs). Methods: This study included 34 RCC-PM lesions in 13 patients who underwent 15 pancreatic operations. The clinicopathlogical characteristics were analyzed with special emphasis on tumor capsular formation, manner of peritumoral invasion, and presence of lymphovascular invasion. Results: Median duration to onset of RCC-PMs was 101 months from initial nephrectomy. Surgical procedures included distal pancreatectomy in 6 cases, pancreaticoduodenectomy in 4, total pancreatectomy in 1, and limited resections in 6 with two overlapping procedures. No perioperative deaths were encountered. One, three, and five year survival rates after pancreatic resection were 86.2%, 86.2%, and 76.6%, respectively. Of thirty- four lesions 32 lesions with tumor diameter ≤ 35 mm were encapsulated. Of these 32 lesions with capsule formation, extra capsular invasion was identified in 5 lesions. No lymphatic invasion was identified in any case. Venous invasion was presented just adjacent to the tumors in 2 lesions. Five year survival rates for the 11 cases with standard operations and 4 cases with limited resection were 70.7% and 100%, respectively without any significant difference. Conclusions: Small RCC-PMs were frequently encapsulated, seldom invaded into pancreatic parenchyma, and were rarely accompanied by microscopic lymph vascular invasion. Limited resection of the pancreas with adequate surgical margins may be oncologically acceptable.
<Keywords: Pancreatic metastases, Renal cell carcinoma, Invasive property, Limited resection of the Pancreas
Renal Cell Carcinoma (RCC) metastasizes to organs throughout the body, including the lungs, liver, bone, and skin. However, Pancreatic Metastases (RCC-PMs) are rare. In the accumulated literature concerning the resection of RCC-PMs, the number of reported cases has been limited to 236and 399 [1,2]. With recent advances in diagnostic imaging, metastatic lesions are being detected earlier, and experience with resecting RCC-PMs is increasing.
On imaging, RCC-PMs are characterized as well-demarcated, round masses with early enhancement [3,4]. Other pancreatic tumors that must be considered in the differential diagnosis include pancreatic endocrine tumors, but in patients with a history of RCC, the process of histological diagnosis by Fine Needle Aspiration (FNA), leading to a clinical diagnosis, is not difficult.
Treatment of RCC-PMs, when the metastatic organ is limited, is usually pancreatic resection. Indicated standard procedures include Pancreaticoduodenectomy (PD) and distal Pancreatectomy (DP). However, for small lesions ≤ 2 cm discovered during follow-up monitoring of RCC, whether such invasive surgery is appropriate is now somewhat controversial. RCC itself is slow-growing, and lymph node dissection is said to be unnecessary for PMs. Based on the conception of pancreatic parenchymal and organ-preserving operations, the indications for limited surgery are now being debated [5].
Therefore, we histopathologically analyzed lesions in our own series of patients with RCC-PMs to elucidate the pattern of progression into the surrounding pancreatic parenchyma and evaluate the appropriateness of limited resection of the pancreas.
Among 344 cases of pancreatic resection performed at Sapporo Medical University Hospital between January 1996 and December 2009, the present study included a total of 13 patients (8 men, 5 women) who underwent 15 surgical resections of 34 lesions histopathologically diagnosed as pancreatic metastases of RCC (RCC-PMs). The attending surgeons determined surgical procedures according to the basic concept of oncological resection with preservation as much pancreatic parenchyma as possible to avoid total pancreatectomy. Standard operations included pancreaticoduodenectomy with the preservation of pylorus ring or gastric antrum, distal pancreatectomy and total pancreatectomy. Limited resections were defined as procedures with the preservation as much pancreatic parenchyma and adjacent organ or structures as possible, which were named as duodenum-preserving pancreas head resection, middle pancreatectomy, spleen-preserving distal pancreatectomy and partial resection. In the 2 patients who underwent two resections each, standard operations (pylorus preserving pancreatico-duodenectomy and distal pancreatectomy) were initially performed, followed by limited resections (middle pancreatectomy and partial resection). Median age at the time of resection was 72 years (range, 48-80 years). The primary RCC was left-sided in 4 cases, right-sided in 8, and bilateral in 1. Histopathology of the primary tumor showed clear cell type in all cases. Median duration from initial renal operation to onset of PMs was 101 months (Table 1).
