Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2016) Volume 0, Issue 0
Rationale: Research supports the use of screening protocols to identify patients who are candidates for weaning from mechanical ventilation, and the use of spontaneous breathing trials (SBTs) to predict ability to breathe spontaneously. However, once daily screening is poorly aligned with 24-hour continuous care in the intensive care unit (ICU) environment and the most effective SBT technique is not known. The optimal strategy to liberate our sickest patients from ventilators remains to be determined. Objectives: To assess our ability to recruit critically ill adults and adhere to the screening and SBT protocols. Methods: We propose a pilot, factorial design, randomized trial comparing once-daily versus at least twice daily screening and pressure support (PS) ± positive end-expiratory pressure (PEEP) (inspiratory ± expiratory support) or T-piece (no support) as the SBT technique in critically ill adults who are invasively ventilated for at least 24 hours in 11 North American ICUs. Respiratory Therapists (RTs) will screen all enrolled patients between 06:00 and 08:00 hours daily to identify SBT candidates. Patients in the at least twice daily screening arms will also be screened between 13:00 and 15:00 hours; additional screening will be permitted at clinician’s discretion. Once a screening assessment is passed, an SBT will be conducted with the assigned technique. Outcomes: The study will be considered feasible if at least 1 to 2 patients per ICU per month are recruited and if the screening and SBT protocols are adhered to >80% of the time. Relevance: The availability of RTs in ICUs presents an important opportunity to screen patients more frequently, conduct more frequent SBTs, and reduce the duration of invasive ventilation and ICU stay. FAST Trial Registration: Clinical Trials.gov NCT02399267.
Keywords: Weaning; Spontaneous breathing trial; Screening; Randomized controlled trial
The use of invasive mechanical ventilation in critically ill patients can be lifesaving. Most patients admitted to adult intensive care units (ICUs) require invasive ventilation. Weaning is the process during which the work of breathing is transferred from the ventilator back to the patient. Almost 40% of the time spent on invasive mechanical ventilation is spent weaning [1]. Although invasive ventilation is effective, it is associated with the development of numerous complications including respiratory muscle weakness, ventilator associated pneumonia (VAP) [2] and sinusitis [3]. VAP is associated with increased morbidity and a trend toward increased mortality [4]. At the same time, premature or failed attempts at extubation necessitating reintubation are also associated with important complications including an increased risk of developing VAP [5], prolonged ventilation and ICU stay and increased mortality [6,7] Consequently, in their efforts to minimize the duration of invasive ventilation [8], clinicians are challenged by a ‘trade-off’ between the complications associated with protracted invasive ventilation and the risks associated with a premature failed attempt at extubation.
More than two decades of research support the use of specific strategies to limit the duration of invasive ventilation including the (i) use of multidisciplinary screening protocols to identify candidates for a spontaneous breathing trial (SBT) [9-11], (ii) conduct of SBTs [12-14] in patients who meet screening criteria, and (iii) use of specific modes and techniques [reductions in Pressure Support (PS) and once daily SBTs [PS ± positive end expiratory pressure (PEEP) or T-piece] [15-17] to discontinue support in patients who fail an initial SBT.
