Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2016) Volume 5, Issue 1
Maternal and child health information forms cradle human right, that allow mothers to access quality and reliable health care hence, decrease morbidity and mortality rates, aimed to be achieved in global goals number 3 and 17 of 2015 by 2030. Globally over 80% of community households have limited access to effective, reliable, efficiency and quality Maternal & child health information, especially in Sub Saharan Africa ( SSA), and depends solely on health professionals and community health workers (CHWs), as their main sources of health information, with large diversified society of demographic, socio-economic and socio-cultural factors. The aim of this study was to determine factors influencing accessibility of maternal & child health information. Specifically to determine how health professions and community health workers influence accessibility of maternal health information, investigate association that exists between source of maternal & child health information received and health practices and establish how demographic and social cultural factors influence utilization of maternal health & Child information among rural women in Kenya, using cross sectional and descriptive design. Cluster sampling design was used to identify study participants, mothers with children aged 0-11 months. Results showed that, health professionals remain main source of health information (46.2%) followed by community health workers (32.9%), in Kenya However, since CHWs are accessible and reliable sources in rural areas, they form most efficient community health linkages with health facilities, so it’s important to empower them for sustainable healthcare at community level.
<Keywords: Accessibility, Maternal health information, Sustainable, Empowerment, Global goal numbers
Study by Ahmad et al. [1], show that globally over 80% of community households have limited access to effective, reliable, efficiency and quality Maternal & child health information, especially in Sub Saharan Africa (SSA), and describe accessibility of maternal and child health information as the knowledge communicated or received concerning particular circumstances of preventive, curative or palliative health care. Health information plays a big role on reproductive health, child health and promotes integrated management of childhood illness (IMCI), which includes management five diseases of under five children: Malaria, pneumonia, Diarrhea, measles and malnutrition [2].
Individuals seek healthcare information from health professionals or community health workers, during chief’s Barazas or health posters for reasons ranging from health awareness on primary health care, health promotion such as screening, curiosity to self-diagnosis and treatment, [3]. Health information and capacity building help health seeking behaviors of individuals, majority of maternal mothers, feel empowered and more in control of their reproductive health and also address on both unmated and psychological needs of women at specific time of need [4]. It has also been shown that access to quality health care information leads to real improvements on reproductive health, in prevention of mother to child transmission (PMCT) in this era of HIV & AIDS pandemic [5]. Health information empower women to make informed choices and increase their perceptions in satisfaction of health provision towards primary prevention [6].
The challenge of not preventing or eradicating these avoidable or treatable conditions or diseases through disseminating maternal health and child information to households, using reliable and accessible sources, have led to majority of maternal and under five child deaths. For instance 536,000 maternal deaths occur worldwide in 2005, where by 99% (533,000) of these deaths, happened in Sub-Saharan Africa. In Kenya, majority suffer from illness and disability related to inaccessibility to affordable obstetric and gynaecological care, KDH, (2008-2009) [7], utilization of reproductive health and IMCI services for children below five years in managing malnutrition, measles, pneumonia and malaria illness, in most rural communities of Kenya, remains inaccessible, unaffordable and inefficient, due to prolonged poverty in vicious cycle [2].
Health professional and community health workers influence on accessibility of maternal & child health information among rural women on reproductive health
According to Wolfson [5], investing in women’s health will ultimately provide a win-win situation for development, empowerment, human rights equity and equality by using health providers or media health posters. Wolfson stresses that when a woman’s health is advanced and promoted it will definitely benefit families, children, husbands, elders and in-laws because women are the primary care givers in the home and indeed the primary caregivers in most societies. It is imperative therefore that they be adequately empowered with information to make the right decisions pertaining to their reproductive health. In rural settings in addition to taking care of nutrition for the family, a house wife is also expected to know basic health care to ensure that first aid to all family members is done, so if a family member gets sick she needs to act as a nurse if not as a doctor. This explains why world has much to gain by investing in women’s health. Women are the primary seekers of health information for their children of under fives and other family members as well as themselves [2].
