Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2014) Volume 3, Issue 1
Hepatosplenic T cell lymphoma (HSTL) is a rare entity of primary T cell lymphoma, characterized by pancytopenia, hepato-splenomegaly, and sinusoidal or sinusal infiltration of the liver and the spleen. This report describes a rare presentation of a case of HSTL with left shift leukocytosis, thrombocytosis, mild hepatomegaly along with an initial presentation of acute fulminant hepatic failure and bone marrow picture further confusing with chronic myelomonocytic leukemia(CMML). Contrary to the initial suspicion of hepatic infiltration of CMML, ultrasound guided liver biopsy showed leukemic infiltration into hepatic sinusoids with minimal cholestasis. Specific immunostaining of bone marrow revealed predominance of CD3+ T cells with negativity for other cell surface markers. Genetic analysis of bone marrow demonstrated trisomy 8 and isochromosome 7q, thus strongly suggesting hepatosplenic T-cell lymphoma (HSTL). This case report describes the complexity of diagnosing hepatosplenic T-cell lymphoma in a patient presenting with advanced liver disease and bone marrow biopsy finding initially suggestive of CMML.
<Hepatosplenic T cell lymphoma (HSTL) has been recognized as a distinctive clinico pathological entity among peripheral T cell lymphomas [1,2]. Typically, this lymphoma occurs at a young age and is characterized by hepatosplenomegaly, anemia, thrombocytopenia, no superficial lymphadenopathy, and an aggressive clinical course. Patho-histologically the lymphoma shows simusoidal/sinusal infiltration of liver, spleen and bone marrow. However, malignant lymphomas arising in the spleen are very rare and usually constitute less than 3% of all non-Hodgkin’s lymphomas [3]. More specifically, most of the splenic lymphomas by enlarge originate from the B-cells. In contrast to this Farcet et al. [4] in 1990 described two peripheral γδ T cell lymphoma with predominant infiltration of the liver and the spleen. Eventually in 1994 the Revised European American Lymphoma (REAL) classification has adopted heptosplenic γδ T cell (HSTL) as a distinct lymphoma entity [5]. Although previous reports have shown that thrombocytopenia and circulating blast-like lymphoma cells in HSTL makes this condition erroneously mis-diagnosed as idiopathic thrombocytpenicpurpura [6] and acute lymphoblastic leukemia [7] respectively, in this case report we present a novel clinical presentation of HSTL with thromobocytosis, monocyte predominant leukocytosis with left shift, no circulatory blast cells, and hypercellular bone marrow and thus perplexingly mimicking chronic myelomonocytic leukemia (CMML).
The patient is a 58 year old caucassian male with past medical history of hyperlipidemia presented with bilateral swelling of lower extremities and altered mental status. His past medical history was predominantly unremarkable. Family history was significant for unknown cancer in mother. Physical exam revealed 1+ pitting edema in bilateral lower extremities. Abdomen was remarkable for mild hepatomegaly and non-tender, non-distended abdomen. Heart and lung examination was with in normal limits. Patient appears to be well oriented to time, place and person.
The laboratory studies including the complete blood picture and liver function tests were shown in Tables 1 and 2, respectively.
| Complete Blood Count: | ||
| RBC | 3.93 million/μL | |
| WBC | 30,400/μL | |
| Platelets | 27,000/μL | |
| Hemoglobin | 13.3 g/dL | |
| Hematocrit | 42.30% | |
| MCV | 107 fL | |
| Differential: | ||
| Monocyte | 37% | |
| Electrolytes: | Within Normal Limits | |
| BUN | 25 mg/dL | |
| Ammonia | 75 μmol/L | |
| Coagulation Profile: | ||
| PT | 15.8 seconds | |
| INR | 1.3 | |
Table 1: Complete Blood Profile.
| Liver Function Tests | |
| Alkaline phosphatase | 535 U/L |
| LDH | 863 U/L |
| AST | 157 U/L |
| ALT | 57 U/L |
| Total Protein | 5.8 g/dL |
| Albumin | 2.5 g/dL |
| Bilirubin | 2 mg/dL |
Table 2: Liver Function Tests.