| Total numbers of patients and lesions | 13 patients | 34 lesions |
|---|---|---|
| Sex (men/women) | 8 men | 5 women |
| Age at pancreatic surgery (median, range) | 72 years (48-80 years) | |
| Initial pathology | clear cell carcinoma | |
| Initial RCC location | ||
| Left side Right side Bilateral |
4 8 1 |
|
| Interval from nephrectomy to pancreatic operations (median, range) | 101 months (0-228 months) | |
| Extrapancreatic metastases (absent/present) | 8 / 7 | |
| Sites of extrapancreatic metastases | ||
| Lung | 4 | |
| Thyroid | 2 | |
| Gallbladder | 1 | |
| Adrenal gland | 1 | |
| Main site of RCC-PMs | ||
| Ph | 6 | |
| Pbt | 7 | |
| Phbt | 2 | |
| No. of RCC-PMs | ||
| 1 | 9 | |
| 2-4 | 5 | |
| 14 | 1 | |
| Surgical procedures | ||
| Standard operation | 11 | |
| PD | 4 | |
| Dp | 6 | |
| TP | 1 | |
| Limited resection | 4 | |
| MP | 2 | |
| DpPHR | 1 | |
| Partial resection | 1 | |
*including 2 duplicated patients: **including 1 duplicated patient; ***including 1 repetition Ph. Pancreas head: Pbt. Pancreas body-tail: Phbt, Pancreas head-body-tail: PD. pancreaticoduodenectomy: DP. distalpancreatectomy: TP. total panen:atectomy: MP. middlepancreatectomy: DDPIIR, duodenum-presening pancreas head resection.
Table 1: Characteristics of patients undergoing pancreatic operations for RCC-PMs, main site of RCC-PMs and pancreatic operations
Survival rates after standard operations and limited resection were assessed using Kaplan-Meier analysis. Histopathological analysis included tumor capsule formation (Figure 1a,b), extra capsular invasion (Figure 1c,d), microscopic venous invasion(Figure 1e,f), and lymphatic invasion. Microscopic venous and lymphatic invasions were further assessed by Elastica van Gieson and D2-40 immuno staining, respectively. Two pathologists (Y.K. and T.H.) performed the histopathological analyses.
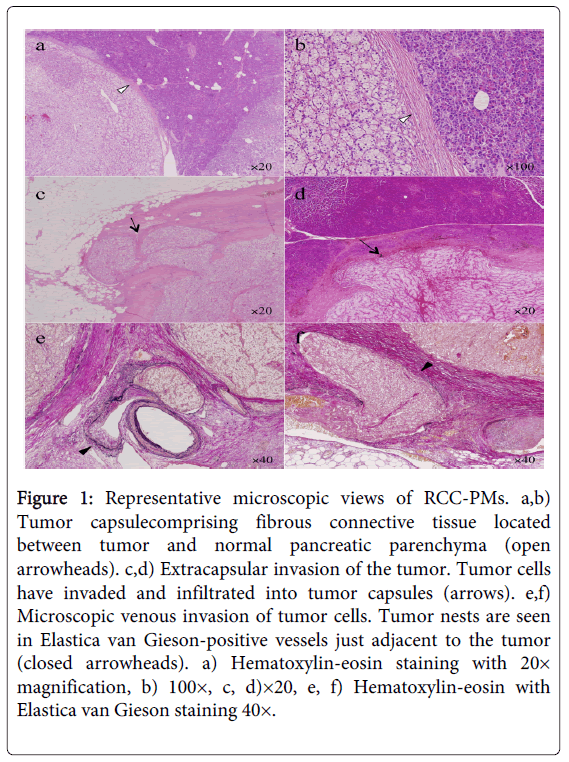
Figure 1: Representative microscopic views of RCC-PMs. a,b) Tumor capsulecomprising fibrous connective tissue located between tumor and normal pancreatic parenchyma (open arrowheads). c,d) Extracapsular invasion of the tumor. Tumor cells have invaded and infiltrated into tumor capsules (arrows). e,f) Microscopic venous invasion of tumor cells. Tumor nests are seen in Elastica van Gieson-positive vessels just adjacent to the tumor (closed arrowheads). a) Hematoxylin-eosin staining with 20× magnification, b) 100×, c, d)×20, e, f) Hematoxylin-eosin with Elastica van Gieson staining 40×.