Illiteracy and access to knowledge are two of the key problems that inhibit socio-economic development in developing countries. Rural women of reproductive age lack the vital or basic maternal health information they need to improve their health, and because most are illiterate, they cannot benefit from many educational methods. Furthermore, lack of electricity and poor roads isolate them in accessing various sources of maternal health information. In Ghana according to a Non Governmental Organization which did pilot test on the use of talk book in accessing health information in rural area in northern Ghana’ observed that most of these Organizations travel to villages where they share knowledge about health but fail to consider the population reached [6-8]. This method of delivering information is expensive costing US$20-$40 per trip. It is also inefficient because each visit occurs infrequently and covers various topics causing many community members to forget information that is not immediately applicable to them. This scenario calls for improvement to access to health knowledge to the rural woman, due to the fact that the rural woman of reproductive age has low or no education hence higher percentage in poor health status compared to urban women. In Nigeria one in 10 women read newspaper weekly compared with three in ten men [9]. This implies that most women of reproductive age have limited sources of maternal health information.
In Kenya Data reveals that proportion of illiterate women is double that of men [7], considering that more than half of the illiterate women are in rural areas. In mass media for example urban women have more access to all forms of mass media compared with their rural counterparts; For example only 16% of women in rural areas reads a newspaper at least once a week, compared with 49% of women in urban areas.69 percent of women in urban watch TV at least once a week while only (22%) do so in rural [7]. This implies that any maternal health information that leads to utilization of health services by the mothers will not reach to majority of the women in rural who are in dire need of it. Most men access to information compared to women at 46% and 24% respectively [7].
A report by Elain wolfson [5] who did a research in 7 districts in Kenya on ‘accessing health information in rural area on HIV/AIDS’; Found out from their study that these rural communities had no electricity or telephone lines as it is the case in many areas in Kenya. Solar powered equipment was used to allow health video shows and World Space receivers used to relay information even under a tree. It was these reasons that led the study to determine how health service providers and Chiefs barazas influence utilization of maternal health information among the rural households.
Association between source of maternal & child health information received and health practices among rural women of the reproductive health
The impact maternal health information from health service providers and mass media posters displays have increased the uptake trends in maternal health services, discussion of PMCT among women of reproductive age of which it was previously very difficult to break the silence in these matters in their social capital, after testing maternal health system in one area. They have begun to understand the importance of PMCT hence started to show willingness to attend clinic and dialogue about the risk of not attending clinic during pregnancy. There is also an increase in condom uptake in some of the field centers, and increased demand for voluntary counseling and testing services among these women who were previously very averse to the very mention of PMCT to promote primary preventions [6].
Elderly women and men participation in health issues has increased in these areas with bigger turnouts reported at community health meetings and health action days. While it is still too early to demonstrate improvement in health through the project activities, with these changes that are beginning to take place it is clear that if these continue there will be a definite impact on PMCT intake in these communities with the attendant improvement in health. It is important to note therefore that health information provided to women of reproductive age should be what they want, and to avoid dumping information on them Haris and fear [10].
Maternal health has emerged as global priority because of a great gap in the status of mother’s well being between the rich and the poor countries. Attention given to maternal health has been concentrated in reducing maternal mortality [11]. This has been reflected among the strategies in the millennium development Goal 5 on maternal health and goal number three on health and well being: Reducing maternal mortality by three-quarters by the year 2030 and goal number 17; Partnership of health and well being with other sustainable development goals which are mainly aimed at decreasing 536,000 maternal deaths that occur in every year in Sub Saharan Africa [12]. Studies show that women of reproductive age in Africa are still not given opportunity to make their own decisions as most of them have low education level and considered low status in the society compared to men. This has made it difficult for the women of reproductive age from Sub Saharan Africa to access maternal health information effectively hence lack knowledge on maternal health services and these justifies reasons for high maternal mortality in most of the African Content [13]. Low status of girls and women denies them the power to make decisions that affect their reproductive health [14].
This triggered the need for conducting this research to help in identify how the sources of maternal health information influence improved health practices among women of reproductive age in Kenya.
Demographic and social cultural factors influence utilization of maternal & child health information among rural women on reproductive health
Younger women were more likely to sort maternal health information from health facility compared to other age groups. This study is in agreement with a study done by Audiences cape, target groups for FP-MCH oriented campaigns, done in Tanzania reported that young women in rural areas, tend to have lower levels of access to mass media compared to other demographic groupings. However these findings are also different from those of Audio Scope [15], which found out that young women in rural areas tend to have lower levels of access to mass media compared to other demographic groupings.
Most of the younger women often feel free with the health professionals and also feel that they are reliable compared to other sources of maternal health information used by the older reproductive women. In this study socio economic factors were found to influence sources of maternal health information on health outcome among women.
