Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2014) Volume 3, Issue 1
Nitrofurantoin is a commonly prescribed urinary antiseptic both for acute treatment and prophylaxis against recurrent urinary tract infections. It is known for its safety, efficacy, tolerability and cost-effectiveness. Rarely, nitrofurantoin can cause acute and chronic lung and liver diseases. Acute pulmonary toxicity due to nitrofurantoin is more common than its chronic form and is probably a hypersensitivity reaction to the drug. In contrast, the chronic pulmonary toxicity appears to be due to cumulative drug exposure leading to chronic inflammation and fibrosis and is therefore an irreversible process. What predisposes to the rare and severe form of acute pulmonary toxicity is unknown. In this case, it appears that renal impairment may have played a role as a predisposing factor.
<The majority of patients affected with nitrofurantoin pulmonary toxicity are elderly women [1]. The proposed mechanism of toxicity is either idiosyncratic oxydant-mediated tissue injury by nitrofurantoin metabolites causing depletion of cellular glutathione (chronic form) or by immunological response induced by nitrofurantoin metabolites acting as heptanes and resulting a hypersensitivity reaction (acute form) [2]. Acute and chronic hepatic toxicity similar in pattern to pulmonary toxicity have been reported. Clinical manifestations of nitrofurantoininduced pulmonary toxicity can be acute, sub-acute and chronic [3]. Acute presentation is the most common form and is characterized by fever, rash, arthralgia, non-productive cough, chest pain, and dyspnea within days to weeks after the exposure. Recurrence of acute toxicity has been described with rechallenge of nitrofurantoin in a patient who did not tolerate it initially [4,5]. Sub-acute presentations have more insidious onset of symptoms, with most cases having received nitrofurantoin for several weeks to months. Chronic presentation and pulmonary fibrosis is typically seen in patients on nitrofurantoin therapy for several months or years with usual presenting symptoms of progressive dyspnea, fatigue and cough. Fulminant pulmonary hemorrhage presenting with hemoptysis and respiratory failure has also been described [6]. Here we report an elderly female with subacute pulmonary symptoms after exposure to nitrofurantioin who succumbed to death from rapidly progressive respiratory failure.
Imaging finding is non-specific in nitrofurantoin induced pulmonary toxicity. A chest X-ray typically shows diffuse parenchymal changes and a CT scan shows bilateral ground glass attenuation [1]. Although Bronchoscopy with broncho alveolar lavage (BAL) is helpful in excluding infectious and neoplastic etiologies, the BAL findings usually are nonspecific and the diagnosis remains clinical. In the acute form, peripheral eosinophilia may be seen in up to 80% of cases and increased eosinophils in BAL can be seen in as high as 40% of cases. New onset of pulmonary symptoms, laboratory finding of eosinophilia along with history of drug exposure is highly suggestive of drug induced pulmonary toxicity. The prognosis for acute nitrofurantoin induced lung toxicity is excellent if the condition is recognized early and the drug is discontinued. The key is to suspect and recognize this entity early on prior to the development of pulmonary fibrosis and stop nitrofurantoin exposure and preserve the remaining lung function with the goal of reversing the lung damage that had already occurred. Rare fatalities have been reported both in acute and in chronic forms [7]. Apart from discontinuing the offending agent, there is no specific therapy. Only retrospective data are available regarding the value of using glucocorticoids and they are conflicting: some suggesting lack of efficacy to accelerate recovery [1] and some suggesting complete recovery after steroid therapy [8]. For severe form, it is probably reasonable to consider a therapeutic trial of steroid after ruling out infectious etiology or congestive heart failure.
An 82-year-old white female with past medical history of urinary incontinence and recurrent urinary tract infections (UTI) was admitted with progressive dyspnea, non-productive cough, and low grade fevers for three weeks. She had been started on nitrofurantoin 100 mg daily for prophylaxis of recurrent UTI six weeks prior to the presentation. Past medical history included moderate dementia leading to assisted living and hypertensive nephropathy with creatinine clearance of 40 mL/min (MDRD equation) one year prior to presentation. She had no exposure to tobacco or other environmental or occupational toxins. Relevant physical findings were temperature 38.5°C, respiratory rate 28/min, oxygen saturation 85% at room air and bilateral rales in the lungs. Laboratory tests were WBC 16, 500/mm3 with 80% neutrophils, 8% eosinophils, creatinine clearance 20 mL/min, and normal bilirubin and hepatic transaminase levels. A chest X-ray and a computed tomography scan (Figures 1 and 2) showed diffuse bilateral parenchymal and interstitial lung disease and ground glass attenuation. Transthoracic echocardiogram showed normal cardiac and valvular functions and B-type natriuretic peptide (BNP) level was within normal range. Sputum for gram stain and culture remained negative. Bronchoscopy with BAL showed acute alveolar and interstitial inflammation without evidence of infectious or neoplastic processes but no increased eosinophils were noted. Transbronchial lung biopsy was not performed in this frail and sick patient. In addition to symptomatic and supportive care (supplemental oxygen and non-invasive ventilation), she was treated with levofloxacin for probable atypical community acquired pneumonia and intravenous methylprednisone for suspicion of nitrofurantoin induced pneumonitis. Endotracheal intubation and mechanical ventilation was not considered respecting patient’s wishes. Unfortunately, the patient died from progressive respiratory failure in two weeks from the date of hospitalization.