The initial abdominal ultrasound showed mild hepatomegaly especially of the left lobe but otherwise normal liver; Gall bladder and bile ducts are normal. The CT/Abdomen showed mild hepatosplenomegaly. The preliminary bone marrow biopsy was hyper cellular and consistent with myelodysplastic syndrome/ Chronic myelomonocytic leukemia and probable acute progression on to acute leukemia (Figure 1).
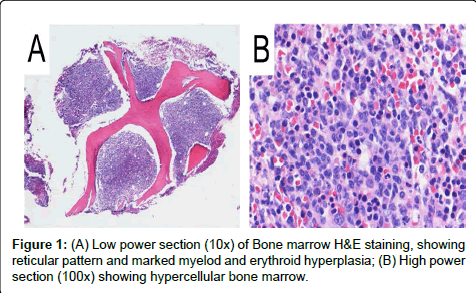
Figure 1: (A) Low power section (10x) of Bone marrow H&E staining, showing reticular pattern and marked myelod and erythroid hyperplasia; (B) High power section (100x) showing hypercellular bone marrow.
The patient was admitted to our hospital. The clinical course of this patient during hospital stay within 4 days following admission was significant for the development of new symptoms of icterus and rapid deterioration of mental status. The LFTs were rapidly elevating including 2-3 fold raise of serum levels of bilirubin, AST, and 2 fold raise of Alkaline phosphatase from initial admission. A working diagnosis of infiltrative CMML to liver was proposed and liver biopsy was obtained.
Ultrasound guided liver biopsy showed leukemic infiltration into hepatic sinusoids with minimal cholestasis (Figure 2). Specific immunostaining demonstrated CD3+ cells in bone marrow (Figure 3A) and liver (Figure 3B). The genetic analysis of bone marrow demonstrated trisomy 8 and iso-chromosome 7q, thus strongly suggesting hepatosplenic T-cell lymphoma (HSTL). After discussing the prognosis and treatment options, patient and family members opted for hospice and comfort measures.
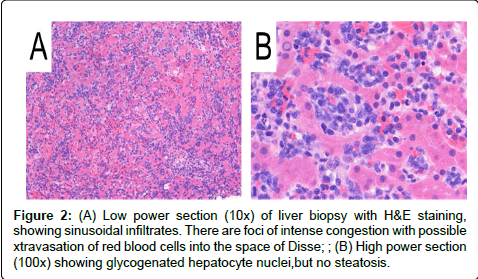
Figure 2: (A) Low power section (10x) of liver biopsy with H&E staining, showing sinusoidal infiltrates. There are foci of intense congestion with possible xtravasation of red blood cells into the space of Disse; ; (B) High power section (100x) showing glycogenated hepatocyte nuclei,but no steatosis.
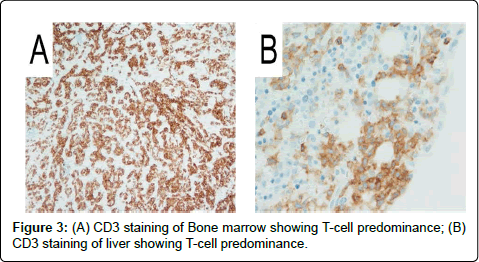
Figure 3: (A) CD3 staining of Bone marrow showing T-cell predominance; (B) CD3 staining of liver showing T-cell predominance.