A systematic review and meta-analysis of 17 trials (n=2,434) found that use of screening protocols to identify SBT candidates is associated with a 26% reduction in total duration of mechanical ventilation [n=14 trials, 95% CI (13%-37%), p=0.0002], 70% reduction in weaning time [n=8 trials, 95% (CI 27%-88%), p=0.009], and an 11% reduction in ICU stay [n=9 trials, 95% CI (3%-19%), p=0.01] [18]. Only 1 trial (n=385) in this review compared twice daily screening led by allied health providers to usual care requiring a physician order to conduct an SBT and found a significantly shorter duration of ventilation and a trend toward a lower VAP rate in the twice daily screening group [11]. Trials included in the review had several methodologic weaknesses including limiting screening to once daily in the intervention arm, using ‘usual care’ as the comparator, and exclusion of patients who required common ICU interventions (vasopressor and/or sedative infusions) or who were anemic (hemoglobin concentration <100 g/L). No trial in this review compared a strategy of more frequent screening to once daily screening. Notwithstanding, findings from national and international surveys show that once daily screening is now standard of care [19,20]. The conduct of daily multidisciplinary ward rounds and once daily screening by Respiratory Therapists (RTs) in North American ICUs is poorly aligned with the continuous care environment of the ICU wherein a patient’s clinical status can change from hour to hour. Once daily screening also disregards the impact of management decisions made during morning rounds that may result in clinical improvement sufficient to pass a screening assessment that could be conducted later in the day. More frequent screening is typically not conducted in practice due to personnel limitations, task prioritization, existing protocols, clinical culture, and clinician reluctance to extubate patients later in the day. Although evidence supports once daily screening compared to usual care, this evidence is no longer relevant to current practice as once daily screening has become standard care [19,20]. Further, the use of once daily SBTs as a weaning strategy in patients who fail an SBT and require an alternative approach to liberate them from invasive ventilation is based on one trial of 64 patients [16].
SBTs are conducted to determine if a patient can breathe independently and are conducted using different techniques and durations. Although 3 techniques are commonly used to conduct SBTs [PS, continuous positive airway pressure (CPAP) and T-piece) in Canada [19], PS and T-piece are the most frequently used techniques internationally [20]. A consensus statement, the Task Force on Weaning, supports the use of either low levels of PS (5-8 cm H2O ± 5 cm H2O PEEP) or T-piece as techniques to conduct SBTs in adults [21]. It is not known if measurements obtained while the patient is on PS (added inspiratory support) overestimate the likelihood of successful extubation or if measurements obtained while the patient is on T-piece (no support) underestimate the likelihood of successful extubation.
Randomized trials support the use of either PS or T-piece to conduct SBTs and suggest that a 30 minute SBT is sufficient for most patients [12,13]. Patients included in these trials were ‘deemed ready for weaning by physicians’ and were not identified by daily screening. In a subgroup analysis, a recent Cochrane Review pooled 4 trials (n=940) that compared PS to T-piece SBTs and found that patients were significantly more likely to pass a PS SBT (RR 1.09, 95% CI 1.02 to 1.17) [22]. Compared to their review, our review included 9 additional trials (including 1 pediatric trial, 4 adult trials, 2 abstracts publications and 2 three-arm trials) that directly compared PS and Tpiece SBTs. Contrary to their findings, we found that although patients were as likely to pass an initial SBT with PS vs. T-piece, they were significantly more likely to be successfully extubated after a PS SBT [23].
Although there is a large body of evidence about weaning from mechanical ventilation, it is insufficient to guide clinical practice today and the most effective strategy to liberate critically ill adults from ventilators remains unknown. The continuous presence of RTs in many North American ICUs presents a unique opportunity to identify the optimal strategy.
In the Frequency of Screening and SBT Technique Trial (FAST Trial) , we will evaluate the feasibility of conducting an open-label, multicentre, factorial design trial in critically ill adults to identify SBT candidates (once vs. at least twice daily) and (ii) SBT technique [PS ± PEEP vs. T-piece (off ventilator, no CPAP/PEEP)] to assess a patient’s ability to breathe spontaneously. We will study 100 patients in 11 ICUs. This trial will be conducted under the auspices of the Canadian Critical Care Trials Group (CCCTG). The trial is registered in ClinicalTrials.gov: NCT02399267 and has been funded by the Canadian Institutes of Health Research. A diagram depicting the study design is shown in Figure 1.
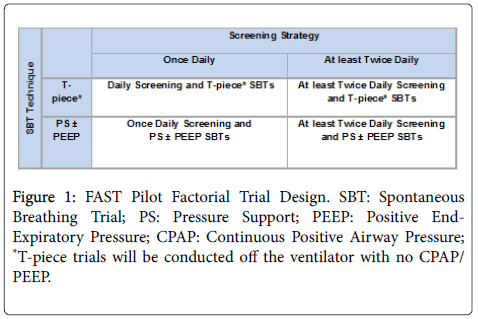
Figure 1: FAST Pilot Factorial Trial Design. SBT: Spontaneous Breathing Trial; PS: Pressure Support; PEEP: Positive End- Expiratory Pressure; CPAP: Continuous Positive Airway Pressure; *T-piece trials will be conducted off the ventilator with no CPAP/ PEEP.