Statistical analyses were performed as appropriate using SPSS for Windows version 15.0 (Statistical Package for the Social Sciences, Chicago, IL). Categorical variables were compared using Fisher’s exact test, while continuous values were compared using the Mann-Whitney U test. Statistical significance was defined at the p<0.05 level. Data are presented as median and range.
The significance of this clinical study and the purposes of the methodology were explained to patients, and written informed consent for the handling of specimens and other laboratory results was obtained prior to enrolment.
The site of pancreatic metastases was the head in 5 cases, body in 4, tail in 1, head/body in 1, body/tail in 2, tail and head in 1, and whole pancreas in 1, with the main site of RCC-PMs in the head in 6 cases, body/tail in 7, and whole pancreas in 2. The number of PMs was 1 in 9 cases, 2-4 in 5 cases, and 13 in 1 case (Table 1), and the median number of metastases was1. Regarding previous and concomitant metastases to other organs at the time RCC-PMs were detected, only PMs were seen in 8 cases, while metastases to other organs were also present in 7 cases. Other metastatic organs were the lungs in 4 cases, thyroid gland in 2, gallbladder in 1, and adrenal gland in 1, including one repetition (1 patient with both lung and adrenal metastases). The reason for pancreatic resection in cases with extra-pancreatic metastases was: stabilized extra pancreatic metastases in 3 cases (lungs); complete resection of all metastases in 3 cases; and because of gastrointestinal (GI) bleeding due to duodenal invasion by tumor in 1 case.
The operative procedures were standard operations, including PD, DP, and total pancreatectomy (TP), in 11 cases; and limited resections in 4 cases. Limited resection included middle pancreatectomy (MP) in 2 cases, duodenum-preserving pancreas head resection (DpPHR) in 1, and partial resection in 1 case (Table 1). No perioperative deaths were encountered. The median duration of patient observation was 66.7 months (range, 4.4-111.7 months). One, three, and five year survival rates after pancreatic resection were 86.2%, 86.2%, and 76.6%, respectively (Figure 2a). In 4 cases, during follow-up observation, tumor-related deaths occurred due to RCC at 4.4, 11.4, 39.0, and 71.4 months. In the remaining 11 cases, although 4 cases survived but censored at 10.6, 20.8, 67.7, and 79.4 months, median survival has been 79.4 months (range, 10.6-111.7 months). Five year survival rates for the 11 cases with standard operations and 4 cases with limited resection were 70.7% and 100%, respectively; no significant difference was apparent (Figure 2b).