Education was a significant finding on factors influencing sources of maternal health information among women of reproductive age in this study. This could be explained by the fact that majority of those who have gone to school were likely to get there source of information from health professional, CHW and media. This is supported by Mbagaya [16] who found out that parent’s schooling particularly that of the mothers is likely to influence their behavior in seeking health information for their children. The author further argued that the mother’s health seeking behavior was influenced by the number of years of schooling. The findings seem to indicate that education of a woman plays a big role in determining the source of information and action to take.
From this study is clear also that source of income of women is important in influencing decision making and accessing the sources of maternal health information freely and these improves their health status and cannot be assumed [17].
Occupation was found to have significance in influencing maternal health information among women. Similar findings are reported by Magadi [13] who found out that women who are employed tend to start antenatal care earlier. The authors argue that employed women are more knowledgeable on pregnancy and childbirth issues than the unemployed due to freedom of movement outside household. They also tend to get information on services available for pregnancy care during work from workmates. Women’s involvement in gainful employment is one of the important factors positively affecting the use of quality medical care to treat complications and also empowers women to take part in decision-making processes about health care in the family.
These findings are also supported by those of [14] in his study on barriers to equitable access to health information, who indicated that major barriers were lack of information workforce capacity, and the high cost of accessing up to date, timely, and relevant information.
It was these reasons that study intended to establish how Demographic and social Cultural factors influence utilization of maternal health information among rural women on reproductive age health in Kisumu [18,19].
Study design
Cross-sectional study design in mixed research of quantitative and qualitative methods of data collection on sources of maternal health information and health practices.
Study population
The study population consisted of rural women of reproductive age between 15-49 years who had lived in Bar B sub location for at least for the last six months and have children who are below one year in age.
Sampling design and sample size
Cluster sampling, was used to identify study participants who were women of reproductive age with children under one year in age. The sub location had a total of 5 villages, comprising Bonde, Gul, Wachara, Ndede and Geta with a total of 210 study participants. A register of women under reproductive age was used. This method ensured equal representation of participants in each cluster. This procedure was convenient since each cluster registered had equal chance of being included in the study.
Selection of study units
Community health workers were used as reference points to identify targeted households around it and selecting the first household with a child below one year while enumerators carried out data collection in the households identified by CHWs. The first household for enumeration was selected randomly. Selection of the second household from the first household was done systematically depending on the number of households identified with women with children below one year in a cluster (catchment area). Only one subject was enumerated per household. Where one or more study subjects meeting the inclusion criteria were encountered the household with the youngest child was enumerated.
Inclusion/Exclusion criteria
The primary target for the study was women of reproductive age with children aged below one year at the time of the study. In order to be eligible for this research, the women had to be residents of Bar B sub location, had full pregnancy with a child below 1 year, have lived in the area for at least 6 months, and most importantly they had to voluntarily accept participation in the research after being taken through the terms and conditions of the research.
Data collection methods and instruments
Quantitative data was obtained from women with children aged below1year and was collected using questionnaire. The questionnaire was designed to collect information on demographic factors, socio economic, cultural factors and sources of maternal health information.
Focus group discussion was used to collect qualitative data from the CHWs while Key Informant interview was used to collect qualitative data from the in charge of maternity ward in health facility, an NGO officer working in the area, CHEW of Bar B sub location and assistant chief in Bar B sub location area. FGD and KII were held validate the quantitative data and answer questions why and how.
Recruitment and training of research assistants
Three focus group discussion moderators and note takers were selected from professionals and 15 enumerators who were form four leavers and some are doing community health course in college were selected from the area to participate in household survey. The research team were people with experience in research procedures and knowledgeable of the local language, English and the study area. A pretest and amendment was done just before going to the field. Training included briefing on research process principles and ethics and data collection tools.
Data collection
Pilot test was administered on the questionnaire to ascertain the flow of the questionnaire, understanding of the tool and administer the questionnaire test capability of enumerators and determine time taken to administer the tool.
Quantitative data was collected for 3 days. The data collection team comprising of 12 enumerators met every day for briefing before the exercise on serializing the questionnaire and supervision of data collection was undertaken and cleaned at the end of each day. Closed ended structured questionnaire was used. The questionnaire was divided into sections as per the study objectives. The questionnaire was translated into the local language (Luo) by two independent translators. This was because the area is largely inhabited by the Luos.
Data processing and analysis
Data was entered and electronically analyzed with the use of statistical package for Social Scientist (SPSS) package version 16. Frequencies were used to determine the occurrences and distribution of the variables under study. Cross tabulations was used to determine the level of relationship of the variables that would correlate with each other. In order to ensure correct entry and analysis, cleaning was done from right immediately in the field and during running frequencies to identify wrong data entries and possible omissions. Prompt correction was done immediately such errors were detected.