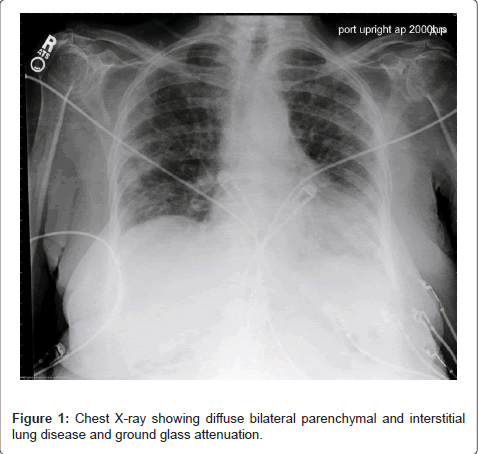
Figure 1: Chest X-ray showing diffuse bilateral parenchymal and interstitial lung disease and ground glass attenuation.
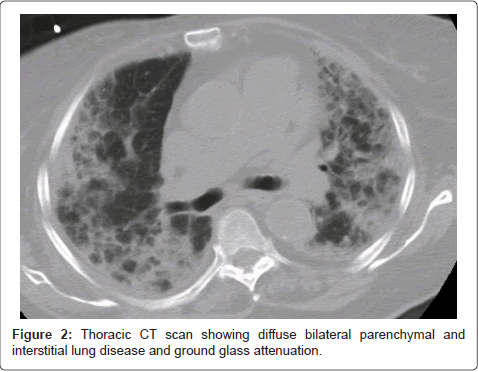
Figure 2: Thoracic CT scan showing diffuse bilateral parenchymal and interstitial lung disease and ground glass attenuation.
It is unknown what exactly predisposes some patients to develop nitrofurantoin pulmonary toxicity and why the toxicity can be very serious in a small fraction of patients. It has been reported to occur both at the treatment and at the prophylaxis dose including lower prophylaxis daily dose of 50 mg [8] suggesting a non-dosedependent mechanism of toxicity. It has also been described with continuous and with intermittent prophylaxis for UTI [8]. There are also published reports of acute and chronic concomitant pulmonary and hepatotoxicity; including a case of acute respiratory distress syndrome and hepatitis following a single dose of nitrofurantoin [9]. Two uniform risk factors that have been described are age (elderly) and gender (women). There remains a debate on renal insufficiency as the risk factor that predisposes a patient to pulmonary toxicity but it is a standard practice to avoid nitrofurantoin in patients with decreased creatinine clearance of <60 mL/min. Furthermore, majority (75%) of nitrofurantoin ingested is metabolized by liver and rest of it (25%) is excreted unchanged in the urine. Since nitrofurantoin and its metabolites are renally excreted and reduced renal function is common in the elderly patients, inadvertent toxic accumulation of nitrofurantoin and its intermediates/metabolites can occur in this population [10]. There is a possibility that reduced renal function may have predisposed this patient to this severe and fatal pulmonary toxicity. There may be a genetic susceptibility to nitrofurantoin induced pulmonary and liver toxicity. There is emerging literature on genetic polymorphisms on drug-metabolizing enzymes and human leukocytes antigens (HLA) in the pathogenesis of drug induced hypersensitivity, acute and chronic toxicity [11,12]. And finally, multiple factors including concomitant use of other drugs, pre-existing lung disease, sequela of prior pulmonary infections, nutritional and immune status of the host may play a role. Elderly patients tend to have decreased renal function either due to comorbidities such as diabetes and hypertension or due to age related loss of nephrons and therefore they should have creatinine clearance checked before this medication is started. Furthermore, patients with cognitive impairment cannot report side effects of drugs promptly and by the time it is obvious to others, the toxicity can become irreversible.
This case is also an example of system failure and a lost opportunity in part of ancillary providers (pharmacy or nursing) who usually remind prescribing providers of drug-drug interaction and need for dose adjustment for renal or hepatic insufficiency. It is also important to read packet insert (by prescribers, dispensers, care givers, and anyone involved in providing healthcare to the patients including patients themselves and their family members) which can provide valuable information on indications, contraindications and interactions. In the case of nitrofurantoin the package insert of Macrodantin (Proctor and Gamble Pharmaceutical, Cincinnati, OH, USA) clearly states “Anuria, oliguria, or significant impairment of renal function (creatinine clearance under 60 mL per minute or clinically significant elevated serum creatinine) are contraindications”) to nitrofurantoin.
Providers should maintain a high index of suspicion for new onset of pulmonary symptoms after prescribing nitrofurantoin especially in elderly women. Medical science has come a long way since the first report [5] of nitrofurantoin pulmonary toxicity was published in 1962 but many questions remain unanswered about the molecular basis of its toxicity and why some individuals are susceptible to severe form of toxicity. Nitrofurantoin toxicity can be a model for the study of drug induced hyper-acute, acute and chronic toxicity and organ damage. Further researches in this area are highly desirable.