Primary objective
[1] To assess our ability to recruit critically ill adults who can breathe spontaneously or initiate breaths on one of several commonly used modes of ventilation into the trial.
Secondary objectives
[2] To assess compliance with once daily and at least twice daily screening assessment protocols and the risk of contamination in the once daily arm. Similarly, we will assess compliance with PS and Tpiece SBT protocols and the risk of contamination in either arm,
[3] To quantify potential co-interventions in this unblinded study (sedation, analgesia and delirium management and timing of mobilization) that may lead to performance bias and may require protocolization or detailed documentation in a future, large scale weaning trial,
Tertiary objectives
[4] To identify barriers (clinician and institutional) to recruitment,
[5] To classify trial participants as those who require (i) simple, (ii) difficult or (iii) prolonged weaning using established definitions [21],
[6] To obtain preliminary estimates of the impact of the alternative screening (‘once daily’ vs . ‘at least twice daily’) and SBT techniques (PS ± PEEP vs . T-piece off ventilator with no CPAP/PEEP) on important outcomes [e.g., time to first SBT and first successful SBT, time to first extubation and successful extubation [24], total duration of mechanical ventilation, ICU and hospital length of stay, ICU and hospital mortality, the use of noninvasive ventilation (NIV) after extubation, and weaning-related complications (self-extubation, reintubation, tracheostomy) [24-27].
Research personnel (research coordinators and/or RTs) will identify, consent (where applicable), and enroll eligible patients from during regular weekday hours using a central randomization system stratified by ICU with variable undisclosed block sizes. Eligible patients (Table 1) will be randomly assigned to both a screening frequency (once vs. at least twice daily) and an SBT technique (PS ± PEEP vs. T-piece).
| ; Inclusion Criteria | Eligible patients are those (1) receiving invasive mechanical ventilation for>24 hours (2) capable of initiating spontaneous breaths on PS or PAV or triggering breaths on volume or pressure AC, volume or pressure SIMV ± PS, PRVC, VS or APRV (3) FiO2<70% and (4) PEEP<12 cm H2O |
| Exclusion Criteria | We will exclude patients (1) brain death or expected brain death (2) who have evidence of myocardial ischemia in the 24 hour period before enrollment, except if current trend in troponin is downward and it has been>24 hours since last troponin peak or the patient has undergone a revascularization procedure and attending physician has no concerns regarding ongoing ischemia (3) who have received continuous invasive mechanical ventilation for>2 weeks (4) who have a tracheostomy in situ at the time of screening (5) who are receiving sedative infusions for seizures or alcohol withdrawal (6) who require escalating doses of sedative agents (7) who are receiving neuromuscular blockers or who have known quadriplegia, paraplegia or 4 limb weakness or paralysis preventing active mobilization (e.g., active range of motion, exercises in bed, sitting at edge of bed, transferring from bed to chair, standing, marching in place, ambulating) (8) who are moribund (e.g., at imminent risk for death) or who have limitations of treatment (e.g., withdrawal of support, do not reintubate order, however, do not resuscitate orders will be permitted) (9) who have profound neurologic deficits (e.g. post cardiac or respiratory arrest, large intracranial stroke or bleed) or GCS<6 (10) who are using modes that automate SBT conduct (11) who are current enrolled in a confounding study that includes a weaning protocol, or (12) who were previously enrolled in this trial (13) patients who have already undergone an SBT or are on T-piece, or CPAP alone (without PS), or PS<8 cm H2O regardless of PEEP, or other ‘SBT equivalent’ settings immediately before randomization, (14) patients who have already undergone extubation [planned, unplanned (e.g. self, accidental)] during the same ICU admission. |
| PS: Pressure Support; PAV: Proportional Assist Ventilation; AC: Assist Control; SIMV: Synchronized Intermittent Mandatory Ventilation, PRVC: Pressure Regulated Volume Control; VS: Volume Support; APRV: Airway Pressure Release Ventilation; FiO2: Inspired Fractional Concentration of Oxygen; PEEP: Positive End-Expiratory Pressure; GCS: Glasgow Coma Scale; SBT: Spontaneous Breathing Trial; CPAP: Continuous Positive Airway Pressure. | |
Table 1: Inclusion and exclusion criteria.