Descriptive analysis was used to examine variables according to the study objectives using Bars, charts, tables, frequencies, percentages and graphs. First cross tabulations was used to find out the patterns in data, this was followed by determining significance of the relationship using chi square test (95% confidence interval).
Statistical tests of significance and validity were used to determine the level at which the study techniques and findings are within the expected standards. A report was then finally written to give detailed and complete account of the whole process. Feedback will be given to all relevant authorities and those who will be interested with the study findings.
Ethical considerations
Before undertaking the study the proposal was defended before the University’s research Scientists panel for critic and approval who gave out their recommendation which were included in the study. Consent was then sought from Great Lakes University of Kisumu academic research and ethics committee for its implementation by filling in the ethics form and observing all the requirements on safety and rights of the respondents.
Demographic characteristics of respondents
Table 1 presents the characteristics of the 210 women of reproductive age who accepted to be interviewed majority (39.5%) were of age group 20-24 years, followed by women aged 15-19 at (22.4%) a few (0.5%) were aged 45-49 years old. Among the respondents most (70.0%) of them were married, (22.9%) of the respondents were single and few (1.9%) were separated. Looking at the level of education among the women interviewed, majority (75.2 %) were primary school leavers, (18.6%) were secondary school leavers with only (1.9 %) went up to tertiary level. Considering the source of income of the respondents, majority (49.5%) of the respondents were small scale business, followed by (22.5%) who are in jua kali sector and very few (6.7%) are salaried. In religion most (55.2%) respondents were Protestants, (29.5%) belonged to indigenous, and a few (11.0%) were Catholics with only (1.9%) Muslims.
| Variables | No. of women (n) | Proportion of women (%) |
|---|---|---|
| Age-group (years) 15-19 20-24 25-29 30-34 35-39 40-44 45-49 Total |
47 83 50 17 8 4 1 210 |
22.4 39.5 23.8 8.1 3.8 1.9 .5 100.0 |
| Marital status Single Married Widowed Separated Total |
48 147 11 4 210 |
22.9 70.0 5.2 1.9 100.0 |
| Level of Education None Primary Secondary Tertiary Total |
9 158 39 4 210 |
4.3 75.2 18.6 1.9 100.0 |
| Source of income Salaried Small scale business Jua Kali Farming Total |
14 104 48 44 210 |
6.7 49.5 22.9 21.0 100.0 |
| Religion Catholic Protestant Indigenous Muslim Others Total |
23 116 62 4 5 210 |
11.0 55.2 29.5 1.9 2.4 100.0 |
Table 1: Demographic characteristics of the women of reproductive age.
Locally available sources of maternal health information
Main sources of maternal health information used by the women were health professionals (46.2%) and community health workers (32.9%). A few (8.1%) respondents used media as source of maternal health information. However significant relation exist, between sources of health information available locally and health practices, from health facilities (P value 0.01 95% CI 0.45, 0.86), as shown in Figure 1.
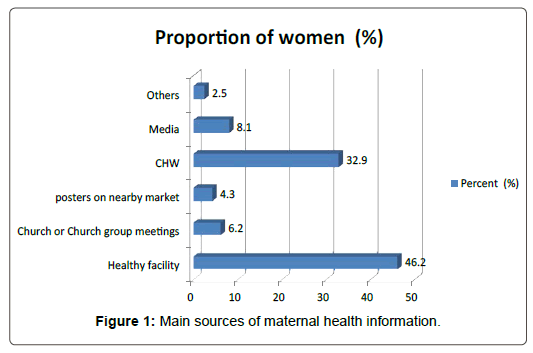
Figure 1: Main sources of maternal health information.
Main sources of maternal health information by health practices
Mothers, were asked about significance attached to their sources of information and health practices exist for instance, antenatal care, attendance for four or more times, most respondents (66.7%) got information mainly from CHW followed by those who used health facility (P value 0.2 95% CI 1.3, 3.7), as shown in Table 2.