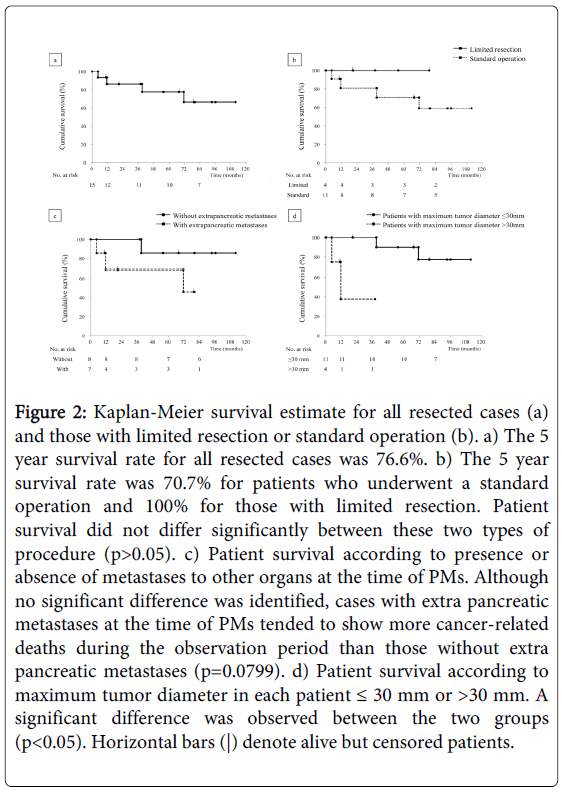
Figure 2: Kaplan-Meier survival estimate for all resected cases (a) and those with limited resection or standard operation (b). a) The 5 year survival rate for all resected cases was 76.6%. b) The 5 year survival rate was 70.7% for patients who underwent a standard operation and 100% for those with limited resection. Patient survival did not differ significantly between these two types of procedure (p>0.05). c) Patient survival according to presence or absence of metastases to other organs at the time of PMs. Although no significant difference was identified, cases with extra pancreatic metastases at the time of PMs tended to show more cancer-related deaths during the observation period than those without extra pancreatic metastases (p=0.0799). d) Patient survival according to maximum tumor diameter in each patient ≤ 30 mm or >30 mm. A significant difference was observed between the two groups (p<0.05). Horizontal bars (|) denote alive but censored patients.
The 34 PM lesions were histopathologically diagnosed as clear cell type RCC. There was no exposure of tumor cells to the surgical margins in all specimens analyzed, and complete surgical resection (R0) was confirmed in all cases. Median diameter of each tumor was 10 mm (range, 4-75 mm). Median maximum tumor diameter in each patient was 25.0 mm (range, 6-75 mm). Among the 34 RCC-PM lesions, 32 lesions in 13 patients showed capsule formation. Among these 32 lesions with tumor-capsule formation, tumor cells had invaded and infiltrated into the tumor capsules, a situation termed extra capsular invasion, in 5 lesions (Figure 3). Median distance of extra capsular invasion was 170 µm (range, 100-250 µm), showing that invasion was limited to a very adjacent area. In the 2 lesions of the 2 patients without capsule formation, invasive growth of the tumor into the surrounding pancreatic parenchyma and adjacent organs, duodenum and spleen was seen in each patient. Microscopic venous invasion was present in 2 of 34 tumors (Figure 3). The sites of venous invasion were in close proximity to the tumor, at 1 site in 1 case, and at 2 sites in the other. Neither lymphatic invasion nor metastases in resected lymph nodes were seen in any case. Correlations between tumor diameter and tumor-capsule formation, extra capsular invasion, or microscopic venous invasion did not reach the level of statistical significance, as the number of patients was not large and might not have allowed sufficient statistical power.
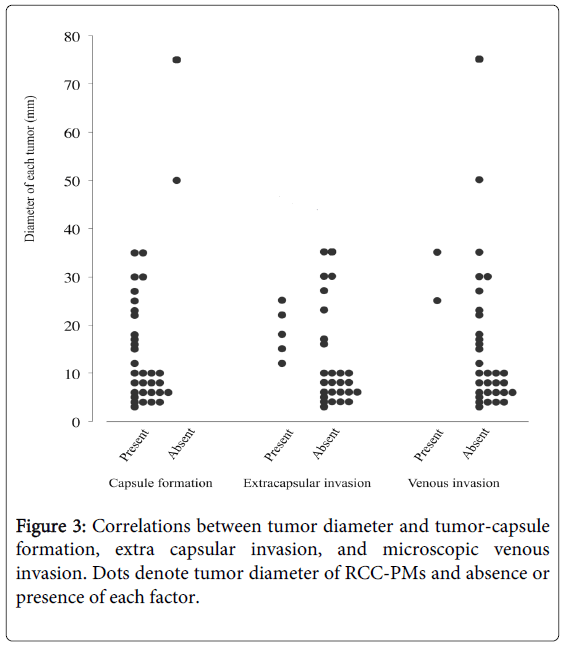
Figure 3: Correlations between tumor diameter and tumor-capsule formation, extra capsular invasion, and microscopic venous invasion. Dots denote tumor diameter of RCC-PMs and absence or presence of each factor.