After randomization, RTs in participating ICUs will be informed of the allocated study arms and practice checklists will be completed by bedside nurses. These checklists will record current practices in sedation, analgesia and delirium management, and whether patients are being passively or actively mobilized before SBTs, but their content will not influence progression to an SBT.
Given the minimal risk associated with the interventions being evaluated (screening frequency and SBT conduct) and the need to enroll patients as soon as possible after they initiate spontaneous or trigger breaths, we will request approval from participating Research Ethics Board (REB) to use a hybrid consent mode prioritizing patient or substitute decision maker (SDM) consent (for patients without decision-making capacity or when SDMs are available) and deferred consent (when SDMs are not available) where feasible [25]. For patients who are enrolled under deferred consent, consent will be sought as soon as possible after randomization. A similar hybrid consent model was used in two multicenter, pilot screening frequency trials comparing once daily screening to at least twice daily screening [26].
Screening for readiness to undergo a spontaneous breathing trial
In the once daily screening arms, RTs will screen invasively ventilated patients between approximately 06:00-08:00 hours daily. In the ‘at least twice daily’ screening arm, patients will be screened at a minimum between approximately 06:00-08:00 hours and between 13:00-15:00 hours daily. If a screening period is missed inadvertently or due to an investigation or intervention (e.g., operation/procedure) necessitating absence from the ICU, it may be conducted later the same day and ideally within 6 hours of the scheduled screening period. Additional screening trials in the ‘at least twice daily’ screening arms will be permitted at the clinician’s discretion.
To pass the screening assessment and undergo an SBT, all of the following criteria must be met:
1. The patient must be capable of initiating spontaneous breaths on PS or Proportional Assist Ventilation (PAV) or triggering breaths on volume or pressure Assist Control (AC), volume or pressure Synchronized intermittent mandatory ventilation (SIMV) ± PS, Pressure Regulated Volume Control (PRVC), Volume Support (VS) or Airway Pressure Release Ventilation (APRV),
2. The ratio of partial pressure of oxygen to FiO2 (PaO2/FiO2)>200 mmHg,
3. RR<35 breaths/min,
4. PEEP<10 cm H2O,
5. HR<140 beats/min,
6. The ratio of respiratory frequency to tidal volume (f/VT)<105 breaths/min/L during a 2 minute assessment on CPAP of 0 cm H2O (alternatively PS=0 cm H2O /PEEP=0 cm H2O).
Conduct of spontaneous breathing trials
After passing a screening assessment, patients will undergo an initial SBT with the assigned technique. All SBTs will be 30-120 minutes in duration [13]. SBTs will be conducted with PS <8 cm H2O with PEEP <5 cm H2O or T-piece (off ventilator with no CPAP/PEEP). Between SBT trials, patients will be returned to the mode of ventilation used before the SBT. Regardless of the SBT technique utilized, patients who pass an SBT will be assessed for extubation using standardized criteria. Extubation will be recommended to be done as soon as possible after passing an SBT.
We will use standardized criteria to determine SBT failure in all arms (Table 2). After an unsuccessful SBT, patients will be initially returned to the ventilator settings used just before the SBT. Ventilator settings will be adjusted to restore respiratory comfort, recognizing that some patients may meet criteria to return to a fully supported mode of ventilation.
| SBT failure criteria will be defined by the presence of any ONE of: |
| A respiratory rate (RR)>35 breaths/min with signs of respiratory distress or an increase in RR>20% from baseline with signs of respiratory distress |
| Oxygen saturation of arterial blood (SaO2) or pulse oximetry<90%; |
| Heart rate (HR)>140 beats/min with signs of respiratory distress or an increase in HR>20% from baseline with signs of respiratory distress |
| Systolic blood pressure >80 or <90 mmHg |
| The presence of somnolence, agitation, diaphoresis, or anxiety |
| Requirement for the addition of or an increase in vasopressor or inotropic agent support and |
| Chest pain or other limiting pain precluding further continuation |
Table 2: Criteria for failure of a spontaneous breathing trial.