| Main source of Maternal health information | No of times attended ANC | Total N (%) | ||
|---|---|---|---|---|
| 1-3(times) N (%) | 4+(times) N (%) | Don't Know N (%) | ||
| Healthy facility Church or Church group meetings posters CHW Media Others |
26(26.8) | 63(64.9) | 8(8.2) | 97(100.0) |
| 5(38.5) | 6(46.2) | 2(15.4) | 13(100.0) | |
| 2(22.2) | 6(66.7) | 1 (11.1) | 9(100.0) | |
| 20(29.0) | 46(66.7) | 3(4.3) | 69(100.0) | |
| 8(47.1) | 7(41.2) | 2(11.8) | 17(100.0) | |
| 4(50) | 0(0.0) | 1(50.0) | 5(100.0) | |
| Total N (%) | 65(31.0) | 128(61.0) | 17(8.1) | 210(100.0) |
Table 2: Sources of maternal health information by ANC visit.
| An na yudo wach mar dhi e clinic kuom nyamrerwa moro modak ibath dalawa, eka ne achako dhi e clinic. FGD discussants in Geta and Bonde, 23th of June 2015. |
(That I got information from one the CHW who lives close to my house who told me that I should go to clinic now that am expecting that is when I started going to clinic)
| a friend of mine told me that since you are expecting it is important to go to hospital so that they find out how the baby is sleeping in the womb because these people are not allowed to deliver at home FGD discussants in Ndete 24th of June 2015. |
| An aparo ni onego wayud weche nyuol koa kuom nurses kata nyamrerwa kata ka oluong puonj kamoro to ber ka wadhi winjo FGD discussant in Wachara, 24th of June 2015. |
(I think we should get maternal health information from the nurses and CHWs or when there is education day then we should attend)
Sources of maternal health information by place of delivery
Most of the women who delivered in hospital got information from posters (77.8%), followed by those who got information from the churches (76.9%) those who got information from health facility were (74.2%). Community health workers were (59.4%) media was used by (58.8%) respondents, the least source was among those who delivered in hospital was mobile publicity events at (50.0%). Chance of getting information from place of delivery was more reliable with (P value 0.3, 95% CI 2.0, 3.8)
Association of maternal health information obtained and quality of health service received
Relationship between source of maternal and child health information received and health care provided by service providers were effective and efficiency with (95% CI 2.8, 6.9) from health professionals, community health workers, and media.
Influence of socio strata in delivery of maternal health information in the society
When asked to mention the main source of efficient and reliable maternal health information from the health facility were most (52.9 %) used by women aged 30-34 followed by CHW (34.9%) preferred by women aged 20-24 years.
Women aged 35-39 as mentioned by CHW were main source of maternal health information in rural areas with statistical significantly (P value 0.02 95%, CI 1.3, 1.4)
Marital status as an attribute source of maternal health information in rural areas
According to the study findings the married were more (49.7%) likely to receive maternal health information from health professional, followed by the widowed (45.5%) who used CHWs as source of maternal health information and only (41.7%) single use health facility the separated also preferred CHWs as their main source of maternal health information. There was no significant relation in source of maternal health information by marital status (P value 0.000, 95% CI 0.2, 0.3).
Level of education
From Table 3, respondents who went to school up to secondary and tertiary level mostly preferred health professionals at (59.0.0%) and (50.0%) respectively as their main source of information followed by CHW at (25.6%) and (25.0%) respectively. Level of education statistically significantly influenced source of quality maternal $ child health information (P value .0.5, 95% CI 3.3, 8.1).
| Education level | Source of Maternal health information | Total N (%) | |||||
| Healthy facility N (%) | Church or Church group meetings N (%) | posters on nearby market N (%) | CHW N (%) | Media N (%) | Others N (%) | ||
| None | 4(44.4) | 1(11.1) | 0(.0) | 3(33.3) | 0(0) | 1(11.1) | 9(100.0) |
| Primary | 68(43.0) | 8(5.1) | 7(4.4) | 55(34.8) | 17(10.8) | 3(1.8) | 158(100.0) |
| Secondary | 23(59.0) | 4(10.3) | 2(5.1) | (10(25.6) | 0(.0) | 0(0) | 39(100.0) |
| Tertiary | 2(50.0) | 0(.0) | 0(.0) | 1(25.0) | 0(.0) | 1(25.0) | 4(100.0) |
| Total N (%) | 97(46.2) | 13(6.2) | 9(4.3) | 69(32.9) | 17(8.1) | 5(2.5) | 210(100.0) |
Table 3: Level of education and source of maternal & child health information.
Accessibility to stable source of income
Source of income was significantly influential in determining source of maternal health information. In this study most (50.0%) of the people in Jua kali sector preferred health professionals, followed by small scale business who closely preferred health professionals and community health workers (46.2%) and (40.0%) respectively. The salaried also used (42.9%) health professionals as source of maternal health information.