Univariate analysis was carried out using factors of sex (men vs. women), age at the time of pancreatic operation, initial RCC location (left vs. right), interval from nephrectomy to pancreatic operation, number of RCC-PMs, single vs. more than two RCC-PMs, extra-pancreatic metastases (- vs. +), maximum tumor diameter in each patient, operative procedures (standard vs. limited), tumor capsule (- vs. +), extra-capsular invasion (- vs. +), and microscopic venous invasion (- vs. +). Those factors showing values of p<0.2 were further assessed in multivariate analysis with Cox proportional hazards regression modelling to identify prognostic indicators for cancer-related overall survival (OS).
In univariate analysis, maximum tumor diameter in each patient was the only significant predictor for cancer-related OS, and the presence of extra pancreatic metastases was the only other factor with p<0.2 (Table 2). Multivariate analysis revealed no significant predictors of cancer-related OS, but maximum tumor diameter in each patient showed a marginal odds ratio for cancer-related death of 1.073 (95% confidence interval, 0.999-1.151; p=0.053) (Table 2). Pathological characteristics of RCC-PM did not affect patient outcomes. Kaplan-Meier survival was estimated according to the presence or absence of metastases to other organs at the time of PMs, and to maximum tumor diameter in each patient (≤ 30 mm or >30 mm). Cases with extra pancreatic metastases, although not significantly different, tended to show more cancer-related deaths (Figure 2c), while cases with maximum tumor diameter >30 mm showed significantly poorer prognosis than those with ≤ 30 mm (p<0.05) (Figure 2d).
| Factors | Odds ratio | Univariate 95% CI | p | Odds ratio | Multivariate 95% CI | p |
|---|---|---|---|---|---|---|
| Sex (men vs. women) | 1.034 | 0.142-7.539 | 0.973 | |||
| Age at pancreatic operation | 0.961 | 0.879-1.051 | 0.385 | |||
| Initial site of RCC (left vs. right) | 0.411 | 0.057-2.958 | 0.378 | |||
| Interval from nephrectomy to pancreatic operations (months) | 0.997 | 0.984-1.010 | 0.614 | |||
| Number of RCC-PMs | 0.552 | 0.096-3.181 | 0.506 | |||
| RCC-PMs (1 vs. ≥2) | 0.545 | 0.056-5.283 | 0.600 | |||
| Extrapancreatic metastases (- vs.+) | 4.715 | 0.483-46.054 | 0.182 | 2.519 | 0.187-33.869 | 0.486 |
| Maximum tumor diameter in each patient (mm) | 1.082 | 1.009-1.159 | 0.026 | 1.073 | 0.999-1.151 | 0.053 |
| Operative procedures (standard vs. limited) | 0.032 | 0-726.249 | 0.501 | |||
| Tumor capsule (- vs. +) | 0.000 | 0-1.412e+60 | 0.880 | |||
| Extracapsular invasion (- vs. +) | 1.086 | 0.110-10.688 | 0.943 | |||
| Microscopic venous invasion (- vs. +) | 0.040 | 0-12059.673 | 0.617 |
Table 2: Predictors for Cancer-related overall Survival
These results revealed that the treatment protocol in our institution was generally acceptable and applying limited resection of the pancreas to patients carrying small RCC-PMs did not increase the risk of death from cancer progression.
With RCC, 20-30% of patients have metastases at the time of discovery [6]. Recurrence and metastases after radical surgery occur in 14.6% of cases [7]. Sites of tumor metastases and recurrence include the lungs, bone, skin, liver, and locally, whereas metastases to the GI tract and pancreas are relatively rare. The incidence of PMs is reportedly around 2.8% in clinical cases [8] and 6% in autopsy cases [9]. In general, these tend to be hematogenous metastases, but this has not been confirmed. Primary RCC may be associated with lymph node metastases [10]. In addition, microscopic venous invasion in primary lesions is reported to be a high risk factor for postoperative recurrence [7]. So both lymphogenous and hematogenous routes may contribute to metastases. In the present study, no lymphatic invasion was observed around PMs; thus, at least in terms of the mechanisms underlying RCC-PMs, the contribution of the lymphogenous route might be small.