Criteria to suspend the protocol and return to a controlled/ supported mode of ventilation
Patients will remain on a mode that permits spontaneous or triggered breaths between SBTs and during the night. However, patients will be permitted to return to/remain on a supported mode of ventilation without spontaneous or triggered breaths if selected criteria are met (Table 3). Patients who meet any of these criteria will be reassessed daily to identify the earliest time when they meet initial inclusion criteria and can initiate spontaneous breaths or trigger breaths and the screening and SBT protocols can be resumed as per treatment assignment.
| 1. | Surgery or invasive procedures requiring sedation, |
| 2. | Respiratory distress as defined by: Sustained hypoxemia [pulse oximetry oxygen saturation (SpO2)<90%] with an FiO2>60% and PEEP>10 cm H2O or hypercapnia with pH<7.30 or clinical respiratory distress. Repeated episodes (≥ 3 episodes within 1 hour) wherein an inspiratory pressure (drive pressure+PEEP on pressure modes or plateau pressure on volume modes) of 35 cm H2O or more is attained (despite suctioning, bronchodilation, etc.) |
| 3. | Hemodynamic instability despite fluid boluses and requirement for high dose vasopressors: norepinephrine>15 µg/min (0.2 µg/kg/min) or equivalent, |
| 4. | Suspected myocardial ischemia based on EKG and/or elevated Troponin I, |
| 5. | Neurologic deterioration with need to control PaCO2 (e.g., raised intracranial pressure) or central hypoventilation. |
| 6. | RR<10 breaths/min related to need for increased sedation, |
| 7. | PEEP>13 cm H2O, |
| 8. | FiO2>71%. |
Table 3: Criteria to suspend the protocol and return to a controlled/supported mode of ventilation. FiO2: Inspired Fractional Concentration of Oxygen; PEEP: Positive End-Expiratory Pressure; EKG: Electrocardiogram; RR=Respiratory Rate.
Extubation
All patients will be assessed for extubation after successfully completing an SBT. To be extubated the following criteria [24] will be met:
1. SpO2>90% (or at baseline level in chronically hypoxemic patients) on an FiO2<40% and PEEP<5 cm H2O,
2. A cough of sufficient strength to clear secretions and must not require suctioning more than every 2 hours,
3. Patients should be hemodynamically stable [off vasopressors or on minimal levophed i.e., <7 μg/min (0.1 μg/kg/min or equivalent),
4. A level of consciousness sufficient to ensure airway protection.
5. A cuff leak is present
All of the above criteria (except #4 and #5) will similarly apply to patients who undergo trach mask trials with a tracheostomy and are disconnected [28].
Other important considerations in the design of a weaning trial include titration of ventilator support, use of NIV after extubation, reintubation, and tracheostomy. These interventions will also be monitored and recorded [29].
In all four groups, we will collect daily data up to successful extubation, ICU discharge, ICU death or until day 60 after randomization (deemed ventilator dependent) whichever comes first. All patients will be followed to hospital discharge.
Consistent with our pilot trial design, we aim to assess feasibility metrics in the FAST Trial.
Primary outcome
The primary outcome will determine our ability to recruit critically ill patients into the trial. We will consider recruitment to be acceptable if on average, at least 1 to 2 patients per ICU are included per month.
Secondary outcomes
We will evaluate compliance with screening assessments (once vs . at least twice daily) conducted as per protocol, when feasible (i.e., criteria to return to full ventilation have not been met) and the potential for contamination. Similarly, we will assess compliance with the assigned SBT strategy (PS ± PEEP vs . T-piece). Compliance rates of >80% will be considered acceptable for screening frequency and SBT conduct. We will consider a contamination rate of <10% in the once daily strategy or between SBT techniques acceptable.