Irrespective of the source of income health professionals remain the main source of maternal health information for the respondents, Source of income positively influenced health seeking behaviors among respondents (P value 0.46, 95% CI 0.52, 0.94).
Distance from health facility
Respondents who live closer (6-15 minutes’ walk) the hospital got most (87.7%) of the maternal health information from the hospital compared to those who came from far (35.9%) those who came from far (1hr and over) preferred CHW as main source of maternal health information. Interestingly those who come closest to the health facility preferred health facility and CHWs in equal measures as sources of maternal health information.
Distance from the source and distance from the market centre had no relationship to source of health facility (P value 0.01, 95% CI 0.01, 0.02)
| ‘Karwa kama wadakie ka yoo madhi espital ok bor ahinya makmana ni mtokni onge koro ok inyal chopo piyo mamiyo nikech pikipiki ngenygi onge licence ok nyal chopo kuro.’’FGD discussant in Bonde, 24th of June 2015. |
(In this our region the road to hospital is not very far but the problem is that vehicles a very few so you can’t reach the hospital as fast, the motorcycles also can’t reach there at night because they don’t have license).
Religion
Results from Table 4 show, most Muslims preferred health facility as source of maternal $ child health information, like the Protestants then followed last by Catholics. Religion by source of maternal health information did not have any significance in preferred source of maternal health information according to this study. (P value 0.01, 95% CI 0.01, 0.02)
| What is your religion | Main source of Maternal health information | Total N (%) | |||||
|---|---|---|---|---|---|---|---|
| Healthy facility N (%) | Church or Church group meetings N (%) | posters on nearby market N (%) | CHW N (%) | Media N (%) | Others N (%) | ||
| Catholic | 10(43.5) | 0(.0) | 1(4.3) | 8(34.8) | 3(13.0) | 1(4.3) | 23(100.0) |
| Protestant | 54(46.6) | 10(8.6) | 6(5.2) | 38(32.8) | 7(6.0) | 1(0.9) | 116(100.0) |
| Indigenous | 26(41.9) | 3(4.8) | 2(3.2) | 21(33.9) | 7(11.3) | 3(4.8) | 62(100.0) |
| Muslim | 4(100.0) | 0(.0) | 0(.0) | 0(.0) | 0(.0) | 0(0) | 4(100.0) |
| Others | 3(60.0) | 0(.0) | (.0) | 2(40.0) | 0(.0) | 0(0) | 5(100.0) |
| Total N (%) | 97(46.2) | 13(6.2) | 9(4.3) | 69(32.9) | 17(8.1) | 5(2.5) | 210(100.0) |
Table 4: Religion by source of maternal $ child health information.
| A neighbor belonged to a religion which didn’t allow its members to go to clinic so she didn’t go to hospital when she got pregnant but the child died because she was weak but after the third born she went to hospital and the child is now healthy their religion did not allow her because they believed the saved don’t go to hospital. |
Discussion
The findings from this study indicate that health professionals and CHWs were,most reliable and accessible sources of maternal health information.
| These days it is easy in the village because as CHW we have our household that we take care of and we know the status of all of them so the pregnant ones we advice, so getting information is easy so life of today we can say CHW have helped people. We have support groups so we give them brochures through support group to read. These days are not like old days like our generation. KII interview and FGD discussants in Geta, 23 of June 2015. |
However this is in contrast with findings of O’Keefe [8], which reported that media source is often the most important source of information, especially television plays a significant role in providing health information. A study by Obermeyer in Morocco and Tunisia also indicated that watching television weekly is associated with an increase in the likelihood of both prenatal care and hospital delivery
Interestingly in a survey carried out by Wafula [15], in Kenya namely Trans-Nzoia District and Umlalazi District in South Africa on sources of health information amongst rural women, results showed that family and friends were the main sources of maternal health information in Kenya which is a contrast to findings of this study which found out that family and friends were the least sources of maternal health information.
Source of maternal health information influenced health practices according to this study. This is in the agreement with a study by Lemerani Marshal on determinants of timely antenatal visits a case study of Mitundu Hospital in Lilongwe District in Malawi who found out that media information influenced antenatal visit followed by health professionals.
The results are also similar to a study by Benjamin-Garner [9], which demonstrate how source of income influence uptake of maternal and child health information among reproductive aged mothers, more effectively and efficiently.
The main sources of maternal health information are health professionals (doctors and nurses) and community health workers who are the main link of the community households with health facility. Socio economic factors, like level of education and source of income, strongly influences the uptake of maternal and child health information.