Clinicopathological features of patients with RCC-PMs include a mean age of 60 years at recurrence, with a slight preponderance of males. No difference in primary tumor site was evident (left vs. right), and no differences were seen in the site of PMs or number of metastases (solitary vs. multiple). Most metastases are metachronous (86-88%) rather than synchronous (12-14%). In patients with metachronous metastases, the mean time to recurrence after RCC surgery is about 10 years [1,11]. In our case series, median patients age were almost 10 years older than previous reports, and primary RCCs predominantly involved the right side, despite previous descriptions. The median interval from nephrectomy to pancreatic operations was consistently 101 months in our study.
Regarding treatment for RCC-PMs, resection yielded a 5 year survival rate of 68-75% [12] and a mean survival of 19.8 years [11] has been reported. Favourable out comes can thus be expected. However, caution is necessary because extra pancreatic metastases may be a factor that influences subsequent survival time. Niess et al. [13] reported the outcome of patients with extra pancreatic metastases at the time of their resection and those with isolated pancreatic metastases. The median survival of patients with multi-organ disease (11 months) was significantly shorter than those without extra pancreatic metastases (64 months, p<0.05). In our study as well, cases with metastases to other organs at the time of PMs, although not significantly different, showed more cancer-related deaths during the observation period than cases without extra pancreatic metastases (Figure 2c).
Conventional cytotoxic chemotherapeutic agents and hormonal therapies have little impact on survival in patients with metastatic RCC and response rates are usually <10% [6]. Until recently, cytokine therapy using interleukin 2 or interferon∂ was the mainstay of treatment. However, this approach yielded low response rates of <30% and a median survival of 1 year [14]. Therefore, in patients without extra pancreatic metastases or without enlargement of extra pancreatic metastases; aggressive surgical treatment for patients with PMs in whom resection is possible without residual lesions represents a therapeutic strategy that might be able to improve outcomes [4]. Moreover, in patients with factors that impair quality of life such as obstructive jaundice or GI symptoms associated with tumor enlargement, the indications for surgery should be expanded. Regarding operative procedures, the appropriateness of pancreatectomy to reliably resect PMs, the necessity of lymph node dissection, and the extent to which pancreatic parenchyma should be preserved have become controversial.
General characteristics of RCC-PMs are encapsulation, expansive growth, and well-demarcated borders. To date, pathological studies examining these characteristics have been extremely rare. In the present study, for tumors ≤ 3 cm, extra capsular invasion was observed in 16.7% of total lesions and 27.3% of all patients, whereas venous invasion was seen in only 3.3% and 9.1%; and for tumors ≤ 1.5 cm, the extra capsular invasion rate was 9.5% of all lesions and 20.0% of all patients, and venous invasion rates were 0% respectively. For larger lesions with tumor diameter ≥ 5 cm, invasion into adjacent structures tended to be seen, but smaller lesions were quite localized and had a low propensity for invasion or metastases. The reported cases with resected RCC-PMs were mostly clear cell type of RCC. To our knowledge there might be reportedly no other types of RCC that underwent pancreatic resection. It would be hypothesized that clear cell type-RCC might have an affinity to the pancreas.
With regard to limited resection of RCC-PMs, no volume studies have been reported, only sporadic cases [4]. In the present study, 4 cases underwent limited resection, and tumor size in each patient ranged from 6 mm to 35 mm; in all cases, lesions were encapsulated, without extra capsular invasion. In one case, microscopic venous invasion was seen just adjacent to the tumor, but no recurrent lesions have been noted after 32 months of follow-up. Courses of all patients were uneventful during postoperative oncological follow-up. After limited resection, no new recurrent PMs have occurred in any case.
Histopathological analysis of RCC-PMs showed no metastases to regional lymph nodes; and for small lesions, there were little invasion into the peripheral pancreatic parenchyma, minimal venous invasion, and no lymphatic invasion. These findings suggest that limited resection of the pancreas might be an option to be taken into account for treating small and single RCC-PMs.