We will record practices related to sedation, analgesia, delirium, and mobilization in all treatment arms, using a checklist, to determine strategies that are infrequently utilized at the time weaning assessments and may require protocolization or detailed documentation in a future trial.
Tertiary outcomes
We will characterize clinician and institutional barriers to recruitment.
We will classify trial participants in both arms as requiring (i) simple, (ii) difficult or (iii) prolonged weaning using the Task Force definitions [21]. An estimate of the proportion of patients who can be extubated after a first SBT attempt will inform future sample size estimates.
We will obtain preliminary estimates of the impact of the alternative screening and SBT strategies on clinically important outcomes. We will include NIV (CPAP and bilevel) in calculating total duration of ventilation excluding intermittent nocturnal NIV after extubation (i.e., NIV used nocturnally or was likely required but not recognized prior to ICU admission). We expect that reintubation rates (primary safety outcome) will not exceed the average reported rate of 13% (3 -19%) [30].
Data management plan
The Coordinating and Data Management Centre will be the Applied Health Research Centre (AHRC) of the Li Ka Shing Knowledge Institute (www.ahrconline.com) of St. Michael’s Hospital. We will use an electronic data capture system Research Electronic Data Capture (RedCap; Vanderbilt University, Tennessee, USA) to randomize patients and for data management. The database includes logic checks and range checks for selected data values.
Since the FAST trial is being conducted to demonstrate feasibility, its goals will be primarily descriptive, not inferential. The clinical outcomes will be the outcomes of interest for the subsequent trial.
Primary analysis
We will report the number of patients included as a proportion of the number of eligible patients. We will report reasons for exclusion and document barriers to participation as proportions of the total number of patients screened for eligibility. We will report the number of patients included, on average, per ICU per month.
Secondary analysis
We will evaluate compliance with the assigned screening strategies by evaluating whether a single screening assessment was completed in the ‘once daily screening’ arm (yes/no) or whether two or more assessments were conducted in the ‘at least twice daily screening’ arm (yes/no). Similarly, we will assess compliance with the SBT strategy by evaluating whether SBTs were conducted based on treatment assignment using PS (yes/no) or T-piece (yes/no). Of importance, in this feasibility trial, we will record reasons why screening assessments were not completed, or SBTs were not conducted using the assigned strategies. We will evaluate compliance with screening frequency when criteria to return to full ventilation were not met. Further, we will exclude circumstances when it was not feasible to conduct assessments from this computation (e.g., patient not in the ICU, met criteria to return to an alternate mode of ventilation without spontaneous or triggered breaths etc.).
To assess whether patients are being optimized for weaning, we will report the proportion of practices used separately for sedation, analgesia, delirium management, and mobilization in screening assessments before the (i) first SBT and (ii) the first successful SBT. Similarly, we will record the proportion of practices used in screening assessment that led to an (iii) SBT preceding the first attempt at extubation and (iv) SBT preceding successful extubation.
We will compare clinical outcomes and complication rates (e.g., reintubation) between screening and SBT strategies using the Chisquare test (alternatively, Fisher’s exact test for expected values <5) and Student’s t-test (alternatively, the Mann-Whitney U-test, if normality assumptions are not satisfied) for binary and continuous outcomes, respectively. We will compare time to successful extubation (from randomization) using the log-rank test with censoring of deaths. Finally, we will describe the proportion of simple, difficult and prolonged weaning in both strategies using the Task Force on Weaning definitions [21]. We will consider p-values <0.05 to be significant.
The proposed study is novel in seeking to identify the optimal screening and SBT strategies to minimize patients’ exposure to invasive ventilation and its associated complications. It will provide valuable data regarding trial feasibility and preliminary estimates of the effect of the alternative weaning strategies. Only one weaning trial has been done in Canada [24] by members of our group. Establishing the optimal screening frequency and SBT technique is appealing to ICU clinicians because these interventions are sensible, low-risk, and represent an efficient use of current resources. Moreover, these interventions hold promise as strategies that could change clinical practice, enhance the care delivered to critically ill adults, and improve patient outcomes.