In this report we present a case of HSTL with rare findings of leukocytosis and hypercellular marrow. Literature evidence suggested that the cytokines produced by the malignant T cells suppress the bone marrow precursor cells [8]. However, the evidence to support this hypothesis seems to have some deficiencies and needs further proof. A major challenge in diagnosis of HSTL may be due to the fact that thisrare entity is not frequently considered in the differential diagnosis. The common features of thrombocytopenia and circulating blast cells were frequently diagnosed as idiopathic thrombocytopenic purpura [6] and acute lymphoblastic leukemia [7], respectively. Further the presence of fever, jaundice, hepatosplenomegaly, and absence of peripheral lymphadenopathy commonly leads to a misinterpretation towards viral infection [9]. The exact pathogenesis in our patient is not clear. Although EBV has been suggested to have a potential pathogenic role in development of peripheral lymphomas [10], reports by Oshima et al. [11] argues against an essential role for EBV. Infact, studies by Sadahira et al. [12] have found that only 2% of lymphoid cells in HSTL patient had EBV infection, thus favoring a non-EBV etiology.
It has been shown in several neoplastic conditions and peripheral T cell lymphomas that liver involvement leads to sever hepatic damage, thus frequently mislead into diagnosing hepatobiliary disease [13]. Further, neoplastic cells mainly infiltratethe portal area and induce apoptosis of periportal hepatocytes leading to abnormal liver function tests such as elevation of AST, ALT enzyme levels. In contrast, the acute fulminant hepatic damage in HSTL, as also observed in our case report, is due to infiltration into sinosoidal spaces in the liver leading to atrophic degeneration of the hepatic cords, leading to intrahepatic cholestatis rather than parenchymal damage [6,14]. The exact immuno phenotype of the HSTL is still under considerable debate. Although CD3 cell marker has been shown in several reports, the use of other reported cell surface and intra cytoplasmic markers requires further evidence [1,15]. Although the T-cell receptor (TCR) of malignant T cells has been shown to be γδ in origin [16], Takaku et al. [17] have shown a αβ variant of TCR in HSTL. However, genetic analysis of the αβ variant of TCR demonstrated a normal karyotype, whereas the karyotype of the more common γδ variant of TCR in HSTL demonstrates a characteristic trisomy 8 and iso-chromosome 7q [5,18]. It is of interest to note that these γδ lymphomas have unusual clinico pathologic presentations, which include either midline granuloma or hepatosplenic lymphomas with a sinusal/sinusoidal infiltration in spleen, marrow, and liver. The fact that the distribution of the neoplastic γδ T cells in the splenic red pulp resembles that of normal γδ T cells reinforces the concept of a preferential homing of γδ T cells to this hematopoietic tissue [16]. Along with immunostaining, under questionable histo-pathological picture, some authors have recommended TCR gamma chain gene by polymerase chain reaction on the tissue biopsy (liver/spleen) to confirmed a clonal γδ T-cell proliferation [9]. Conflicting evidence can be noticed with regard to the expression of cytotoxic molecules TIA-1 (T cell intracellular antigen-1) and granzyme-B in HSTL [6]. Although several reports demonstrate the expression of cytotoxic moleculesTIA-1 and granzyme-B, report by Sadahira et al. [12] demonstrate an absence of expression of cytotoxic molecules, thus questioning their use as diagnostic markers of HSTL.
Much confusion has also been noticed in the current available therapeutic options of HSTL. Although various chemotherapeutic regimens including CHOP, m-BACOP, allogeneic bone marrow transplantation, splenectomy, etc have all been used, the success and 5-year survival of these patients quiet abyssmal at just 7% [1]. Complete remission is rarely noticed.The most encouraging evidence came from a report from M.D. Anderson Cancer Center, wherein, 7 out of 14 patients who received chemotherapy achieved complete remission [19]. However, the median survival still remained abysmal at 11 months (2-36 months) [19]. Further research towards appropriate chemotherapeutic intervention is warranted for effective treatment of HSTL.
To our knowledge and based on literature search, this is the first report of HSTL presenting with leukocytosis, thromobocytosis, acute fulminant liver failure, hyper cellular marrow in the absence of apparent comorbidities. An awareness of this entity will help in accurate early diagnosis of HSTL, especially given the high mortality of this disease.