To address the concerns that elderly critically ill patients may experience more adverse events and are less likely to be enrolled in weaning trials due to comorbidities and treatment limitations, we conducted 2 parallel, multicenter, pilot screening frequency trials comparing once vs. at least twice daily screening in 100 elderly patients >65 years (SENIOR Trial; ClinicalTrials.gov NCT02243449) and 50 non-elderly patients <65 years (RELEASE Trial; NCT02001220) [26]. In the multicenter RELEASE (10 ICUs) and SENIOR trials (11 ICUs), we prioritized evaluation of screening frequency, recognizing that a ‘change in screening culture’ was warranted and allowed personnel in participating centers to use their preferred SBT technique. In addition, the parallel pilot trials enabled us to (i) evaluate our consent and enrolment processes, refine our inclusion and exclusion criteria, assess our randomization process and data collection procedures, (ii) assess protocol adherence, (iii) obtain preliminary estimates of effect of the alternative screening strategies on outcomes and (iv) use a staged approach to design and implement a large factorial trial. Based on recruitment in these pilot trials, we expect to recruit on average, 1 out of every 5 patients screened by research personnel, or approximately 2 patients per month per ICU. Both trials were completed in a timely manner (8 and 11 months, respectively) and had similar and high consent rates. The high consent rates likely reflect the low-risk and familiar interventions being evaluated and use of an altered consent model given the time sensitive nature of patient inclusion [25].
Through our pilot trials, we refined the eligibility criteria for the current FAST trial to identify the population of interest and enhance generalizability. Specifically, we revised and expanded the criterion excluding patients who already had undergone an SBT to also exclude patients who are already on SBT equivalent settings. This criterion is necessary to ensure that protocol-directed screening identifies patients for an SBT- a population that may benefit from more frequent screening [26]. We identified that more patients in the SENIOR trial were excluded due to age-related illnesses. Consequently, we refined the criterion that excluded patients who have evidence of a myocardial infarction within 24 hours of enrollment to enable patients whose serum Troponin level had peaked to participate in the FAST trial provided that the Troponin level is decreasing or the patient has undergone a revascularization procedure, and the attending physician has no concerns regarding ongoing ischemia. The FAST trial will inform the design of a planned future factorial design weaning trial by further refining recruitment estimates, identifying barriers to recruitment, and evaluating potentially important co-interventions that may require protocolization.
Careful consideration has been given to important aspects of the FAST study design to limit selection, identification, treatment, and performance bias in this necessarily unblinded weaning trial. To limit selection bias we will use a central randomization process with full allocation concealment. To limit identification bias, consistent with evidence from RCTs and meta-analysis, screening and SBTs will be led by RTs in participating ICUs in Canada and the United States. To limit identification bias and subjective assessments of weaning readiness in all arms, we will include the rapid shallow breathing index (f/VT,), measured on a standardized setting, in all screening assessments [31]. To identify potential factors that may result in performance bias in the future large scale weaning trial, we will record current practices in sedation, analgesia, and delirium management and the timing of mobilization before screening assessments using a checklist [32-39]. To enhance the generalizability of our findings, we will permit SBTs to be 30 -120 minutes in duration. Finally, to limit treatment bias, we provided guidance on (i) titration of ventilator settings, PEEP and FiO2 the (ii) use of NIV after extubation, (iii) reintubation, and (iv) tracheostomy [29].
Daily screening is not commensurate with the 24 hour care capability provided by respiratory therapists in many North American ICUs. Consequently, an important opportunity exists to screen patients more frequently, conduct more frequent SBTs, and reduce the time critically ill adults spend on invasive ventilation and in the ICU. Data from the FAST pilot trial will evaluate the feasibility and safety of conducting a multicentre, factorial design trial to compare alternative screening frequencies and SBT techniques.
We wish to thank the members of the Canadian Critical Care Trials Group for their methodologic advice and content expertise and Dr. Lauralyn McIntyre for her review of the protocol.
The FAST Trial is funded through an operating grant from the Canadian Institutes of Health Research.